Mohammad Amini1, Ankie M. Harmsze2 and Ron A. Tupker1
Departments of 1Dermatology and 2Clinical Pharmacy, St Antonius Hospital, Nieuwegein, The Netherlands



Mohammad Amini1, Ankie M. Harmsze2 and Ron A. Tupker1
Departments of 1Dermatology and 2Clinical Pharmacy, St Antonius Hospital, Nieuwegein, The Netherlands
Hyperhidrosis is a common ailment, which is accompanied by a low quality of life. There are many current treatment options. The aims of this study were to investigate: (i) the characteristics of sweating in patients referred for hyperhidrosis; (ii) their quality of life, using the Dermatology Life Quality Index and the Hyperhidrosis Disease Severity Scale; and (iii) their estimation of efficacy of the treatments given, using a patient’s global assessment score and the quality of life scores. In 47 of 94 patients (50%) responding to the questionnaires, hyperhidrosis was confined exclusively to the axillae. In 21 (22%) of the patients, sweating in the axillae was combined with sweating of the hands and/or feet, face or other, more widespread, regions. Fifteen patients (16%) had generalized hyperhidrosis. In half of all cases, sweating occurred in attacks. Attacks were mostly triggered by warmth, exercise, emotions, or had no apparent cause. Quality of life was low in all cases. All treatments improved quality of life. Key words: hyperhidrosis; quality of life; antiperspirants; iontophoresis; botulinum toxin; oxybutynin.
(Accepted December 28, 2007.)
Acta Derm Venereol 2008; 88: 356–362.
Ron A. Tupker, Department of Dermatology, St Antonius Hospital, PO Box 2500, NL-3430 EM Nieuwegein, The Netherlands. E-mail: r.tupker@antonius.net
Hyperhidrosis is defined as excessive sweating, beyond what is necessary to maintain thermal regulation (1). It is important to distinguish focal forms (axillary, hands, feet, craniofacial) from generalized forms (1). There is a current revival of interest in this condition due to new treatments with high efficacy (2–5). Furthermore, it has been found recently that hyperhidrosis is a common disease for which most patients do not seek medical advice because they do not appreciate the condition as a disease (6). Finally, hyperhidrosis represents a disease with a severe psychosocial impact (4, 6, 7).
There are many current treatment options for hyperhidrosis, including local antiperspirants, tap water iontophoresis, botulinum toxin injections, surgical removal of overactive sweat glands, systemic anticholinergics and endoscopic transthoracic sympathectomy (8, 9). Each therapy has its advantages and disadvantages, which led to the development of treatment algorithms for the different sites of focal hyperhidrosis (9).
The heavy quality of life burden of hyperhidrosis can be evaluated by means of validated questionnaires (6, 7). These questionnaires are pre-eminently useful as instruments to monitor the effectiveness of various treatments.
The aims of this study were to investigate retrospectively the following items in patients with various types of hyperhidrosis who have attended our dermatological clinic over a period of 4 years: (i) the characteristics of their sweating; (ii) their quality of life, using the Dermatology Life Quality Index (DLQI) (10) and the Hyperhidrosis Disease Severity Scale (HDSS) (6); (iii) furthermore, the patient’s estimation of efficacy of the treatments given was monitored using these quality of life instruments.
MATERIALS AND METHODS
A search was performed of the digital database of all letters sent to the patient’s general practitioners using the terms “hyperhidrosis” or identical Dutch synonyms, for the period January 2001 to May 2005. This search yielded 126 patients with hyperhidrosis. A letter explaining the aim of the study was sent to all 126 patients. Four questionnaires were sent, as described below.
Characteristics of hyperhidrosis
The following characteristics were assessed: duration of hyperhidrosis; location; whether it was a continuous complaint or occurred in attacks; if in attacks, what was the triggering factor (e.g. emotion, heat, exercise, food, occurs spontaneously, other); whether it occurred in the day time or at night; accompanying complaints; use of tobacco, alcohol, coffee, hot spices, and their relationship with the complaints; diseases (acute and chronic infections, hyperthyroidism, diabetes mellitus, menopause, hormonal disease, gout, neurological diseases, other disease), and their relationship with the complaints; use of medication, and their relationship with the complaints. The diagnosis was generalized hyperhidrosis if the areas included other locations than those involved in focal hyperhidrosis (e.g. axillary, hands, feet, craniofacial).
The impact of hyperhidrosis on daily life was assessed with the DLQI (10) and the HDSS (6).
The effects, side-effects and impact of the side-effects of the different treatments
These were determined as follows. A patient’s global assessment score was used to monitor the effect of the treatment. In this scoring system, 0 = poor response (no or only minor effect); 1 = moderate response; 2 = good response; and 3 = excellent response. The side-effect impact score also had 4 grades, 0 = no impact; 1 = low impact; 2 = moderate; 3 = severe.
As antiperspirants the following preparations were prescribed: 20% aluminium chloride solution (Pharmacopoeia of Dutch Pharmacists (PDP)), 15% aluminium hydroxychloride solution (PDP), 20% aluminium chloride hexahydrate solution (PDP) or SyNeo5® (T. Brunner Hygiene, Schlierbach, Germany), an unspecified over-the-counter preparation with aluminium chloride and aluminium chlorohydrate as the active ingredients.
For botulinum toxin type A, Botox® (Allergan, Inc. Irvine, USA) was used in the majority of patients. Botox® 100 U was diluted in 8 ml of 0.9% sterile saline and injected intradermally at about 50 sites per axilla (or foot), using a 0.5 × 16 mm, 25G 5/8” needle. In 3 patients, Dysport® (Beaufour Ipsen, Biotech, Paris, France) 500 U was diluted and administered similarly.
Tap water iontophoresis was given 3 times weekly for 10 min using Hidrex® GS (Hidrex GmbH, Wuppertal, Germany). The direct current strength was slowly increased, guided by the occurrence of tingling sensations. The maximal strength was 30 mA. The total treatment duration varied between 6 and 10 weeks. When this therapy was successful, patients were advised to purchase this instrument themselves.
For subcutaneous curettage, a 6-cm incision was made in the axilla. Metzenbaum scissors were used to undermine the entire area of hyperhidrosis. Thereafter, the undermined area was curetted using a sharp gynaecological curette (Lawton 53470).
The antimuscarinic drug, Dridase® (oxybutynin 2.5 mg; Pharmachemie, Haarlem, The Netherlands) was prescribed 3 times daily.
Statistical analysis
Data are expressed as mean values ± standard deviation (SD). Data were analysed using the two-sided paired Student’s t-test. In case data were not normally distributed the two-sided Wilcoxon signed-rank test was used. Differences with p < 0.05 were considered statistically significant.
RESULTS
Ninety-four out of the 126 patients (75%) responded to the questionnaire, of which 64 patients responded after one or two telephone reminders. The majority of the 32 non-responders had an unknown address.
Patient characteristics
Table I summarizes the patient characteristics, classified by anatomical location of the hyperhidrosis. In 47 patients, the axillae were the only locations of hyperhidrosis, and in 11 and 4 patients axillary hyperhidrosis was combined with hyperhidrosis of the hands and/or feet, and face, respectively. In 17 patients, sweating was restricted to the hands and/or feet. Fifteen patients exhibited a more widespread pattern of hyperhidrosis, not (only) confined to the areas of focal hyperhidrosis. In 6 of these patients, the axillae were involved. The mean age of patients with generalized hyperhidrosis was higher than that of the other patient groups. In this group there was a higher co-morbidity and use of medication. In only one case, medication (paroxetine) was judged as the cause of (in this case) generalized hyperhidrosis, based on temporal relationship. The patients did not observe a relationship between the onset of hyperhidrosis and diseases or conditions. Diabetes mellitus was found in 5 patients, of whom 4 had generalized hyperhidrosis. Hypothyroidism was present in 3 patients with the focal form, as was the case for 2 patients with neurological ailments. Other diseases were present in 10 patients with focal, and 6 patients with generalized, hyperhidrosis.
Table I. Patient characteristics of various hyperhidrosis locations and DLQI/HDSS before and after therapy
| Hands +/– feet (n = 17) | Axillae (n = 47) | Axillae + hands +/– feet (n = 11) | Axillae + face (n = 4) | Generalized (n = 15) | |
| Female/male | 6/11 | 34/13 | 10/1 | 1/3 | 11/4 |
| Age, mean (SD) | 30.6 (11.21) | 29.5 (8.78) | 25.6 (7.08) | 28.8 (12.23) | 48.5 (20.72) |
| Age of onset, mean (SD) | 15.7 (11.37) | 20.6 (8.29) | 15.4 (7.61) | 16.8 (13.94) | 40.0 (21.45) |
| Family history* | 2 | 16 | 5 | 1 | 2 |
| Continuous | 11 | 25 | 7 | 0 | 5 |
| Attacks (total), triggered by†: | 6 | 22 | 4 | 4 | 10 |
| Emotion | 1 | 10 | 0 | 1 | 2 |
| Warmth/exercise | 4 | 15 | 1 | 3 | 8 |
| No reason | 1 | 10 | 5 | 3 | 7 |
| Daytime | 7 | 33 | 5 | 0 | 6 |
| Night-time | 0 | 0 | 0 | 0 | 1 |
| Day and night | 10 | 14 | 6 | 4 | 8 |
| DLQI before therapy, mean (SD) | 9.24 (5.08) | 10.98 (4.51) | 12.91 (2.95) | 15.75 (5.62) | 12.27 (6.76) |
| HDSS before therapy, mean (SD) | 1.71 (0.92) | 2.15 (0.72) | 2.18 (0.60) | 2.75 (0.50) | 2.2 (1.01) |
| DLQI after therapy, mean (SD) | 3.59 (2.58) | 1.98 (2.94) | 5.09 (3.78) | 8.5 (11.21) | 3.6 (4.40) |
| HDSS after therapy, mean (SD) | 0.6 (0.74) | 0.58 (0.78) | 1.11 (0.60) | 1.25 (1.5) | 0.77 (0.83) |
†More than one trigger factor may be present in the same patient.
SD: standard deviation; DLQI: Dermatology Life Quality Index; HDSS: Hyperhidrosis Disease Severity Scale.
*Positive when present in first- or second-degree relatives.
The sweating had a continuous pattern in most of the patients with palmoplantar hyperhidrosis, whereas sweating in attacks was seen in the majority of generalized hyperhidrosis. In axillary sweating, half of the patients complained of sweating in attacks. The attacks were mostly triggered by warmth and exercise, but might also occur with no apparent reason. Emotional sweating was claimed as a reason in a minority of patients. Many patients suffered from sweating in the daytime only, especially when the problem was located in the armpits, whereas slightly fewer patients also had night-time sweating. Tobacco was claimed as a provocative factor by one out of 28 patients using tobacco. For alcohol, coffee and hot spices these figures were 1 out of 20, 3 out of 60 and 2 out of 8, respectively.
The DLQI before treatment tended to be higher in the generalized form and when sweating in the armpits was combined with sweating in other locations (see Table I). The same holds true for the HDSS, although the latter had also a high value in patients in whom the sweating was solely axillary.
Efficacy of treatments
In all location groups, scores for DLQI and HDSS decreased after therapy (see Table I). The type of therapy varied between the different location groups (Fig. 1). In the hands and/or feet group, 10 out of 17 (60%) patients were treated with iontophoresis, and 6 (35%) with antiperspirants. Antiperspirants were used in about 25% of patients with a form of axillary hyperhidrosis. In total, 29 patients were treated with antiperspirants, of whom 12 were given 20% aluminium chloride solution, 3 were given 15% aluminium hydroxychloride, 8 were given 20% aluminium chloride hexahydrate, and 6 were given SyNeo5®. Botulinum toxin injections were given in the majority of patients with axillary hyperhidrosis. Botulinum was injected only 2 times in another location than the axillae, namely in the soles. Curettage of axillary sweat glands was performed in 4 patients. Oxybutynin was given to 11 patients with generalized hyperhidrosis. In 2 of these patients, the dosage of oxybutynin was adjusted to 5 mg 3 times daily, since the effect of 2.5 mg 3 times daily was unsatisfactory.
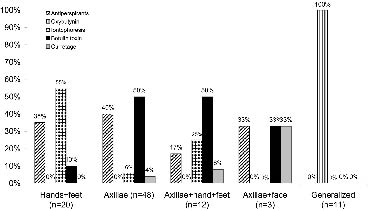
Fig. 1. Types of therapy in different locations. For each location the frequency of the type of therapy is denoted as a percentage. Note that the total percentage in each location is 100.
When a classification was made by type of therapy, scores for DLQI and HDSS also decreased in all treatments (Table II). The number of patients who judged their treatment as “good” or “excellent” for the various treatment modalities is shown in Table III. The mean duration ± SD of effect in botulinum toxin therapy was 5.9 ± 4.24 months. No difference was noted between the efficacy of Botox® vs. Dysport®, but the Dysport group was too small (n = 4) for a proper comparison. In the botulinum toxin group, more patients had previous therapy, mostly in the form of antiperspirants, compared with the groups treated with antiperspirants or iontophoresis (Table III).
Table II. Efficacy of different treatments evaluated by Dermatology Life Quality Index (DLQI) and Hyperhidrosis Disease Severity Scale (HDSS). Mean (SD) values before and after treatment.
| Treatment | DLQI | HDSS | ||
| before | after | before | after | |
| Antiperspirants | 8.9 (4.91) | 3.10 (3.46)* | 1.88 (0.86) | 0.85 (0.78)* |
| Botulinum toxin | 12.91 (4.33) | 2.61 (5.12)* | 2.31 (0.59) | 0.5 (0.76)* |
| Iontophoresis | 10.00 (4.18) | 4.40 (4.45)* | 1.73 (0.88) | 0.87 (0.83)* |
| Curettage | 11.50 (1.73) | 1.75 (2.06) | 2.5 (0.58) | 1.0 (1.41) |
| Oxybutynin | 13.73 (6.04) | 4.36 (4.70)* | 2.4 (0.84) | 0.9 (0.88) |
SD: standard deviation.
*p < 0.05, compared with pre-therapy value.
Table III. Characteristics of various treatments
| Antiperspirants (n = 29) | Botulinum toxin (n = 33) | Iontophoresis (n = 17) | Curettage (n = 4) | Oxybutynin (n = 11) | |
| Previous therapies | |||||
| Antiperspirants | 8 | 20 | 2 | 1 | 0 |
| Iontophoresis | 0 | 1 | 0 | 0 | 0 |
| Botulinum toxin | 0 | 0 | 0 | 2 | 0 |
| Other systemic medication | 0 | 0 | 0 | 0 | 6 |
| No therapy | 17 | 9 | 15 | 1 | 5 |
| Unknown | 4 | 3 | 0 | 0 | 0 |
| Side-effects of current treatment | |||||
| Pruritus | 3 | 1 | 1 | 0 | 0 |
| Erythema/irritation | 12 | 0 | 1 | 1 (infection) | 0 |
| Pain | 0 | 1 | 0 | 1 | 0 |
| Dry mouth | 0 | 0 | 0 | 0 | 6 |
| Urination obstruction | 0 | 0 | 0 | 0 | 3 |
| Abdominal complaints | 0 | 0 | 0 | 0 | 4 |
| Lassitude | 0 | 0 | 0 | 0 | 2 |
| Other | 1 | 0 | 0 | 1 (hyperhidrosis back and hands) | 1 (dizziness) |
| None | 13 | 31 | 15 | 1 | 0 |
| Side-effect impact score* | 1.54 | 0.5 | 1 | 1 | 1.64 |
| Stopped† (n) | 5 | 0 | 0 | Not relevant | 3 |
| No/moderate effect (n) | 18 | 6 | 5‡ | 1 | 3 |
| Good/excellent effect (n) | 11 | 27 | 12§ | 3 | 8 |
*Average side-effect impact score only in patients with side-effects.
†Number of patients who have stopped because of the side-effects.
‡3 cases had iontophoresis for axillary hyperhidrosis.
§1 case had iontophoresis for axillary hyperhidrosis.
Side-effects of treatments
In the groups treated with botulinum toxin and iontophoresis, the numbers of patients experiencing side-effects was surprisingly low (Table III). Five out of 29 antiperspirant-treated patients had stopped this treatment because of side-effects, and 3 out of 11 patients who were treated with oxybutynin (Table III).
DISCUSSION
This retrospective study mirrors the frequency distribution of the location of hyperhidrosis in a group of patients seen in a dermatological practice. In 47 (50%) of the patients, hyperhidrosis was confined exclusively to the axillae. In 21 (22%) of the patients, sweating in the axillae was combined with sweating of hands and/or feet, face or other, more widespread regions. In 17 patients (18%) the problem was connected only with the hands and/or feet, whereas 15 patients (16%) suffered from generalized hyperhidrosis. A large-scale prevalence study showed that 2.8% of the population in the USA has hyperhidrosis, of which 50.8% has axillary hyperhidrosis (6). Other locations were not evaluated. A recent retrospective study on 508 patients addresses the issue of location and other patient characteristics (11). Seventy-three of their patients had axillary involvement, which was combined or not with other sites. The frequency distribution in that study may be biased by the fact that it was performed on patients referred for consideration of botulinum toxin therapy (11). To our knowledge, our report is the first study that gives a better insight into the frequency distribution of various locations of hyperhidrosis, since it is based on the patient population that visited a secondary referral outpatient clinic in which several therapeutic options are offered. However, even our population is selected, since patients are directed by their general practitioner because of insufficient effect of the initial therapy. It is possible that the group with axillary hyperhidrosis is over-represented in our study because of the public awareness of the availability of botulinum toxin therapy.
The patients described in our study fulfil most of the criteria for primary focal hyperhidrosis given by Hornberger et al. (9), with the exception of the group with generalized hyperhidrosis. They defined primary focal hyperhidrosis as “focal, visible, excessive sweating of at least 6 months duration without apparent cause, with at least two of the following characteristics: bilateral and relatively symmetric; impairs daily activities; frequency of at least one episode per week; age of onset less than 25 years; positive family history; cessation during sleep” (9). In our patients with focal hyperhidrosis, no indication of the causes of secondary hyperhidrosis were present. In the group with generalized hyperhidrosis, the mean age was higher, as was the occurrence of co-morbidity and use of medication. In only one case, medication with a selective serotonin reuptake inhibitor antidepressant (paroxetine) was judged as the cause of hyperhidrosis, based on temporal relationship. In all other cases, no cause could be found, and therefore all other cases were designed as “primary”. Hurley (12) distinguishes neural and non-neural causes of hyperhidrosis. Neural causes are further subdivided into cortical (caused by emotions), hypothalamic, medullary, spinal and axon-reflex dependent. Palmoplantar and axillary hyperhidrosis are grouped under the cortical forms, since emotional factors are the presumed eliciting influences (12). Emotional stimuli were recognized as the predominant activating factors in axillary (13) and palmoplantar hyperhidrosis (14) patients. In contrast, hypothalamic hyperhidrosis is postulated to be elicited by thermoregulatory influences, such as exercise, infection and metabolic diseases (12). In our patient population, however, attacks were mostly triggered by warmth or exercise, or had no apparent cause, whereas emotions were noted as a factor in the minority of patients. Several patients claimed both emotions and warmth/exercise as eliciting factors. Moreover, a majority of patients, especially in the focal forms, feel that their sweating has a continuous pattern, e.g. without attacks. These aberrant findings may be interpreted as being caused by recall bias (see below). Furthermore, some patients may have another opinion about the definition of “continuous” and “attacks”. In a recent study using a daily subjective evaluation scale, it was found that the majority of palmar hyperhidrosis patients had a large variation in sweating, which was triggered by stress or exercise (15). In contrast, some patients had a consistently high level of sweating (15). Based on these and our results, we are convinced of the fact that “thermoregulatory” factors are at least as important in focal hyperhidrosis as emotional factors, that these different factors can co-exist, and that the distinction between cortical and hypothalamic forms is not realistic. Another striking finding in our study is the fact that sweating occurred also at night-time in all patient groups, which is in opposition to the criteria for primary focal hyperhidrosis set out by Hornberger et al. (9). According to Hurley (12), emotional sweating is always diurnal, whereas thermoregulatory sweating may be diurnal or nocturnal. In our view, emotions do not stop at night, and may be responsible for the night-time sweating in some of our patients, as may warmth and other (thermoregulatory) factors.
The average DLQI scores before treatment varied between 9.24 (palmoplantar group) and 15.75 (axillae combined with face). These values correspond to those cited in the literature (7, 16, 17). Low quality of life was also noticed, as monitored by means of the Hyperhidrosis Impact Questionnaire (4, 6). It is known that the symptoms of hyperhidrosis can manifest differently for the various areas affected, such as soiled clothing, paperwork or shoes, and wet handshakes, leading to limitations in work and leisure, and psychological distress (12). A new finding however, is the severity of its impact in a large population having axillary hyperhidrosis, as manifested by high HDSS scores (6). Lear et al. (11) had noted HDSS values of 3 and 4 (corresponding to “barely tolerable” and “intolerable”, respectively) in the majority of their patients, irrespective of site. Our study demonstrates that HDSS scores were not as high as found in the latter study, and tended to be lower, especially in patients with exclusively palmoplantar forms. The reason for the lower HDSS values in our patient group might be a selection phenomenon, as our outpatient clinic is a secondary referral institute.
It is a striking finding that in all treatment groups an improvement of quality of life was observed. This can be explained partly by selection. Most patients to whom antiperspirants were given had no previous therapy, in contrast to patients who were treated with botulinum toxin. Another factor explaining the patient’s satisfaction with their current treatment may be recall bias and placebo effects. These are known disadvantages of questionnaires. Recall bias may be a problem in this retrospective, questionnaire-based investigation, since these questionnaires were designed to be used in order to describe recent feelings (6, 10). Therefore, the DLQI and HDSS values before therapy may be influenced by this time effect. The same holds true for our questionnaire on sweating characteristics. It cannot be excluded that the treatment might modify the patterns of sweating. Nevertheless, our mean DLQI and HDSS scores before therapy were similar as those found in the literature (see below). Furthermore, sweating symptoms may often recur after therapy initiation, for example by the recurrence several months after botulinum toxin. No use was made of methods to map or quantify the degree of sweating, such as iodine starch test (18, 19), gravimetry (3, 14, 20) or transepidermal water loss measurement (21). Therefore, no objective data could be obtained. On the other hand, objective data can be difficult to interpret in this disorder, characterized by its fluctuating behaviour. Moreover, the quality of life burden may diverge with objective findings.
All therapies given are established treatments for hyperhidrosis. In a highly selected group of 38 axillary hyperhidrosis patients waiting for surgery, 20% aluminium chloride hexahydrate gave considerable relief in 24 patients, of whom 5 experienced irritation (13) The same solution was given to 12 patients with palmar hyperhidrosis, of whom all patients reported that their treated hands were drier than their untreated hands (21). The treated sides had significantly decreased transepidermal water loss values compared with the untreated sides (21). In our study, 11 out of 29 patients treated with antiperspirants judged their effect as good or excellent. The most frequent side-effect was local erythema and/or irritation, which was severe enough to stop this therapy in 5 patients.
There is an abundance of literature about the beneficial effect of botulinum toxin injections, of which we cite a selection (2–5, 16, 19). In these controlled studies in axillary hyperhidrosis, response rates varied from 14 out of 23 patients (5) to 100% (3). DLQI scores decreased from 10.1 to 4.3 (axillae and palmoplantar) (16) and 18 to 4 (axillae) (19) after treatment, which correspond to our data (12.9 to 2.6). We have found 27 out of 33 patients with exclusively axillary hyperhidrosis in whom botulinum toxin had a beneficial effect. Also the mean duration of its effect (5.9 months) in our group was similar to other studies. Recurrence was noted after a mean period of 18 weeks for palmar hyperhidrosis (19), whereas in studies on axillary hyperhidrosis, the mean duration was 6 months (17), 7.6 months (5) and 12 months (3). Side-effects in the axillae were only transient and mild (2–5, 17), as found in our material.
In a study on iontophoresis in 11 palmar hyperhidrosis patients, 6 patients were satisfied enough to continue with maintenance treatment (20). In contrast, Akins et al. (18) observed a clinical response in 24 out of 27 treated sites (palms, soles, axillae). A positive clinical response was arbitrarily interpreted as a greater than 50% inhibition of sweating as estimated by two physicians (18). A more recent study on 112 palmoplantar hyperhidrosis patients showed that there were 21 non-responders, defined as an unsatisfactory result within 20 days after stopping iontophoresis (14). In our study, 12 out of 17 patients were satisfied with iontophoresis, and continued this therapy at home. Side-effects were seen in only a minority, and were not a reason to stop this treatment. In contrast, erythema, burning and discomfort were noted by others (14, 18). The low incidence of side-effects in our study may be due to the fact that the patients could adjust the strength of the current, guided by the occurrence of tingling sensations.
Subcutaneous curettage is a form of surgical removal of overactive sweat glands that is highly selective (17). The patient’s subjective assessment was “good” or “very good” in a study by Rompel & Scholz (5) in 51 out of 77 patients who underwent curettage. The outcome for patient’s satisfaction was not significantly different from that after botulinum toxin injections, but the median follow-up duration was longer in the curettage group (5). Side-effects were wound infection, epidermal necrosis and haematoma formation. The number of patients (n = 4) who had curettage in our study was too low to draw significant conclusions concerning its efficacy and side-effects.
The group who was treated with oxybutynin represents a part of the larger group that was reported on earlier (7). In that report, oxybutynin had a good or excellent effect in 11 out of 14 patients with generalized hyperhidrosis. Therefore, oxybutynin is an important exception of the generally hold understanding that systemic anticholinergics have a too low benefit:risk ratio to justify their use in hyperhidrosis (1, 8, 12). In the current study, 8 out of 11 patients experienced a good or excellent effect. Three out of 11 patients stopped this drug because of anticholinergic side-effects. The incidence and intensity of side-effects may differ among individual anticholinergic agents. This may be partly explained by receptor selectivity (22). This therapy was used only in patients with generalized hyperhidrosis. Recently, we observed (very) good responses of oxybutynin in patients with focal forms of hyperhidrosis who did not respond to antiperspirants (not published).
In order to make a rational decision as to when to choose a certain therapeutic option, treatment algorithms are proposed (9). Such algorithms are not hard-and-fast rules, but should be adapted in a flexible way, nourished by new findings. We agree on the initial and proper use of local antiperspirants as proposed by Hornberger et al. (9). However, oxybutynin should be considered not only in generalized forms, but also in focal forms, before sympathectomy, given the potential hazards of the latter procedure.
In conclusion, 50% of our patients had axillary hyperhidrosis, and in a further 22% the axillary hyperhidrosis was combined with hyperhidrosis in other regions. In 16% of the patients there was generalized hyperhidrosis. In about half of all cases, patients recognized that their sweating occurred in attacks. These attacks were mostly triggered by warmth or exercise, or had no apparent cause, and, less frequently, were triggered by emotions. The quality of life of patients was low. All treatments improved quality of life. These findings may reflect the nature of this retrospective, questionnaire-based study. Given the importance of this subject, large-scale, prospective investigations are required.
The authors declare no conflicts of interest.
REFERENCES
1. Stolman LP. Treatment of hyperhidrosis. Dermatol Clin 1998; 16: 863–869.
2. Schnider P, Binder M, Kittler H, Birner P, Starkel D, Wolff K, Auff E. A randomized, double-blind, placebo-controlled trial of botulinum A toxin for severe axillary hyperhidrosis. Br J Dermatol 1999; 140: 677–680.
3. Heckmann M, Breit S, Ceballos-Baumann A, Schaller M, Plewig G. Side-controlled intradermal injection of botulinum toxin A in recalcitrant axillary hyperhidrosis. J Am Acad Dermatol 1999; 41: 987–990.
4. Naumann MK, Hamm H, Lowe NJ. Effect of botulinum toxin type A on quality of life measures in patient with excessive axillary sweating: a randomized controlled trial. Br J Dermatol 2002; 147: 1218–1226.
5. Rompel R, Scholz S. Subcutaneous curettage vs. injection of botulinum toxin A for treatment of axillary hyperhidrosis. Eur Acad Dermatol Venerol 2001; 15: 207–211.
6. Strutton D, Kowalski JW, Glaser DA, Stang PE. US prevalence of hyperhidrosis and impact on individuals with axillary hyperhidrosis: results from a national survey. J Am Acad Dermatol 2004; 51: 241–248.
7. Tupker RA, Harmsze AM, Deneer VHM. Oxybutynin in the treatment of generalized hyperhidrosis. Arch Dermatol 2006; 142: 1065–1066.
8. Togel B, Greve B, Raulin C. Current therapeutic strategies for hyperhidrosis: a review. Eur J Dermatol 2002; 12: 219–223.
9. Hornberger J, Grimes K, Naumann M, Glaser DA, Lowe NJ, Naver H, et al. Recognition, diagnosis, and treatment of primary focal hyperhidrosis. J Am Acad Dermatol 2004; 51: 274–286.
10. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI) – a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; 19: 210–216.
11. Lear W, Kessler E, Solish N, Glaser DA. An epidemiological study of hyperhidrosis. Dermatol Surg 2007; 33: S69–S75.
12. Hurley HJ. Diseases of the eccrine sweat glands. In: Bologna JL, Jorizzo JL, Rapini RP, editors. Textbook of dermatology. London: Mosby, 2003: p. 567–586.
13. Rayner CRW, Ritchie ID, Stark GP. Axillary hyperhidrosis, 20% aluminium chloride hexahydrate, and surgery. BMJ 1980; 280: 1168.
14. Karakoç Y, Aydemir EH, Tunaya Kalkan M, Unal G. Safe control of palmoplantar hyperhidrosis with direct electrical current. Int J Dermatol 2002; 41: 602–605.
15. Krogstad AL, Mork C, Piechnik SK. Pattern of sweating and response to stress and exercise in patients with palmar hyperhidrosis. Br J Dermatol 2006; 154: 1118–1122.
16. Swartling C, Naver H, Lindberg M. Botulinum A toxin improves life quality in severe primary focal hyperhidrosis. Eur J Neurol 2001; 8: 247–s52.
17. Tan SR, Solish N. Long-term efficacy and quality of life in the treatment of focal hyperhidrosis with botulinum toxin A. Dermatol Surg 2002; 28: 495–499.
18. Akins DL, Meisenheimer JL, Dobson RL. Efficacy of the Drionic unit in the treatment of hyperhidrosis. J Am Acad Dermatol 1987; 16: 827–832.
19. Simonetta Moreau M, Cauhepe C, Magues JP, Senard JM. A double-blind, randomized, comparative study of Dysport® vs. Botox® in primary palmar hyperhidrosis. Br J Dermatol 2003; 149: 1041–1045.
20. Dahl JC, Gelent-Madsen L. Treatment of hyperhidrosis manuum by tap water iontophoresis. Acta Derm Venerol 1989; 69: 346–348.
21. Goh CL. Aluminum chloride hexahydrate versus palmar hyperhidrosis. Int J Dermatol 1990; 29: 368–370.
22. Nelson CP, Gupta P, Napier CM, Nahorski SR, Challiss RAJ. Functional selectivity of muscarinic receptor antagonists for inhibition of M3-mediated phosphoinositide responses in guinea pig urinary bladder and submandibular salivary gland. J Pharmacology Exp Ther 2004; 310: 1255–1265.

