This non-interventional observational open study (TOCCATA, sponsored by Basilea Pharmaceutica Germany) investigated the use of alitretinoin to treat chronic hand eczema under daily “real life” medical practice conditions in Germany. A total of 349 dermatologists throughout Germany enrolled 680 adult patients with chronic hand eczema. Patients were prescribed and treated with alitretinoin in accordance with the summary of product characteristics. The maximum observation duration was 24 weeks, with efficacy and safety parameters evaluated every 4 weeks. Efficacy was primarily evaluated by assessing disease severity according to the Physician Global Assessment. In total, 56.7% of patients achieved a Physician Global Assessment rating of “clear” or “almost clear” hands, with only small differences in patients with different morphological forms: hyperkeratotic-rhagadiform (59.2%), fingertip (52.2%) and vesicular (47.9%). This observational study demonstrates the effectiveness and tolerability of alitretinoin in everyday clinical practice in addition to the known efficacy and safety obtained by randomized controlled clinical trials. Key words: alitretinoin; chronic hand eczema; observational study: efficacy.
(Accepted August 29, 2011.)
Acta Derm Venereol 2012; 92: XX–XX.
Thomas L. Diepgen, Department of Clinical Social Medicine, Occupational & Environmental Dermatology, Ruprecht-Karls-University Heidelberg, DE-69115 Heidelberg, Germany. E-mail: thomas.diepgen@med.uni-heidelberg.de
Hand eczema is a common skin disorder, with a one-year prevalence of up to 10%. Severe chronic hand eczema (CHE) is thought to account for up to 7% of cases of CHE (1–4). Although no single causative factor for hand eczema has been identified, genetic predisposition, an altered immune response, atopy and environmental factors, such as handling chemicals or other skin irritants, have all been suggested as contributing factors. Due to this multifactorial aetiology it is often difficult to identify and eliminate all potential causative factors (4–6).
Severe hand eczema resulting in prolonged disability is associated with a high health economic burden and significant loss of quality of life (7, 8). Although numerous treatment options are available, the management of CHE is often difficult and unsatisfactory. Therefore, guidelines for the management of hand eczema have been developed during the last 2 years in several countries (9–14). The authors of these guidelines came to the conclusion that there is a lack of, and simultaneously a need for, well-designed controlled clinical trials, especially in directly comparing available treatment modalities and demonstrating effectiveness under daily practice conditions.
It is estimated that the majority of patients with severe CHE are unresponsive to standard treatments (4), and for these patients alitretinoin (Toctino®) has recently become available as the only approved systemic treatment option. Alitretinoin (9-cis retinoic acid) is an endogenously occurring physiological vitamin A derivative (retinoid) with its main mechanism of action in CHE thought to be anti-inflammatory and immunomodulatory.
In the clinical development programme for registration, studies of up to 6 months’ duration with alitretinoin have shown that it is highly effective in the treatment of severe CHE unresponsive to potent topical corticosteroids and is well tolerated with a good safety profile (15–17). Alitretinoin was initially granted approval by several European authorities, including the German Health Authorities in autumn 2008, for the treatment of patients with severe CHE unresponsive to potent topical corticosteroids.
TOCCATA was designed as a non-interventional study to further investigate the effectiveness and tolerability of alitretinoin, and to collect structured data under daily dermatological practice conditions. While clinical trials are conducted in an ideal setting, adequately designed and performed observational studies can contribute significantly to the understanding of disease and its management under real-life conditions. In healthcare research, investigations of the treatment of chronic skin diseases under everyday conditions in dermatological clinics and private practice have become more important in recent years. TOCCATA is the first such study investigating the treatment of CHE with oral alitretinoin in Germany.
MATERIALS AND METHODS
Between November 2008 and March 2010, 680 patients were enrolled into the TOCCATA study by 349 dermatologists throughout Germany. (TOCCATA: “Toctino® bei schwerem chronischem Handekzem – Therapieverlauf in Anwendungsbobachtung” (Toctino® in severe chronic hand eczema – therapy in an observational study)).
The study was approved by the ethics committee of the University of Heidelberg. In line with the principles of a non-interventional observational study, the treating physicians documented alitretinoin treatment (30 or 10 mg daily) of adult patients with severe CHE unresponsive to potent topical corticosteroids during routine medical practice. This was done in the usual manner, in accordance with the terms of the marketing authorization and the summary of product characteristics (18) and considering the pertinent hand eczema management guideline (11). Patients with CHE treated by a dermatologist could be included in the study if the following criteria were met: (i) disease duration of at least 3 months or more than 2 flares within the last 12 months (according to the Guideline of the German Dermatological Society (11); (ii) pretreatment with topical corticosteroids; (iii) no long-lasting healing under adequate topical treatment including corticosteroids; and (iv) no other active severe skin diseases or acute skin infections dominating the clinical picture.
For female patients of child-bearing age, strict adherence to pregnancy prevention measures, including pregnancy testing, contraceptive counselling and effective contraception was required, and contraception was continued for one month after completion of therapy according to the summary of product characteristics.
The planned maximum observation period was 24 weeks, and information was documented at baseline (T0), i.e. before treatment start, at the 4-weekly follow-up visits, and at the end of observation at week 24 (or after clearance of CHE symptoms). From visit T3 onwards (week 12), treatment could be stopped if the patient showed total clearance of their CHE, as assessed by the Physician Global Assessment (PGA). The severity of hand eczema was defined according to the PGA (17), and for a standardized assessment a validated photographic guide (19) was distributed to each study investigator as an aid to evaluating the severity of CHE. The definition of subtypes of hand eczema was defined according to the German guidelines “Guideline on the management of hand eczema” (11).
The case report forms (CRFs) captured 10 major data categories (demographics, CHE diagnosis, previous therapies, working ability, Toctino® dosage, therapy completion, compliance, PGA, overall assessment of effectiveness and tolerability by the physician and patient, respectively, adverse drug reactions), amounting to 100 up to almost 200 data points for each patient, depending on the number of follow-up visits. For women of childbearing age, all activities documenting concurrence with the approved Pregnancy Prevention Programme were documented by the treating physician.
Statistical methodology
Data from all available patient CRFs were taken into account, including those from patients who discontinued treatment early. All parameters were presented descriptively; for continuous variables the descriptive parameters: number, mean value, standard deviation, minimum, 5% quantile, 25% quantile, median, 75% quantile, 95% quantile and maximum were calculated. Missing values were not considered in the calculations. For categorical variables, absolute and relative frequencies were calculated.
RESULTS
Population demographics and characteristics
Baseline patient demographics and characteristics are shown in Table I. The mean duration of disease was approximately 7 years, and over 50% of patients had ongoing disease for more than 3 years. The majority of the patients (78%) were working, although 42% of them reported sickness absence in the previous 12 months (mean 35 days); at the start of the study 15% were currently on sick leave (mean 59 days). The most frequently represented employment groups were metalworkers and electricians (17%), healthcare professionals (10%), foodstuff and gastronomy workers (9%), construction workers (6%) and cleaners (5%).
Apart from the 96% of patients presenting with CHE on both hands, 39% also had eczema present on the feet, and 19% on other body areas. Almost two-thirds of patients presented morphologically with hyperkeratotic disease and over one-third with the vesicular (dyshidrosiform) pompholyx type (Table I, multiple nominations possible).
In the 12 months prior to baseline, 669 patients (98%) had been treated with many different types of therapies for severe CHE: 665 (98%) with topical therapies, 289 (43%) with various forms of ultraviolet (UV) therapy (cream, bath or systemic therapy), and 458 (67%) with systemic treatments. Of the systemic non-symptomatic therapies, the most common were corticosteroids (45%), retinoids (15%), cyclosporine (7%), methotrexate (5%) and azathioprine (1%).
Table I. Patient characteristics and aetiology, morphology and localization of chronic hand eczema (CHE) at baseline (including eczema in other body areas)
|
Characteristics
|
|
|
Total patients enrolled, n
|
680
|
|
Age, years, mean ± SD
|
49.9 ± 12.6
|
|
Males, n (%)
|
375 (56)
|
|
Females, n (%)
|
299 (44)
|
|
Body weight, kg, mean ± SD
|
79.2 ± 14.3
|
|
Duration of CHE, years, mean ± SD
|
6.7 ± 8.0
|
|
≤ 12 months, n (%)
|
127 (19)
|
|
> 12–36 months, n (%)
|
177 (27)
|
|
> 36–72 months, n (%)
|
115 (17)
|
|
> 72 months, n (%)
|
244 (37)
|
|
CHE subtypesa,b: Aetiological and morphological criteria, n (%)
|
|
Irritant
|
159 (24)
|
|
Atopic
|
166 (25)
|
|
Allergic
|
91 (14)
|
|
Vesicular/pompholyx
|
241 (36)
|
|
Hyperkeratotic-rhagadiform
|
437 (65)
|
|
Fingertip
|
91 (14)
|
|
Localization of eczemaa,c, n (%)
|
|
Both hands
|
645 (96)
|
|
Feet
|
254 (39)
|
|
Other body areas
|
124 (19)
|
aMultiple nominations were possible; data available for b668 patients; c665 patients.
SD: standard deviation.
In spite of this extensive use of topical and systemic therapies, at baseline all patients presented with a CHE history of at least 3 months or more than two relapses within the previous year. The inadequacy of previous therapy was also reflected by the actual PGA-severity grade that was determined post-inclusion at baseline, showing that the overwhelming proportion of patients (99.1%) were actually PGA-severe (64.5%) or PGA-moderate (34.6%).
Efficacy
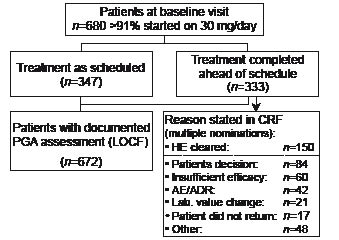
The flow of patients through the study is shown in Fig. 1. Over 91% of patients were initially prescribed alitretinoin 30 mg per day, and almost 75% of the patients received this dose unchanged throughout their treatment course. A total of 333 (49%) patients completed treatment ahead of schedule, 45% of whom stated their reason for discontinuation was “clearance of hand eczema”.
Fig. 1. Flow of study participants. PGA: Physician Global Assessment; CRF: case report form; HE: hand eczema; AE/ADR: adverse event/adverse drug reaction; LOCF: last observation carried forward.
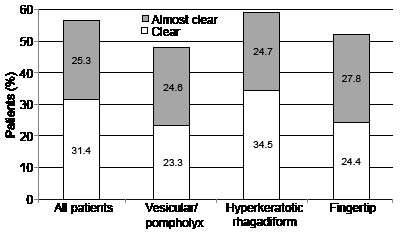
According to the last observation carried forward analysis (LOCF), 57% of patients achieved a PGA rating of “clear” or “almost clear” hands (Fig. 2), with a continuous increase in response observed during the treatment course. Similar response rates (LOCF) were seen for all three morphological types, with a slightly higher response rate observed for the hyperkeratotic type (Fig. 2). Slightly higher response rates (61%) were observed for patients rated PGA-moderate at the beginning and slightly lower rates (53%) for patients rated PGA-severe at baseline. In addition, a trend for a reduction in the level of sickness absence was apparent during alitretinoin treatment.
Fig. 2. Physician Global Assessment (PGA) efficacy overall and stratified by baseline morphology (last observation).
The median length of treatment duration in TOCCATA was 153 days, with a tendency to be shorter for patients with a shorter pre-study duration of disease. This observation was most pronounced in patients with a hand eczema history of ≤ 1 year, where the median treatment duration was approximately 20% less (121 days). Other factors, such as gender, history of previous hospitalization due to CHE, or morphological type of CHE, had no influence on treatment duration.
Safety
The overall safety profile of alitretinoin was consistent with the known profile of the drug. A total of 298 adverse drug reactions were recorded in 23% of the 680 patients with headache as the most frequent one (7.5%) followed by increased blood triglycerides (4.9%) and increased blood cholesterol (3.8%). Serious adverse drug reactions were documented in only four (0.6%) patients (lymphatic oedema, paranoia, recto-sigmoiditis and soft-tissue swelling). In the 42 patients where treatment was discontinued due to adverse reactions, headache was the most frequent reason (26 patients) and in the 21 patients where treatment was discontinued due to clinically relevant changes of laboratory values this was mostly due to lipid value changes (9 out of 11 patients where changes were specified).
Physician’s overall assessment of efficacy and tolerability, respectively, was “good/very good” in approximately 80% of patients, which was similar to the corresponding assessments of the patients themselves (approximately 75%). Patient compliance, as judged by the treating physician at each visit, was rated as “good” in 90% throughout the observation period, and only 6% of patients discontinued treatment within the first 4 weeks for any reason.
DISCUSSION
The objective of the TOCCATA study was to gain further insight into the effectiveness and tolerability of alitretinoin in patients with severe CHE under daily medical practice conditions, and how these observations might correlate with data collected under a strict randomized clinical trial setting.
The patient demographics and characteristics of TOCCATA were very similar to those seen in the Phase III clinical trial programme. The mean duration of disease was approximately 7 years in TOCCATA, slightly shorter than in the pivotal Phase III BACH study (9 years) (17).
Occupational exposure to skin irritants and allergens can contribute to the development of hand eczema (20, 21). Of note, a trend for a reduction of sickness absence and CHE-related productivity loss was apparent with alitretinoin treatment, and this important aspect should be further explored in the most appropriate healthcare and social system setting, e.g. an occupational health insurance framework.
Taking all dosages and different morphological/aetiological diagnoses into account, 57% of patients were assessed as having “clear” or “almost clear” hands according to PGA in the TOCCATA study. This correlates remarkably well with the 48% of patients with a similar PGA result in the alitretinoin 30 mg treatment arm of the BACH study, even though not all patients in TOCCATA were treated continuously with alitretinoin 30 mg as they were in the BACH study in the 30 mg treatment arm.
The slightly better therapeutic response in TOCCATA might be explained by the fact that patients were able to continue with some concomitant treatments, whereas all concomitant CHE medications were excluded in the alitretinoin CHE clinical trials. In addition, one-third of patients in TOCCATA had only PGA-moderate disease post-inclusion at baseline, whereas in the BACH study all patients had to be PGA-severe for inclusion in the study.
The well-documented morphological diversity of CHE was clearly demonstrated in this study and the therapeutic response broken down by morphological diagnosis showed a high level of healing (“clear” or “almost clear”) in all three forms of eczema in this study.
The heterogeneity of the disease was also reflected by the fact that the majority of the patients (96%) had eczema on both hands, and 40% of patients also had eczema of the feet (not recorded in previous trials). A post-TOCCATA follow-up in nearly 200 patients with “clear” or “almost clear” PGA whose feet were also affected showed that in 60% it was indicated that the treatment response was comparable on hands and feet.
The duration of treatment with alitretinoin in TOCCATA showed a tendency to be shorter in those patients with a shorter duration of disease, especially those less than one year, but this observation requires further verification.
The safety findings in TOCCATA were consistent with those in previous clinical trials (15–17, 22), and confirmed the tolerability profile of alitretinoin. The most common treatment-emergent adverse reaction was headache (7.5%), followed by increased triglycerides and increased cholesterol. These are known to be typical retinoid class effects and are transient and well manageable, e.g. treatment of headache by commonly used analgesics or by dose reduction. However, by design in observational trials specific laboratory investigations are usually not imposed but follow common medical practice. Therefore, it might be possible that relevant changes in laboratory values, such as indicating hypothyreosis (23, 24) might have been overlooked in our study.
According to the summary of product characteristics for alitretinoin, for CHE patients with pre-existing cardiovascular risk factors treatment is recommended to be started with 10 mg. In 9% of patients, 10 mg was chosen as the initial dose and 6% of patients remained at this dose throughout treatment. The 10 mg dose also provides an option for temporary or permanent dosage reduction in case of treatment emergent side-effects or tolerability problems that might occur on the recommended starting dose of 30 mg per day. The option of titrating the alitretinoin daily dose either up or down was used in 22% of the patients, similar to data from earlier market investigations. TOCCATA has confirmed that treating physicians are taking advantage of the dosage adjustment option when using alitretinoin.
For a variety of reasons randomized clinical trials, considered as the gold standard in the clinical evidence hierarchy, cannot collect all the data relevant for use in everyday clinical practice. Time-limited drug exposure, restricted endpoints, limited sample sizes, and strict inclusion and exclusion criteria all limit the use of the results in a wider context. Non-interventional observational studies, if adequately designed and performed, can add important information from real-world medical practice despite the known inherent limitations, such as non-random assignment, unblinded assessments, and quality limitations of the collected data. Despite these potential limitations, TOCCATA has shown that data collected during routine medical practice are consistent with the data obtained during the strict clinical trial conditions of the drug development programme. These types of “real-life” studies are important in confirming the effectiveness and tolerability of newly licensed drugs.
In conclusion, this first, large, non-interventional observational open study of alitretinoin, following approval in Germany, shows that the good efficacy and safety profile obtained in the CHE clinical development registrational programme is consistent with the effectiveness and tolerability profile observed under “real life” conditions in dermatological practice.
ACKNOWLEDGEMENTS
These trials were supported and funded by Basilea Pharmaceutica Deutschland GmbH Muenchen Germany. All authors listed participated in writing the protocol, study conduct, data analysis and interpretation, and manuscript generation and review for publication. This non-interventional study was registered in the NIS-database of the German VFA (Verband Forschender Arzneimittelhersteller).
Conflict of interest. TL Diepgen was the principal investigator for the study and has received lecture and consultancy fees from Basilea. T. Zimmermann was the study director and is an employee of Basilea Pharmaceutica GmbH, Germany. E. Pfarr was the study statistician and is an employee of the CRO AMS Advanced Medical Services GmbH Mannheim, Germany.
REFERENCES