Yuta Majima1, Satoshi Hirakawa1*, Yukiko Kito1, Hiroki Suzuki1, Masayo Koide2, Hidekazu Fukamizu3 and Yoshiki Tokura1
Departments of 1Dermatology and 3Plastic and Reconstructive Surgery, Hamamatsu University School of Medicine, Hamamatsu 431-3192, and 2Division of Dermatology, Hamamatsu Red Cross Hospital, Hamamatsu 434-8533, Japan. *E-mail: hirakawa@hama-med.ac.jp
Accepted May 8, 2012.
Basal cell carcinoma (BCC), a common tumour of epithelial origin, is locally invasive and has a low risk of metastasis, estimated to range from 0.028% to 0.1% (1). However, once BCC metastasizes to distant organs, the effective therapeutic options are limited, leading to poor patient outcome.
Recent studies have shown that epithelial-mesenchymal transition (EMT) suppresses epithelial features, and induces mesenchymal traits to epithelial cells in several pathological conditions (2, 3). Of note is that tumours of epithelial origin can express transcription factors Snail and Twist1, or the cell adhesion molecule N-cadherin as a mesenchymal marker. We have previously shown that N-cadherin is up-regulated in invasive tumours, but not in carcinoma in situ of extramammary Paget’s disease, and that EMT is associated with distant organ metastasis, leading to poor patient survival (4, 5). However, it remains unclear whether EMT plays a key role in the development of highly invasive phenotype and potential metastasis in BCC. We report here the first case of morphoeic and metastatic BCC showing the induction of Twist1 and the epithelial-to-mesenchymal conversion of cadherins in association with multiple organ metastases.
CASE REPORT
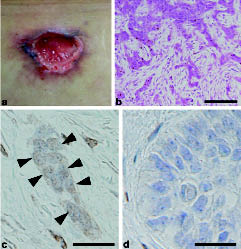
A 51-year-old Japanese man presented with a 3-cm ulcerated nodule with peripheral focal pigmentation on the upper back (Fig. 1a). A biopsy specimen disclosed the proliferation and invasion of epithelial strands with mesenchymal transition and rich stroma, indicating a diagnosis of morphoeic BCC (Fig. 1b). The patient underwent a tumour resection, and the defect was reconstructed with the trapezius musculocutaneous flap. After 4 years of follow-up, a subcutaneous mass appeared in the patient’s supraclavicular fossa. Under the histological diagnosis of metastatic BCC, the tumour was surgically resected with subsequent reconstruction using the pectoral major musculo-cutaneous flap, followed by a total of 60 Gy radiation to the local region. However, multiple foci of tumour metastasis were found in the left levator scapulae muscle and the pleura of the left lung by magnetic resonance imaging. The patient underwent systemic chemotherapy with a combination of cisplatin and doxorubicin. However, the therapeutic effect was minimal, and at the time of writing, the tumours were disseminated in the lung.
Fig. 1. Clinical, roentgenological, and pathological features in metastatic basal cell carcinoma (BCC). (a) Clinical presentation of 3-cm ulcerated nodule on the upper back with peripheral, focal pigmentation. (b) Haematoxylin & eosin stains (× 400) of the cutaneous primary site show foci of basaloid tumour cells on the superiorly and infiltrative tumour cells within the stroma. (c) Prominent Twist1 expression was revealed in the nuclei of tumour cells (arrowheads) at the invasive front in the index case. (d) No Twist1 expression was found in control representative nodular BCC by immunohistochemistry. Scale bars = 100 µm (b); 30 µm (c, d).
To clarify the potential role of EMT in metastatic BCC, we investigated the tumour by immunohistochemical analyses. Formalin-fixed paraffin-embedded sections of the index case showed that the tumour cells were positive for Twist1 at the invasive front of the primary tumour (Fig. 1c), whereas the tumour cells centrally were negative for Twist1. In order to specify Twist1 expression in metastatic BCC, control representative tumour cells of nodular BCC were analysed by immunohistochemistry (Fig. 1d). These non-metastatic tumour cells showed no Twist1 expression in the nuclei (Fig. 1d). Furthermore, double immunofluorescence stains for E-cadherin and N-cadherin showed that E-cadherin was prominently expressed in the nodular form of BCC (Fig. 2a), whereas this epithelial marker was markedly decreased in the tumour cells of the index case (Fig. 2b). In contrast, whereas no N-cadherin expression was found in the control nodular form of BCC (Fig. 2c), tumour cells of the index case markedly bore N-cadherin at the invasive front (Fig. 2d). Moreover, high levels of expression of Twist1 and N-cadherin were found in metastatic tumour cells of the supraclavicular fossa in the index case, whereas E-cadherin expression was markedly decreased in the metastatic tumours. Therefore, these results demonstrate, for the first time, that highly invasive and metastatic BCC may show Twist1 expression and an epithelial-to-mesenchymal conversion of cadherins in the primary sites, indicating that EMT might play a key role in the promotion of tumour invasion and subsequent metastasis.
Fig. 2. Cadherin conversion by epithelial-mesenchymal transition (EMT) in metastatic basal cell carcinoma (BCC). Double immunofluorescence stains for E-cadherin (red) and N-cadherin (green) in non-metastatic nodular BCC as control (a, c) and the index case (b, d). E-cadherin was prominently expressed by tumour cells in nodular BCC (a), whereas no N-cadherin was observed in those cells (c). In contrast, the expression levels of E-cadherin were markedly decreased in tumour cells at the invasive front in the index case (b). Furthermore, N-cadherin was strikingly induced in those cells (d), indicating that highly invasive and metastatic BCC is capable of converting epithelial characteristics to mesenchymal features by EMT. Nuclei are stained in blue with 4’,6-diamidino-2-phenylindole. (a–d) Scale bars = 50 µm.
DISCUSSION
The present case reveals a potential impact of Twist1 on marked invasion and metastasis in BCC. Twist1, a basic helix-loop-helix transcription factor, was originally identified as a master regulator of EMT and metastasis in an experimental tumour model (6). Furthermore, Twist1 is significantly up-regulated in patients with metastatic breast cancer compared with those who remained at early stages (7). Twist1 may be a feasible biomarker for highly invasive and/or metastatic BCC. The expression levels of Snail, the other transcription factor promoting EMT, have been shown to correlate with the depth of tumour invasion in BCC (8). However, no significant relationship was found between Snail and down-regulation of E-cadherin (8), suggesting that another transcription factor is involved in the regulation of EMT in BCC. Our finding is in accordance with the notion that Twist1 is capable of promoting EMT, contributing to aggressive invasion and multiple organ metastases.
The primary tumour of the present patient was histopathologically diagnosed as morphoeic BCC, a stroma-rich form of the cutaneous neoplasm. We previously showed that EMT markers Snail and Twist1 were expressed in the eccrine glands in patients with systemic sclerosis (2, 9). Therefore, a subpopulation of cell lineages in eccrine glands might undergo EMT and further differentiate into the myofibroblasts, contributing to marked fibrosis of the disease. In the present case, tumour cells prominently expressed Twist1 at the invasive front, forming morphoeic fibrosis within the primary sites. Of note, tissue fibrosis is mediated by several inflammatory cytokines, such as transforming growth factor-β, which is a key soluble factor facilitating EMT in tumour progression. Thus, BCC undergoing EMT might induce fibrotic skin change, and subsequently develop tumour cell invasion and metastasis.
REFERENCES