


Mohammad Alimohammadi1,2, Mats Andersson2 and Anna Rostedt Punga3
Departments of 1Medical Sciences and 3Clinical Neurophysiology, Uppsala University, and 2Q-MED, a Galderma Division, Uppsala, Sweden
Despite the extensive use of botulinum toxin type A (BoNT-A) in treatments for glabellar frown lines; the dose-response effect in the glabellar muscles remains unknown. The aim of this randomized, double-blind, placebo-controlled prospective study was to characterize the neurophysiological parameters that correlate with the effect of BoNT-A in the glabellar muscles and its diffusion to surrounding ocular muscles. Sixteen healthy women were recruited and randomized to 3 different dose-groups of onabotulinumtoxin A (Vistabel) or placebo and followed 24 weeks by neurophysiological examinations. Efficacy of treatment on corrugator supercilii muscles was measured by compound motor action potential (CMAP) and electromyography (EMG). Photographs were used to score glabellar frown lines. Diffusion of the drug to surrounding muscles was assessed by CMAP of the nasalis muscle, EMG and concentric needle electrode jitter analysis (CNE) of the orbicularis oculi muscle. CMAP reduction correlated well with intramuscular BoNT-A dose. Muscle paralysis, measured by EMG, began from 2 weeks and was not entirely reversed at 24 weeks in individuals who received high dose of onabotulinumtoxin. In conclusion, we developed a novel neurophysiological strategy for effect evaluation of BoNT-A in glabellar muscles. CMAP and EMG correlated with given BoNT-A dose and are more defined effect measures than clinical glabellar photo scales. Key words: botulinum toxin; glabellar muscles; compound motor action potential; electromyography.
Accepted Mar 20, 2013; Epub ahead of print Aug 8, 2013
Acta Derm Venereol 2013; 93: XX–XX.
Mohammad Alimohammadi, Department of Medical Sciences, Uppsala University, SE-751 85 Uppsala, Sweden. E-mail: mohammad.alimohammadi@medsci.uu.se
Botulinum toxin type A (BoNT-A) prevents the release of acetylcholine (ACh) from the nerve terminal into the neuromuscular junction (NMJ) (1). The reduced ACh release results in neuromuscular blockade and subsequent pharmacological denervation. This effect remains until innervation has been re-established; which results in recovery of the original or new NMJs within approximately 12 weeks (2, 3), usually with limited temporary formation of nerve sprouting during the recovery process. BoNT-A is used in a wide range of medical treatments of muscular hyperactivity/tension, extending from spasticity and dystonia to aesthetic treatment of wrinkles caused by underlying muscle tension, primarily in the area between the eyes (the glabellar complex). Glabellar frown lines are caused by tension in the corrugator supercilii and procerus muscles, and BoNT injection into the glabellar muscles results in paralysis, and hence diminished glabellar frown lines.
BoNT-A exerts its predominant action in the peripheral nervous system. Diffusion has been reported to contralateral facial muscles upon unilateral BoNT-A application (4) as well as remote spread from the site of injection, even to arm muscles, upon facial muscle injection (5). These documented possibilities of still-unknown pharmacological BoNT-A effects emphasize the importance of correct administration of the toxin in terms of injection-points, dose selection, and appropriate effect surveillance.
Visual clinical rating scales that focus on wrinkle depth and maximal muscle contraction are commonly used as efficacy measures of BoNT in facial muscles (6, 7). Nevertheless, these scales are not sensitive enough to detect subtle difference in effect between various BoNT-A formulations or doses (8–10) or even simple parameters, such as details of the exact onset of action. Neurophysiological studies comparing different BoNT products have mainly analysed the compound motor action potential (CMAP), i.e. the collective muscle response upon motor nerve stimulation, and then almost exclusively in the small foot extensor muscle (11–13). Few studies have addressed neurophysiology in facial muscles in a limited fashion (14, 15); however, such measures would enable evaluation of time to onset and duration of treatment effect upon BoNT-A injection in the tiny glabellar muscles.
The aim of this prospective study was to evaluate whether neurophysiological measures correlated with the local effect of BoNT-A in the glabellar muscles as well as with the effects of spread to surrounding facial muscles. We found that neurophysiological measures are highly sensitive for the assessment of dose-response effect upon BoNT-A injection in the glabellar muscles.
MATERIALS AND METHODS
Participants
A total of 16 healthy women, age range 31–64 years, were enrolled from January to March 2012, through public advertisements. Inclusion criteria were visible glabellar frown lines at rest or prominent glabellar muscles. Exclusion criteria were a diagnosis/symptoms of a neuromuscular disorder (e.g. myasthenia gravis), allergy to BoNT-A, previous BoNT-A injection, plastic surgery/implants in the facial area, on-going infection, systemic disease or inflammation surrounding injection areas, earlier unspecific severe allergic reactions, coagulation disorder or medication with anticoagulants or muscle relaxants, pregnancy or lactation.
Ethics
The study was approved by the Regional Ethical Review Board of Uppsala (Dnr: 2011/247)) and the Medical Products Agency (EudraCT nr: 2011-004636-66). All subjects were enrolled after written informed consent.
Study design
The study was designed as prospective, randomized, double-blind and placebo-controlled, where the evaluating clinical neurophysiologist (ARP) and the study subjects were blinded to the given substance and dose until after the study was finalized and analysed. All examinations were conducted at the Department of Clinical Neurophysiology, Uppsala University Hospital from January until September 2012. The neurophysiological and photographical baseline examinations were performed before the intramuscular injection of onabotulinumtoxinA (Vistabel® Allergan Inc. Irvine, California, USA) or placebo (Table I). The study subjects were randomized into 4 groups, with 4 individuals in each group. For the dilution of Vistabel, 1.25 ml 0.9% NaCl was added to a 50 U bottle of Vistabel®, which resulted in a dose of 4 U per 0.1 ml. The same injection volume, 0.1 ml, was given by a dermatologist (MOA) to all subjects in 5 standardized injection points using electromyography (EMG)-guided technique with disposable hypodermic needle electrodes (Bo-ject DHN 37, 37×0.46 mm; 26G, Alpine Biomed, Skovlunde, Denmark) to ensure central muscle injection. Group I received 1 unit/injection (total 5 units); group II received 2 units/injection (total 10 units); group III received 4 units/injection, (total 20 units); and group IV received 0.9% NaCl/injection. The recommended dose for treatment of glabellar frown lines is 20 units total (4 units/injection).
Table I. Comparison between glabellar frown line scores and neurophysiological parameters of the glabellar muscles corrugator supercilii with different doses of botulinum toxin type A (BoNT-A)
|
Dose (units) |
Change in glabellar score (mean) |
CMAP % reduction (mean left/right corrugator) |
|||
|
At rest |
At contraction |
||||
|
Placebo |
0.25 |
0 |
1.7 |
||
|
5 |
–0.50 |
–0.5 |
–56.7 |
||
|
10 |
–0.25 |
–0.5 |
–62.4 |
||
|
20 |
–0.75 |
–2.25 |
–64.4 |
||
CMAP: compound motor action potential.
Neurophysiological examinations and parameters
All neurophysiological examinations were made on Keypoint equipment (Medtronic®, Skovlunde, Denmark). The primary hypothesis (neurophysiological effects of BoNT-A), was evaluated by the following bilateral examinations (Table I): (i) motor neurography (CMAP): stimulation of the temporal branch of the facial nerve with surface electrodes, 4 cm lateral to the eye, and surface recording over the corrugator supercilii; (ii) EMG: a concentric facial EMG electrode (30G; 25 × 0.33 mm; Alpine Biomed, Skovlunde, Denmark) was placed in the corrugator supercilii and analysed spontaneous activity (indicating denervation out of total 10 recording positions within the muscle), quantitative analysis of motor unit potentials (MUPs) at slight voluntary activation and interference pattern at maximal muscle contraction.
To evaluate the secondary hypothesis (effects of spread to injection in adjacent muscles), we performed: (i) motor neurography (CMAP): the zygomatic branch of the facial nerve was stimulated 1.5 cm anterior to the tragus of the ear. Surface electrodes were placed over the muscle belly of the nasalis muscle; (ii) quantitative EMG in the ocular orbicularis oculi muscle. Reference values were provided from the database of normal values at the Department of Clinical Neurophysiology, Uppsala; (iii) jitter analysis with concentric needle electrodes (CNE): a disposable concentric facial EMG needle electrode (16) (30G; 25 × 0.33 mm; Alpine Biomed) was inserted in the lateral lower part of the orbicularis oculi muscle under slight voluntary contraction. Jitter (μs) was expressed as the mean consecutive difference (MCD) of 20 analysed potential pairs (17). MCD was considered normal with jitter values < 34 µs (18, 19). Filter settings were set to 1,000 Hz–10 kHz.
Photodocumentation of glabellar frown lines and subject’s diary
The study subjects were placed between 2 fluorescent strip lamps, fixed in the ceiling, at all follow-up visits. A Nikon D5000 with 105-mm Macro objective was used for photography of the glabellar area in 3 different modes: (i) relaxed mode; (ii) frontalis muscle contraction; and (iii) maximal glabellar muscle contraction. Glabellar frown lines in the relaxed state and at maximal contraction were graded on a 4-point clinical severity scale, from 0 to 3 points (7). In addition, study subjects were given a diary to document any treatment-related adverse events.
Statistical methods
For the end-points, where a measurement was available from left and right sides, the mean for each subject (n = 16) was used in the calculations. Both absolute and percentage change were calculated for each swubject, relating post-treatment values to baseline values. Statistical evaluations were performed based on these within-subject changes where the hypothesis was that the true mean of change was zero (1-sample t-test). Comparison of within-subject changes between dose-groups was performed using a 2-sample t-test, where the hypothesis to test was that the true mean of change was equal. A 2-sided p-value ≤ 0.05 was considered significant.
RESULTS
Clinical characteristics and aesthetic treatment results
All 16 enrolled women (age range 31–64 years, mean 44 years) were naive to previous BoNT-A treatment. None of them met any exclusion criteria, confirmed by neurological examination and CNE analysis of neuromuscular transmission. All subjects were examined at 0, 2, 4, 12 and 24 weeks. Fifteen subjects experienced no adverse events. One of the study subjects, in the 20-unit dose-group, experienced dry skin, seborrhoeic eczema, in the glabellar region. Glabellar frown lines in the relaxed state were graded from 0 to 2 and after BoNT-A treatment, the glabellar frown score did not necessarily change (Fig. S1; available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1647 and Table II). The mean baseline score at maximum frown was 2.5 (range 1–4). At 4 weeks, the number of subjects per group that had improved at least 1 point on the photo scale was 0, 2, 2 and 4 for the 0-, 5-, 10- and 20-unit group, respectively. Based on the photographs in was possible to distinguish between subjects who received placebo and those who received BoNT-A; however, it was not possible to use the photographs to distinguish different dose-groups from each other. Although blinded, all subjects who received the BoNT-A reported that they believed they had had received the active substance, and 11 of 12 persons, regardless of BoNT-A dose, were satisfied with the aesthetic outcome. In addition, one of the persons who received placebo experienced aesthetic improvement and positive impact on her self-confidence, indicating a well-known placebo effect (20).
Table II. Comparison of neuromuscular jitter (µs) as measured by concentric needle electrode in the orbicularis oculi muscle at baseline (week 0) and 2 weeks after injection of placebo or different dose of botulinum toxin type A (BoNT-A). There is a trend of increasing jitter between increasing BoNT-A doses at week 2
|
Dose (units) |
n |
Mean ± SD |
Median |
Min–Max |
|
Baseline (week 0) |
||||
|
Placebo |
4 |
28.8 ± 1.7 |
28.7 |
27.1–30.9 |
|
5 |
4 |
25.8 ± 3.1 |
25.8 |
22.9–28.8 |
|
10 |
4 |
28.1 ± 0.8 |
28.1 |
27.2–29.0 |
|
20 |
4 |
29.1 ± 2.7 |
29.1 |
26.2–32.0 |
|
Week 2 |
||||
|
Placebo |
4 |
29.3 ± 2.4 |
29.3 |
26.4–32.0 |
|
5 |
4 |
33.9 ± 4.2 |
33.9 |
29.7–38.1 |
|
10 |
4 |
35.1 ± 2.7 |
34.4 |
32.8–38.8 |
|
20 |
4 |
36.4 ± 2.5 |
37.1 |
32.9–38.3 |
Reduction in CMAP in the glabellar muscles correlates with given dose of BoNT-A
Initial CMAP ranged from an amplitude of 0.8–1.6 mV for the left and 0.9–1.7 mV for the right corrugator supercilii muscles. CMAP amplitude and area were substantially reduced after 2 weeks in all subjects who received BoNT-A. In a few cases CMAP area and amplitude further dropped from 2 to 4 weeks. The placebo group was easily identified, with CMAP approximately 100% (± 10%) of baseline at all follow-up examinations (Fig. 1).
In the standard dose-group (20-unit), CMAP amplitude was reduced to 28% of baseline at 2 weeks, with a slight increase from 2 to 4 weeks. CMAP amplitude in the 20-unit group increased to 49% at 12 weeks and further to 66% at 24 weeks, indicating a large residual treatment effect (Fig. 1).
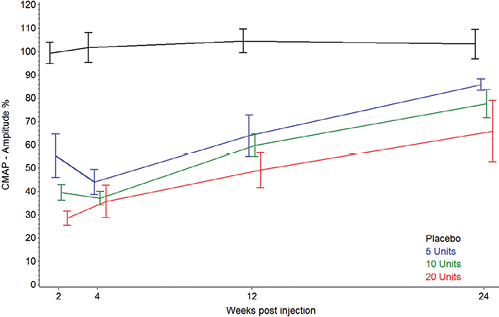
Fig. 1. Compound motor action potential (CMAP) amplitude, recorded from the corrugator supercilii muscles with stimulation of the facial nerve, as percent of baseline value over time after injection of botulinum toxin A. The mean value ± SEM in each dose-group is shown. The different dose-groups can be distinguished based on mean CMAP amplitude.
Considering the half (10-unit) and quarter (5-unit) doses, the relationship between results obtained with the 3 doses was preserved throughout the study, with 20 units consistently showing the largest reduction in amplitude and 5 units the smallest (Fig. 1). All doses differed significantly from placebo, except the 5-unit dose at week 24. The smaller differences that existed between doses were only detected statistically between 5 and 20 units at week 2. However, even with only 4 subjects per group, CMAP amplitude appears to be a useful tool in discriminating between doses (Fig. 2). As a control, CMAP from the nasalis muscle showed no signs of reduction (data not shown).
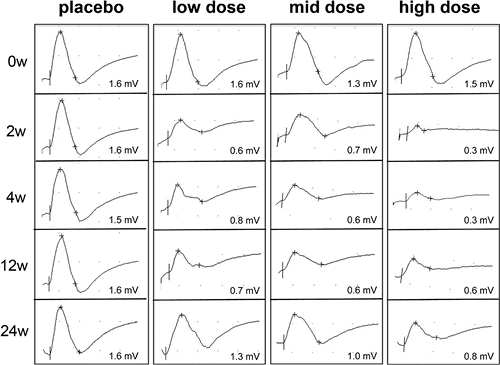
Fig. 2. Representative images of compound motor action potential of the left corrugator supercilii muscle from one subject in each of the dose-groups: placebo and 5 units, 10 and 20 units botulinum toxin A at all follow-up visits. The amplitude is given in mV.
Change in EMG pattern following BoNT-A
The EMG pattern in the placebo group was similar at baseline and all follow-up visits, without abnormal spontaneous activity at rest and maximal voluntary glabellar muscle contraction. In the 20-unit BoNT-A group, abnormal spontaneous activity, including positive sharp waves and fibrillations, occurred from 2 weeks post-injection and became more pronounced at 4 weeks, suggesting pharmacological denervation of the corrugator supercilii muscles. The denervation activity was followed by low amplitude, unstable MUPs or total block of voluntary contraction, i.e. no MUPs were detected by EMG, at 4 weeks. At 12 weeks, denervation activity was absent and ongoing reinnervation was observed with the maximal EMG activity increasing to approximately 25%, whereas maximal contraction reached only approximately 40% at 24 weeks in this group (Fig. 3). The EMG picture was similar in the 10-unit dose-groups and neither of these dose-groups obtained maximal voluntary contraction at 24 weeks (Figs 3 and 4). One person in the 10-unit dose-group had as much denervation activity (i.e. numerous fibrillations and/or positive sharp waves in all recording positions in the muscle) as in the 20-unit dose-groups, but otherwise less denervation activity was noted in the 10- and 5-unit dose-groups. Inter-individual variability was therefore important. The EMG picture was generally less affected in the 5-unit dose-group, with earlier appearance of polyphasic MUPs, indicating a more rapid reinnervation process, with maximal contraction capacity comparable to placebo at 24 weeks.
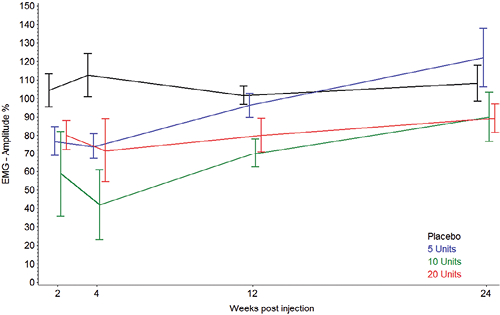
Fig. 3. Mean value of absolute change in maximal voluntary contraction (%) in the corrugator supercilii muscles of subjects in each dose-group of placebo, 5, 10 or 20 units of botulinum toxin A.
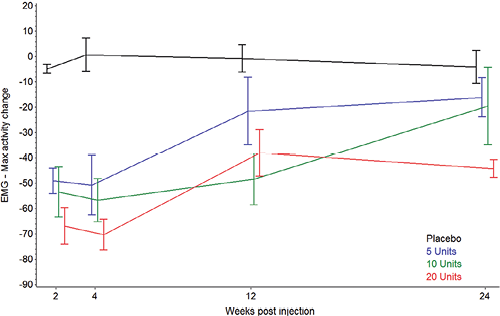
Fig. 4. Electromyography (EMG) amplitude % of baseline values in the corrugator supercilii muscles for each follow-up visit following the injection of placebo or 5, 10 or 20 units botulinum toxin A.
BoNT-A injection in the glabellar area caused disturbed neuromuscular transmission in the ocular muscles
CNE in the orbicularis oculi showed a mean MCD of 28 μs (range 23–32 μs) in the whole group at baseline. In the 12 subjects who received BoNT-A, mean MCD at 2 weeks increased significantly to 35 μs (range 30–39 μs; p < 0.001), whereas mean MCD in the placebo group was unchanged at 29 μs. When studying individual dose-groups, there was a trend of increasing jitter values at 2 week with higher doses of BoNT-A (Table II). The (mean ± SD) change in jitter values between week 0 and 2 was 1.9 ± 11.6% in the placebo group (p = 0.761), 32.8 ± 23.8% in the 5-unit group (p = 0.070), 24.9 ± 10.6% in the 10-unit group (p = 0.018) and 26.1 ± 16.8% in the 20-unit group (p = 0.053). No impulse blockings were noted in any of the groups. No subjects indicated clinical eye closure weakness at week 2, and thus the detected disturbance of neuromuscular transmission was defined as subclinical. There were no signs of pathological EMG pattern in the orbicularis oculi muscle at 2 weeks, indicating that the subclinical neuromuscular transmission failure did not cause substantial pharmacological denervation.
DISCUSSION
We report here on neurophysiological parameters in the glabellar muscles that correlate with given doses of BoNT-A. Hitherto, the only existing measure for the muscle-paralysing effect of BoNTA in the glabellar muscles is the validated clinical glabellar photo scale (6, 7). Since the pharmacological effect of BoNT-A is indeed muscle fibre paralysis, it is important to focus on real neurophysiological parameters for quantification of the functional effect, including onset, duration of action and side-effects. The photo-scale was able to separate placebo and active dose-groups, although not between the different BoNT-A doses. This study was not specifically designed to evaluate the effect photographically, and hence the photographic procedure was not fully standardized, making subtle dose differences difficult to detect. Furthermore, the wide range of wrinkle scores at baseline could have an impact on the photographic evaluation for this small sample-size. Nevertheless, our report indicates that photographs alone do have limitations in grading the objective effect of different BoNT-A doses. One previous report, using EMG, has implied that BoNT-A reduces EMG amplitude in the frontalis muscle upon voluntary contraction (14). After an initial reduction in amplitude at 2 and 4 weeks, reinnervation and/or recovery of the original NMJs starts, and the amplitude of certain MUPs increase, resulting in false high or low values of EMG amplitude depending on the reinnervation/recovery process. Even in the hands of an experienced neurophysiologist, we did not find a correlation between EMG amplitude and BoNT-A dose. This study instead demonstrated that the combination of CMAP and EMG allows for grading of different doses of BoNT-A in the glabellar muscles. These methods enable objective measurement of BoNT-A effect, even in cases where initial glabellar frown lines are almost absent and where the photographic scale fails to show an objective effect at rest.
In clinical neurophysiology, presence of denervation activity is often used to assess the efficacy of BoNT-A in injected muscles, to determine resistance due to BoNT-A antibodies. From this study, it is evident that with a standard dose injection, denervation activity appeared at 2 weeks and was maximal up to 4 weeks. In the cases of half/quarter dose, however, the amount of denervation activity was modest, except in cases of a small initial glabellar muscle mass. Thus, the muscle size and dose of BoNT-A are important factors to consider, since the between-subject variability was most probably caused by differences in these variables. The maximum effect on CMAP and EMG was obtained within 4 weeks, with indication of a more delayed maximal effect for 5 and 10 units, compared with 20 units. Furthermore, the duration of effect of BoNT-A for cosmetic indications is usually reported to be 3–4 months (21). However, these data are derived mainly from clinical studies where the observation period was terminated at specific time-points. Only a few studies have continued to, for example, 6 months: a longer-lasting effect was identified in approximately 30% of patients in examples of these prolonged studies (20). Nevertheless, we confirm that the “real” neurophysiological effect actually lasts longer, since no subject recovered their function even at 24 weeks in the 10- or 20-unit dose-groups. There was also a clear dose-response effect on recovery, with completed reinnervation/recovery in the 5-unit group at 12 weeks and incomplete/ongoing reinnervation/recovery in the 10- and 20-unit groups at the same time. Hence, our data support that muscle recovery depends on formation and maturation of new NMJs and/or recovery of old existing NMJs following pharmacological denervation of BoNT-A (22).
Intriguingly, there was a positive aesthetic effect on the glabellar frown lines with only 5 units of BoNT-A. A parallel reduction in CMAP was seen also in this quarter-dose-group, although the ability to maximally contract the corrugator muscles returned earlier. Since the toxin properties could change with a changed dilution, a higher biological effect per unit of BoNT-A in the more diluted preparation would be an explanation to why the 5-unit dose had a more pronounced clinical and neurophysiological effect than one might expect. The major aesthetic difference between the quarter vs. standard dose-groups was an accompanying paralysis of the adjacent medial part of the frontalis muscle in the 20-unit group, resulting in lateral eyebrow lift, known as “Dr Spock”. Some patients prefer this effect; however, less frontalis muscle involvement (as in the 5-unit dose-group) looks more “natural”. Since 20 units is regarded as the recommended dose of the specific BoNT-A for treatment of glabellar frown lines, this study suggests that individual tailoring of dose is beneficial, based on desired visual appearance.
Adverse effects of BoNT-A after injection in the glabellar area include a risk of blepharoptosis, occurring in 2.5–9.5% of cases (20, 23–25). We did not observe blepharoptosis and, with the exception of one case with seborrhoeic eczema, no adverse events were reported. The EMG-guided injection technique, ensuring that the BoNT-A was injected intramuscularly, could have been a significant contribution to the absence of adverse events. The disturbed neuromuscular transmission in the ocular muscle, which we observed, could have been caused by regional effect of BoNT-A. Since the orbicularis oculi is very close to the glabellar injection sites, this could be explained by a physical spread of toxin or through small intramuscular vessels. All subjects who received BoNT-A developed increased jitter in the ocular muscle and therefore this effect might be related to volume of liquid injected and not to dose. Minimizing the risk of BoNT-A diffusion is probably most dependent on correct injection in the target muscle, which is especially important in the facial area, with proximity to the vital bulbar muscles.
In conclusion, this study successfully characterized novel neurophysiological parameters for detailed evaluation of the dose-response effect of BoNT-A injection in the glabellar muscles. Reductions in CMAP amplitude and maximal EMG activity in the corrugator supercilii muscles correlate well with given dose of BoNT-A and are sensitive objective measures; for example, in the development of new BoNT-A formulations. In addition, 25% of the standard-dose BoNT-A used in cosmetic dermatology is sufficient to paralyse the glabellar muscles and result in a more natural relaxed aesthetic outcome effect than standard doses, which can result in a “frozen forehead” look.
Acknowledgements
The authors are grateful to Dr. Jan-Erik Anheller for monitoring the study and to Dr. Andy Pickett for reviewing the manuscript. The authors would also like to thank Professor Erik Stålberg for valuable scientific discussion.
Conflicts of interest: The study was an investigator-initiated study and the manuscript was prepared solely by the authors. MOA and ARP have received consulting fees from Q-MED AB. MAA is an employee of Q-MED AB, a Galderma Division.
REFERENCES


