


Barbara Maria Gaus1,2, Nina Scheiba1 and Knut Schäkel1*
1Department of Dermatology, University of Heidelberg, Im Neuenheimer Feld 440, DE-69120 Heidelberg, Germany, and 2Current Address: Department of Dermatology, Kantonsspital St. Gallen, St. Gallen, Switzerland. *E-mail: knut.schäkel@med.uni-heidelberg.de
Accepted Sep 24, 2013; Epub ahead of print Mar 27, 2014
Recurrent localised inflammatory skin reactions healing with hyperpigmentation can be induced by certain drugs and are known as fixed drug eruptions. In few cases also food was described to induce these symptoms, and the term “fixed food eruptions” was coined. Fixed food eruptions are rare, the first case was reported in 1992 (1) and the term in analogy to the clinical similarities to fixed drug eruptions was coined in 1996 (2). Since then few cases with different causes were described: cheese crisps, strawberries, lentils, lactose, quinine, cashew nuts and Japanese sand lance (3). We report the second case in which asparagus caused fixed food eruptions (4). Our patient was initially diagnosed as cutaneous lupus based on clinical appearance of the skin lesions, their development in sun-exposed areas, their seasonal manifestation and histopathology. However, asparagus was identified as the causative agent by skin testing and oral provocation. Fixed food eruptions are rare but should be included in the differential diagnosis when considering the origin of recurrent and persistent erythematous skin lesions.
CASE REPORT
A 69-year-old woman presented with a two-year history of persistent, non-pruritic inflammatory skin lesions in sun-exposed areas: face, décolleté and shoulders. Erythematous skin lesions developed in spring. These symptoms disappeared after weeks, leaving behind hyperpigmentation that resolved during the next winter. The erythematous lesions were round to annular, sharply marginated and infiltrated. Together with the histopathology revealing focal interface dermatitis with some dermal deposition of mucin (Fig. 1), initially the diagnosis of cutaneous lupus erythematosus was made and lupus erythematosus tumidus and subacute cutaneous lupus were considered. However, autoantibodies specific for nuclear antigens were negative and no deposition of autoantibodies in the tissue as studied by direct immunofluorescence was found. The detection of anti-thyreoglobulin antibodies were in accord with the patient’s previous diagnosis of Hashimoto`s disease. The skin lesions faded slowly after several weeks of topical treatment with topical glucocorticoid prednicarbate, leaving areas with hyperpigmentation (Fig. 2a).
The following year the patient reported a recurrence of the skin lesions after consuming meals of cooked asparagus (Asparagus officinalis). Prick- and patch-testing with raw and cooked asparagus in uninvolved and previously affected skin lesions were negative. An intradermal testing at a non-involved skin site with a water soluble asparagus protein extract (1:500) turned positive after 6 h and was negative in a healthy control. Lymphocyte transformation test (LTT) with titrated doses of asparagus protein remained unreactive. No asparagus-specific IgG was detectable by Western blotting and ouchterlony double immunodiffusion. Similarly, antigen-specific IgE and a basophil activation test with a titrated protein extract were negative.
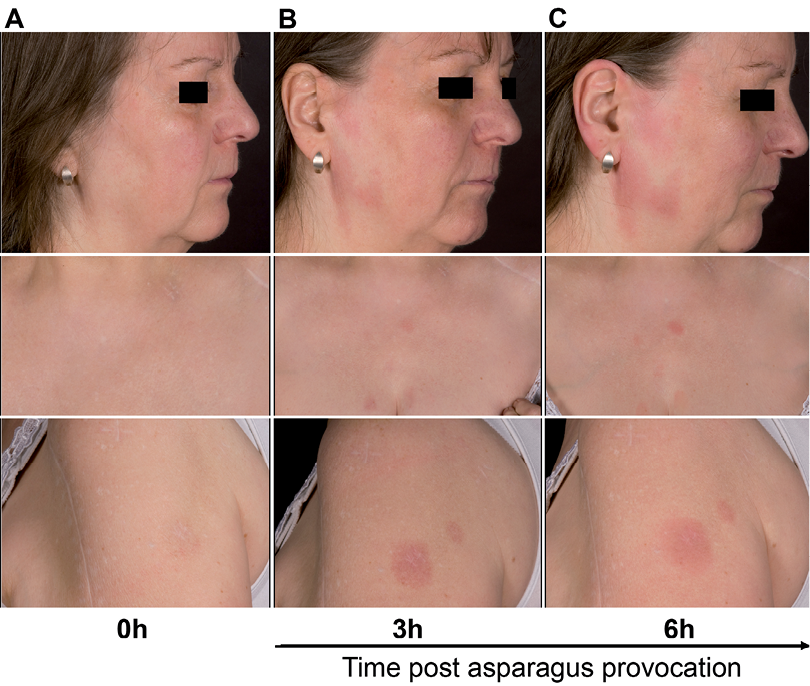
In the following spring when the patient was free of symptoms we performed an open oral food challenge with 100 g of boiled asparagus. Photos were taken from previously involved areas prior to the food challenge, and after 3 and 6 h. Fig. 2 shows the rapid development of the skin lesions in the previously affected areas and the diagnosis of a fixed food eruption caused by ingestion of asparagus was made.
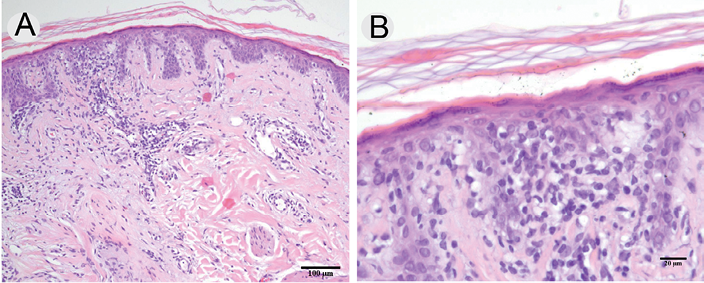
Fig. 1. Histopathologic analysis of lesional skin. The haematoxylin-and-eosin staining reveals focal interface dermatitis and dermal mucin deposition (A). The higher magnification (B) reveals the epidermotropic lymphocytic infiltration and single apoptotic keratinocytes.
DISCUSSION
Repeatedly, asparagus, either fresh or cooked, is described as a cause of protein contact dermatitis or urticaria, due to occupational contact during its canning and production. Although these patients react to cooked asparagus they tolerate the ingested vegetable. Cross reactivity to other members of the Liliaceae family members (garlic and onion) may occur (5).
Although negative in our patient, intralesional patch testing with food helps to identify the causative food. In a large retrospective study intralesional patch testing of patients with fixed drug eruptions gave positive results in 40% of the patients (6).
In analogy to fixed drug eruptions fixed food eruptions are thought to be induced by IFNγ producing CD8+ T cells. The strict recurrence of the lesions upon allergen exposure in previously affected skin areas may be due to the induction of non-migratory memory CD8+ T cells that were recently described in mice (7).
In our patient T-cell dependent tests (LTT, lesional patch test) as well as our testing for specific antibody responses remained negative. Nonetheless, the fast appearance of symptoms after oral provocation as documented here for the first time requires a strong local immune memory.
Fixed food eruptions are rare but should be included in the differential diagnosis when considering the origin of recurrent and persistent erythematous skin lesions.
REFERENCES

