


Kazuhiro Kikuchi, Daisuke Inokuma, Reine Moriuchi, Hanako Koguchi-Yoshioka, Chikako Yasui and Satoko Shimizu
Department of Dermatology, Sapporo City General Hospital, N11 W13, Chuo-ku, Sapporo 060-8604, Japan. E-mail: kikku@med.hokudai.ac.jp
Accepted Jan 14, 2014, Epub ahead of print Mar 13, 2014
Pemphigus is an autoimmune intraepidermal blistering disease (1). The autoimmune target of the antibodies is desmoglein, a cadherin-like cell-to-cell adhesion molecule found in desmosomes. In pemphigus vulgaris (PV), the main antigen is desmoglein 3 (Dsg 3), which is located on the oral mucosa and in the lower layers of the epidermis; in pemphigus foliaceus (PF), the target antigen is desmoglein 1 (Dsg 1), which is structurally located mainly in the upper epidermis (1). It is reported that pemphigus can be induced or exacerbated by radiation therapy (2–11). However, few reports have detailed the serum autoantibody concentrations before and after irradiation (6).
We report a case of PF that was well controlled for more than a year but then worsened after electron-beam radiotherapy for extramammary Paget’s disease.
CASE REPORT
A 59-year-old Japanese woman presented with pruritic scaly, crusted eruptions and flaccid bullae involving the trunk. No mucosal involvement was observed. A skin biopsy from a bulla on her back demonstrated superficial intraepidermal separation with acantholysis. Direct immunofluorescent (IF) microscopy of the lesion showed intracellular deposition of IgG and C3 at the epidermis. Enzyme-linked immunosorbent assay (ELISA) showed a circulating anti-Dsg 1 antibody concentration of 72 IU/ml (normal value <14.0), while the test for anti-Dsg 3 antibodies was negative. Routine laboratory investigations were within normal ranges.
From the above data we made the diagnosis of PF. With the application of corticosteroid ointment, the cutaneous lesions disappeared for more than a year, with the exception of a few new bullae occasionally appearing temporarily. The anti-Dsg 1 antibody concentration was no more than 72 IU/ml for about a year (Fig. 1). Thirteen months after her first visit to our hospital, we found ill-defined, 7 cm-diameter erythema with scales and erosion on her external genitalia. Extramammary Paget’s disease was diagnosed by the histopathological feature of typical Paget cells in the epidermis (figure not shown). She received electron-beam irradiation (total dose of 52.5 Gy) on the vulva for a month since she refused surgical resection. The eruptions on the external genitalia resolved, leaving post-radiation erosions. One month after the radiation therapy, the erosions on the external genitalia were aggravated. Subsequently, dozens of bullae, erosions and erythematous macules of a few millimeters to 5 cm in diameter appeared on her trunk (Fig. 2). Simultaneously, the anti-Dsg1 concentration rose strikingly to 4,307 IU/ml from 101 IU/ml (Fig. 1). We performed a biopsy again from a blister on her back and found the pathological features consistent with PF. We administered 25 mg/day (0.5 mg/kg/day) of oral prednisolone. The skin lesions healed gradually, leaving post-inflammatory hyperpigmentation, and the development of new blisters has stopped. As for the extramammary Paget’s disease, no recurrence has occurred. Prednisolone was tapered without relapse of skin lesions. Anti-Dsg 1 concentrations have decreased (Fig. 1). At 9 months after aggravation, she has continued the prednisolone at a 10 mg/day maintenance dose.
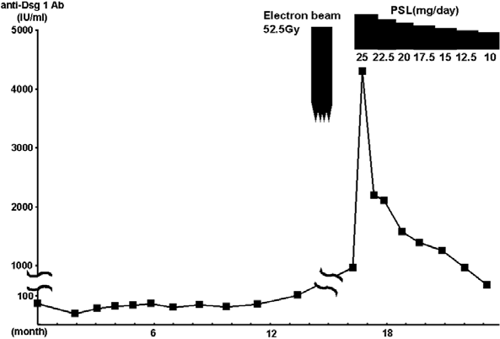
Fig. 1. Serum anti-Dsg 1 antibody concentration of the patient. At about 1 month after electron-beam irradiation, the anti-Dsg1 concentration is strikingly elevated. Treatment with oral prednisolone (PSL) decreased the anti-Dsg 1 concentration.

Fig. 2. Pruritic scaly, crusted eruptions and flaccid bullae involving the trunk at the exacerbation after electron-beam irradiation of the vulva.
Discussion
Twenty-three previous cases of pemphigus occurring or exacerbating after irradiation therapy for malignant neoplasms have been reported (2–11). As for PF, only 4 such cases have been reported (8–11).
The first case of PF after radiation was described by Tagami et al. (9) in 1976. The case was a 41-year-old Japanese man who underwent cobalt therapy for a thymic tumour. Six months later, he developed an eruption diagnosed as pemphigus. Although the author did not describe the type, we and other reviewers interpreted the case as consistent with PF, based on the clinical photos and the histopathological findings.
Low & Keeling (8) reported the case of a 70-year-old Caucasian woman with PF who received cobalt 60 radiation for laryngeal squamous cell carcinoma. Ambay &Stratman (10) reported the case of a 92-year-old woman with PF followed by radiation therapy for left breast carcinoma. Cianchini et al. (11) described the case of a 70-year-old woman with PF following radiation for an adenocarcinoma of the left breast. In these 3 cases, the PF occurred one month, 3 months, and 12 months after irradiation, respectively. All 4 cases had no history of blistering skin disorder before the irradiation.
The present PF case is different from the previous 4 cases of irradiation-induced PF. None of the other cases had a history of blistering disease before irradiation but, in our case, preexisting, well-controlled PF drastically worsened (8–11). In PV, 3 cases which had history of pemphigus were reported to show exacerbation or recurrence after irradiation (4–6). In these cases of PV, as in our case, mucocutaneous lesions had been cured or well controlled for a long period; however, aggravation appeared after irradiation (4–6). The serum anti-Dsg antibody concentration was reported in only one of these cases. The case showed the elevation of serum anti-Dsg 1 antibodies from negative to 26.94 IU/ml after irradiation (6). From these cases, irradiation is considered to be an exacerbating factor for pemphigus (4–6).
It is unclear how radiation therapy acts as a trigger to induce or exacerbate pemphigus (8–11). Pemphigus is induced by the autoantibodies for Dsg (1); therefore, enhancement of the antigen-antibody reaction may be a key to explaining the aggravation of pemphigus by irradiation. In fact, in our patient, the recurrence of eruptions and the markedly increased serum anti-Dsg1 antibody concentration appeared simultaneously. This is compatible with several theories proposed previously. One theory is that radiotherapy itself changes antigenic properties and induces autoantibody production through the alteration of the antigen with unmasking (2, 12). Also in the present case, electron-beam might damage the epidermis in and outside of irradiation field and induce unmasking and alteration of the antigen, resulting in establishment of potential basis for exacerbation of PF. Another possible explanation is that even patients who recently developed pemphigus after irradiation may already have had circulating low-titre autoantibodies, and tissue damage from the radiotherapy may have enhanced the deposition of those antibodies, i.e., blood vessel permeability could have increased and autoantibodies could have diffused more easily (2, 12). These hypotheses may explain the mechanism for onset and exacerbation of pemphigus. In all the previous cases of pemphigus, including our case, the eruptions started from the areas of irradiation and then spread to other areas (2–11). Such a clinical course indicates that irradiation influences the formation of eruptions in pemphigus.
We reported a case of PF that had been well controlled and had had stable serum autoantibody concentrations but which was then exacerbated by electron-beam irradiation. Our observations demonstrate the necessity of precautions against the exacerbation of pemphigus after irradiation. In such cases, the transitions in autoantibody value should be analysed in detail during and after the radiation therapy. It is also important to be aware that even in cases with no history of blistering diseases, pemphigus can occur after irradiation.
REFERENCES

