


Ingela Ahnlide, Kari Nielsen and Mats Bjellerup
Department of Dermatology, Helsingborg Hospital, Department of Clinical Sciences, Faculty of Medicine, Lund University, Lund, Sweden
The increasing incidence of melanoma prompts a need for efficient management of this patient group. In this study, we use the number needed to excise (NNE), as a measurement of the efficiency of diagnosing melanoma. From January 2009 to December 2012, postoperative records from all patients were prospectively registered. All excised tumours with the histopathological diagnosis of naevus, melanoma or seborrhoeic keratosis were included. NNE values, both excluding and including seborrhoeic keratosis, changes over time, as well as patient- and tumour-related factors influencing NNE were determined. In total, 1,717 cases were included. The overall NNE value was 6.5, and the value fell significantly (r = 0.959, p = 0.041) during the 4-year study period from 8.2 to 4.8. NNE values decreased with increasing patient age to 1.8 in patients ≥ 80 years of age. The overall NNE value including seborrhoeic keratosis was 6.8. Key words: melanoma; naevus; dysplastic naevus; melanoma in situ; seborrhoeic keratosis.
Accepted Feb 20, 2014; Epub ahead of print Feb 27, 2014
Acta Derm Venereol
Ingela Ahnlide, Department of Dermatology, Helsingborg Hospital, Clinical Sciences, Lund University, SE-251 87 Helsingborg, Sweden. E-mail: ingela.ahnlide@skane.se
The incidence of skin cancer is increasing in fair skinned populations (1), and is now one of the most common reasons for presentation at hospital dermatology departments. Early diagnosis is important as only early diagnosis and surgical treatment can prevent metastatic disease. The diagnosis of melanoma is straightforward in typical cases. Nevertheless, there is a grey zone of naevi, lentigines and seborrhoeic keratoses (SK) with atypical clinical presentation, in which complete excision is necessary to establish a diagnosis. The size of this grey zone, however, is dependent on diagnostic acumen. The number needed to excise (NNE) is calculated as the number of excised pigmented tumours divided by the number of excised melanomas. The NNE value should obviously be kept low, since a low NNE value means a low rate of unnecessary excisions of benign lesions. This effort must not, however, result in missed melanomas.
In this study, we analysed NNE values in one medium-sized Swedish dermatology department over a 4-year period. Changes in NNE values over time, as well as patient- and tumour-related factors influencing NNE were assessed. The NNE values are presented excluding SK and including SK.
MATERIALS AND METHODS
The study was performed at the Department of Dermatology at Helsingborg Hospital, Helsingborg, Sweden. Six consultants and 4 residents in dermatology were working at the department during the study period (January 2009 to December 2012). The study was approved by the Regional Ethical Review Board in Lund, Sweden (2011/195).
During the study, all skin tumours surgically excised at the department were consecutively registered. The registry was integrated in a computerized patient file system (Melior®, Siemens AB, Upplands Väsby, Sweden) as a standardized patient file. The sex and age of patients, as well as tumour location and histopathological diagnosis were recorded for all patients undergoing surgery, but only excised tumours with the histopathological diagnosis of common naevus, dysplastic naevus, melanoma in situ (including lentigo maligna), invasive melanoma or SK were included in the study. Wide-local excisions, excisions of melanoma metastases, local melanoma recurrences, as well as other benign or malignant skin tumours were excluded.
Data from the registry were extracted and processed using QlikView® (QlikTech International AB, Lund, Sweden). Microsoft Excel® (Microsoft Corp., Seattle, WA, USA) and PASW Statistics 18 (SPSS Inc., Chicago, IL, USA) were used for the statistical analyses. For analysis of changes over time for NNE and numbers of excised melanomas and dysplastic naevi, linear regression was used. The Chi-square test was used for comparing excised melanomas and naevi in men and women and for comparing location of melanoma in men and women.
The NNE values were calculated by dividing the number of excised pigmented tumours (common naevus, dysplastic naevus, melanoma in situ and invasive melanoma) by the number of excised melanomas. However, separate NNE calculations were also made including SK as a benign pigmented tumour. In all calculations, the variable “melanoma” included both melanoma in situ and invasive melanoma.
Changes in NNE values over time, as well as NNE values in relation to sex, age of patient and body location were evaluated.
RESULTS
A total of 4,986 primary excisions of skin tumours were performed at the Department of Dermatology, Helsingborg Hospital, during the study period. Twenty-six cases were excluded because of an invalid report or missing data. Excised malignant tumours included 2,093 basal cell carcinomas (BCC), 596 squamous cell carcinomas (SCC) and 252 melanomas. In total, 1,717 cases met the inclusion criteria and were included in the study, whereof 252 were melanomas (125 in situ and 127 invasive), 1,395 were naevi (of which 563 were dysplastic) and 70 were SK. The median patient age was 44.0 years (range 7–99 years). Mean and median ages at diagnosis for the included diagnoses are shown in Table I.
Table I. Numbers of excised naevi, melanomas and seborrhoeic keratoses. Mean and median age (years) at diagnosis split by histopathological diagnosis
|
n |
Mean age |
Median age |
|
|
Common naevus |
832 |
39.2 |
36.0 |
|
Dysplastic naevus |
563 |
48.6 |
47.0 |
|
Melanoma in situ |
125 |
66.2 |
68.0 |
|
Invasive melanoma |
127 |
64.0 |
66.0 |
|
Seborrhoeic keratosis |
70 |
65.8 |
72.0 |
|
Total |
1,717 |
47.2 |
44.0 |
Excision margins were free of tumour cells in 98.5% of all included excised tumours.
Number needed to excise values, seborrhoeic keratosis not included
The overall NNE value, SK not included, during the study period was 6.5. The NNE values decreased from 8.2 in 2009 to 4.8 in 2012, with a yearly decrease rate of 1.05 (r = 0.959, p = 0.041) (Fig. 1).
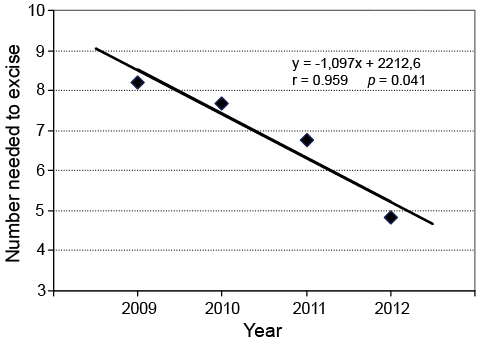
Fig. 1. Trend over time of number needed to excise, not including seborrhoeic keratosis.
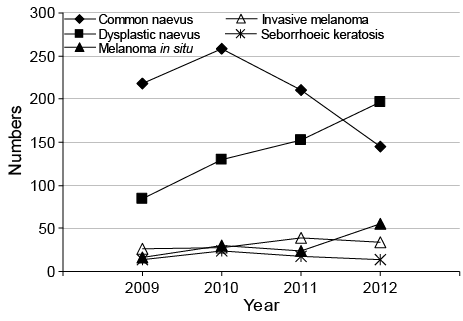
The trends over time of the total numbers of excised lesions are presented in Fig. 2. Melanomas (the sum of melanoma in situ and invasive melanoma) (r = 0.991, p = 0.034) and dysplastic naevi (r = 0.966, p = 0.008) were increasingly excised during the study period.
The NNE values varied markedly with body location. The NNE value (including both sexes) was highest for the trunk (10.4) and lowest for the upper extremities (2.4). In the head and neck region, the NNE value was 4.2 and on the lower extremities it was 4.3. There was a significant difference in body location of excised melanomas between the sexes (p < 0.001), with a predominance of melanomas excised on the trunk in men (Fig. S1a1), and a more even distribution between the locations in women (Fig. S1b1). The NNE values for different body locations were also calculated for men and women separately. The NNE values for different body locations as well as body location of melanomas (including invasive melanoma and melanoma in situ) and naevi (including common and dysplastic naevus) for men and women are shown in Fig. S11. The highest NNE value (18.9) was seen for trunk location in women (Fig. S1b1). The overall NNE value was higher for women than for men, at 7.7 and 5.6, respectively and there was a significantly higher number of excised naevi and lower number of excised melanomas in women compared to men (p = 0.006). The NNE values decreased with increasing age, as shown in Fig. 3. In the age group 0–20 years, the NNE value was 153, while in the age group ≥ 80 years, NNE was 1.8.

Number needed to excise values, seborrhoeic keratosis included
Fig. 4 shows the numbers of excised naevi (including common and dysplastic naevus), melanomas and SK in different age groups.
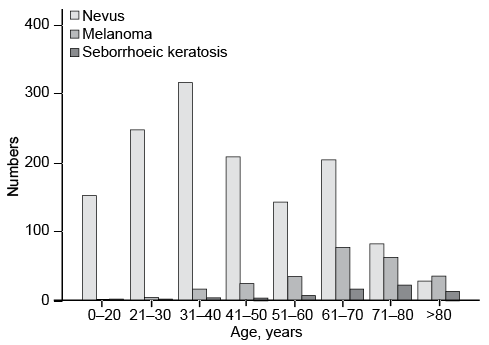
In total, 70 SK were excised, representing 4.1% of all excised lesions included in the study (see Table I). In the age group ≥ 60 years, the rate of excised SK was 9.5% (data not shown).
The overall NNE value including SK was 6.8. In the age group 71–80 years, the inclusion of SK in the calculation changed the NNE value from 2.4 to 2.8, and in the age group ≥ 80 years, this value changed from 1.8 to 2.2 (data not shown).
DISCUSSION
The increase in skin cancer incidence demands that all aspects of diagnosis and treatment needs more scrutiny if safe and cost-effective care is to be delivered (1). We recently published a paper about the accuracy of clinical skin tumour diagnosis in a dermatological setting (2). We concluded that sensitivity and positive predictive values (PPV) were very high for malignant tumours as a group, 98.0% and 85.3%, respectively. PPV were highest for BCC and lowest for melanoma, explained by the need for larger margins of diagnostic safety with the latter. Our data also indicated a better diagnostic performance by dermatologists than by other specialists (GPs, GPs with a special interest in skin cancer, plastic surgeons and general surgeons). We concluded that dermatologists should be placed on the front line of skin tumour diagnosis and treatment.
The present study was restricted to excised pigmented skin tumours only. We have chosen NNE as the main outcome measure, which allows comparison with previous studies in the same field. NNE has been calculated as described earlier, both excluding and including SK. In total, 1,717 cases of excised pigmented skin tumours were included during the 4-year study period. Evaluation of NNE values excluding SK will be discussed first.
We showed that NNE values fell significantly from 8.2 to 4.8. Several factors might contribute to the decreasing NNE values. One hypothetical explanation for the falling NNE values in our department is that diagnostic performance improved among the participating dermatologists. Dermoscopy has been practiced by all physicians at our department for more than 10 years. We have determinedly and continuously tried to improve our skills in dermoscopy. This was achieved by repeated joint feedback sessions/audits evaluating the preoperative dermoscopy photographs of excised lesions, enrolment in dermoscopy courses for both residents and senior consultants and daily continuous education in dermoscopy for all residents; during daily clinical work, residents have the opportunity to consult specialists about diagnostic difficulties. Three of the specialists attended extensive, formal courses in dermoscopy during the study period. It is reasonable to assume that a great part of the decreasing NNE values can be attributed to increased dermoscopy use and consequently, to a higher diagnostic skill to correctly distinguish malignant lesions from benign lesions. In a prospective study on two groups of dermatologists, Carli et al. (3) showed that the implementation of dermoscopy in one group improved the ratio of excised malignant lesions vs. benign lesions. Another finding speaking in favour of this hypothesis is the increase in excised dysplastic naevi relative to excised common naevi shown over time in our study. This is also in line with the findings by Carli et al. (3), who saw an increased rate of excised “problem naevi” among dermoscopy users compared with non users.
Our findings of falling NNE values over time are in line with those of a much larger, retrospective, multicentre investigation that included different specialities by Argenziano et al. (4). They found decreasing NNE values during the 10-year period they studied, presenting the best NNE value (6.8) at the end of the study period. The decrease in NNE values was found only in specialized skin cancer clinics and was due to increased melanoma excisions. In non-specialized clinics, they showed that the NNE values remained unchanged over time (4). We could also verify other data reported by Argenziano et al. (4); in both their and our study NNE values were shown to be higher for women than men and highest for lesions on the trunk. In our study the highest NNE value was found on the trunk in women where the NNE value was as high as 18.9, compared with 7.4 in men. The lower NNE value on the trunk in men compared to women was attributed to a higher number of excised melanomas in this location in men, where an approximately equal number of naevi were excised.
One explanation for higher NNE values on the trunk might be attributed to the distribution of clinically dysplastic naevi, which often mimic early melanomas. As previously shown in a Swedish population (5), these naevi are mostly found on the trunk and not on the upper limbs, rendering higher rates of grey zone lesions on the trunk and low rates on the upper extremities. Moreover, NNE values decreased with increased age, peaking at 153 at 0–20 years, and falling for each 10-year age interval, with the lowest NNE value being 1.8 for the age group ≥ 80 years. In other words, in the age group ≥ 80 years, more than every second excised melanocytic skin lesion was a melanoma. This finding is in line with a previous study (6) that showed that the total body naevus count decreases with increasing age, and the age of the patient has to be considered when managing patients with pigmented lesions, since the risk of new or changing pigmented lesions being melanomas is much higher in the elderly (7).
Is NNE excluding SK a correct way of measuring the efficiency of diagnosing pigmented skin tumours? We do not think so, since one of the most common pigmented skin tumours, especially in the elderly, is omitted, namely SK. This is illustrated by a retrospective study of excised pigmented lesions, where Marks et al. (8) found that the ratio of excised SK to melanoma exceeded the ratio of naevi to melanoma after the age of 60 years. With increasing age, the differential diagnosis to melanoma includes an increasing rate of SK, suggesting that to obtain a correct picture of NNE values and to make NNE values comparable between studies, different clinical settings and different age groups, SK should be reported. The rate of excised SK is particularly useful as a marker of diagnostic accuracy of pigmented skin lesions, since excision is never the first-line treatment, not even for cosmetic or mechanical reasons. If the clinical diagnosis is certain and treatment for some reason eligible, then other treatment options are preferred e.g. curettage.
In the majority of previous studies on NNE values, excised SK are not included in the calculations, and even not reported. However, two studies of NNE values in primary health care in Australia included excised SK (9, 10). In the study by English et al. (9), the total rate of excised SK was 30%, and in the age group ≥ 70 years, 72% of the excised lesions were SK. The corresponding values in the study by Hansen et al. (10) were 24% in the whole study population and 52% in the age group ≥ 60 years. This should be compared with our study, with a low total rate of excised SK of 4.1%, and in the age group ≥ 60 years, a rate of 9.5%.
One limitation of our study was the lack of a control group. Another limitation, shared with most similar studies on NNE, was that NNE values were based on selected histopathological diagnoses and excluded e.g. pigmented BCCs. To overcome these limitations and be able to compare NNE studies, an international consensus on how to correctly calculate NNE is needed.
In summary, we conclude that NNE values can be reduced to very acceptable levels in a specialized dermatological department with resources spent on the continuous improvement of diagnostic abilities. We also confirm previously reported patient-related factors influencing the obtained NNE values. New or improved diagnostic tools to rule out melanoma more easily among ambiguous pigmented lesions on the trunk, especially among women, could result in a decrease in NNE values of the trunk.
ACKNOWLEDGEMENTS
This study was supported by Skane County Council’s Research and Development Foundation, Thelma Zoéga Foundation and Stig and Ragna Gorthon Foundation.
The authors wish to thank Dick Nelson for assistance with the statistical analysis and Lars Gustavsson for technical support. We also wish to thank colleagues and staff at the Department of Dermatology, Helsingborg.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1831
REFERENCES


