


Shu Sasai1, Ryuhei Nishikawa2, Ayaka Ohzono2, Taihei Hayakawa2, Daisuke Tsuruta2,3, Kazuhiro Kudoh4, Tsuyoshi Kikuchi5, Masahiro Hashiguchi6, Chika Ohata2, Minao Furumura2, Hiroshi Koga2, Norito Ishii and Takashi Hashimoto2*
1Division of Dermatology, South Miyagi Medical Center, Miyagi, 2Department of Dermatology, Kurume University School of Medicine, and Kurume University Institute of Cutaneous Cell Biology, 67 Asahimachi, Kurume, Fukuoka 830-0011, 3Present address: Department of Dermatology, Osaka City University Graduate School of Medicine, Osaka, 4Division of Dermatology, Kesennuma City Hospital, Miyagi, 5Cosmic Corporation Co. Ltd, Business Development and Marketing Department, and 6Medical & Biological Laboratories Co. Ltd, Marketing & Technical Support Department, Tokyo, Japan. E-mail: hashimot@med.kurume-u.ac.jp
Accepted Mar 12, 2014; Epub ahead of print Mar 25, 2014
Bullous pemphigoid (BP) is characterized clinically by oedematous erythemas and tense, histopathologically subepidermal blisters with eosinophilic infiltration, and immunologically by immunoglobulin G (IgG) autoantibodies to BP230 and BP180 (1, 2). BP230 mediates the interaction between intermediate filaments and BP180 (3). Since BP230 has a cytoplasmic localization, and IgG antibodies cannot access this in intact cells, the production of IgG autoantibodies to BP230 is thought to be a secondary event. In contrast, as BP180 is a transmembrane protein, IgG autoantibodies to BP180 are considered pathogenic (1).
The aim of this study was to characterize 2 BP patients, whose sera originally reacted only with BP230.
CASE REPORTS
Patient 1. An 82-year-old Japanese woman developed diffuse erythemas and multiple tense blisters over her whole body (Fig. 1a). Indirect immunofluorescence (IF) showed circulating IgG autoantibodies reactive with the epidermal side of 1M NaCl-split skin (Fig. 1b). Skin biopsy was not performed. A clinical diagnosis of generalized BP was made. A combination of topical corticosteroid and oral doxycycline and epinastine hydrochloride resulted in complete remission.
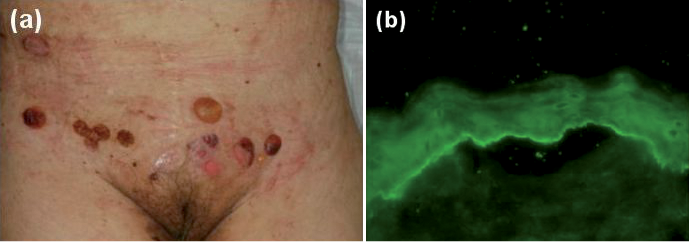
Fig. 1. (a) Clinical features on the abdomen of patient 1. (b) Indirect immunofluorescence (IF) using 1M NaCl-split skin in patient 1 (×100) (For complete figure see Fig. S11).
Patient 2. An 84-year-old Japanese woman presented with oedematous erythemas and tense blisters exclusively on the dorsal side of her feet, which had been present for 1 month (Fig. S1c1). IgG antibodies reacted with the epidermal side of 1M NaCl-split skin (Fig. S1d1). A clinical diagnosis of localized BP was made. However, patient 2 was lost to follow-up. Skin biopsy was not performed.
Both patients were negative for BP180, but positive for BP230 on IgG ELISA kits for BP230 and BP180 produced in Japan (Mesacup, Medical & Biological Laboratories (MBL), Nagoya, Japan) (4, 5), (Table SI1). To verify this result, the sera was also examined with different IgG ELISA kits produced in Germany (Euroimmun Co. Ltd, Luebeck, Germany) (6, 7). Using these ELISA kits, patient 1 was positive for both BP180 and BP230, whereas patient 2 was negative for both antigens (Table SI1).
The BP230 ELISA kit produced by MBL uses full-length bacterial recombinant proteins (RPs) of both N- and C-terminal domains of BP230, while the ELISA kit produced by Euroimmun uses bacterial RP of partial C-terminal domain of BP230. Therefore, to study the reactivity with BP230 in more detail, we performed novel BP230-domain-specific ELISAs (Hayakawa et al., manuscript in preparation) (Table SI1). Bacterial RPs of N- and C-terminal domains of BP230 were prepared, as described previously (8). In these ELISAs, patient 1 was negative for the N-terminal domain, but strongly positive for the C-terminal domain, of BP230 (Table SI1). Patient 2 was strongly positive for the N-terminal domain and intermediately positive for the C-terminal domain.
The presence of IgE antibodies was further examined by novel techniques (Ohzono et al., manuscript in preparation) (Table SI1), utilizing commercially available BP180 and BP230 ELISA kits for IgG antibodies (MBL). Two additional BP patients (patients 3 and 4) and 2 healthy individuals were used as controls. This study showed that, while IgE anti-BP180 antibodies were negative in both patients 1 and 2, IgE anti-BP230 antibodies were slightly positive in patient 1 and strongly positive in patient 2.
Immunoblotting of normal human epidermal extract showed positive IgG reactivity with the 230 kDa BP230 in patient 2, but not in patient 1 (Fig. S1e1). In immunoblotting analyses of RPs of monomeric NC16a domain and C-terminal domain of BP180, both patients did not react with either RP (Fig. S1f and g1). IgG antibodies in both patients did not show any positive results in immunoblotting analyses using normal human dermal extract, or concentrated HaCaT cell culture supernatant and purified human laminin-332.
DISCUSSION
The 2 patients with BP showed distinct results between 2 different commercially available ELISA kits for both BP230 and BP180.
Taking into account the difference in RPs used in the N- and C-terminal BP230 ELISA and C-terminal BP230 ELISA, one can explain the discrepant results that patient 2 was negative in the C-terminal BP230 ELISA, but positive in the N- and C-terminal BP230 ELISA, while patient 1 was positive on both ELISAs. Namely, patient 1 may have high antibodies to the partial C-terminal domain RP of BP230 used in the C-terminal BP230 ELISA, resulting in high relative units in the C-terminal BP230 ELISA. In contrast, patient 2 may have high antibodies to the N-terminal domain of BP230, but low antibodies to the C-terminal domain RP used in the C-terminal BP230 ELISA, resulting in a high index in the N- and C-terminal BP230 ELISA and negative relative units in the C-terminal BP230 ELISA.
Concerning BP180 ELISA kits, MBL ELISA uses monomeric NC16a RP of only one NC16a domain, while Euroimmun ELISA uses tetrameric NC16a RP of 4 tandem repeats of NC16a domain, indicating higher sensitivity in tetrameric NC16a ELISA. This explains well the discrepant result that patient 1 was negative in monomeric NC16a ELISA, but weakly positive in tetrameric NC16a ELISA.
As a mechanism of subepidermal blister formation in BP, binding of anti-BP180 antibodies to BP180 is considered to cause inflammation, internalization of BP180 and signalling events, resulting in dermo-epidermal separation (1, 9, 10). In contrast, circulating IgG anti-BP230 antibodies are thought to be secondary antibodies.
In the present study, patient 2 showed autoantibodies to BP230, but not to BP180, in 2 different ELISAs. Negative reactivity with BP180 was also supported by the results in immunoblotting using epidermal extract, concentrated culture supernatant of HaCaT cells and 2 BP180 RPs. These results tempted us to speculate that anti-BP230 antibodies, at least in patient 2, were pathogenic. Thus far, 3 BP cases with generalized skin lesions, similar to case 1 in this study, were reported to show only anti-BP230 antibodies (11). In addition, several cases of localized BP or pemphigoid nodularis, similar to case 2 in this study, were reported to react only with BP230 (12, 13).
A pathogenic role of anti-BP230 autoantibodies was also suspected in patient 1 when reactivity was first found only with BP230 in the study using the C-terminal BP230 ELISA and monomeric NC16a ELISA. However, the tetrameric NC16a ELISA, with higher sensitivity to BP180, detected relatively low reactivity with BP180 in patient 1. Thus, IgG anti-BP180 autoantibodies may cause the extensive skin lesions in patient 1.
The results of this study indicate that simultaneous use of 2 different ELISA kits may be helpful in making diagnoses and understanding the pathophysiology in individual patients with BP. Further extensive comparative studies between the 2 commercially available ELISA kits for both BP180 and BP230 are in progress.
Pathogenic IgE antibodies to BP antigens were reported to be present in BP sera (14, 15). Therefore, we also performed a preliminary study for IgE antibodies to BP180 and BP230 using a novel technique that detected weak and strong IgE reactivity with BP230 in patients 1 and 2, respectively, while both patients showed negative IgE reactivity with BP180. Interestingly, this reactivity profile for IgE antibodies was similar to that for IgG antibodies. The high IgE antibodies to BP230 may play a role in blister formation in patient 2. However, while patient 1 showed extensive skin lesions, patient 2 showed minimum skin lesions restricted to the dorsal side of the feet, indicating a relatively low pathogenic activity of IgE anti-BP230 autoantibodies. A more extensive study of IgE antibodies to BP180 and BP230 in patients with BP, which may elucidate the pathogenic role of IgE antibodies in BP, is in progress in our institute.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1848
REFERENCES


