


Anna Hillert Winther and Anette Bygum*
Department of Dermatology and Allergy Centre, Odense University Hospital, DK-5000 Odense C, Denmark. *E-mail: anette.bygum@rsyd.dk
Accepted Mar 20, 2014; Epub ahead of print Apr 2, 2014
Median canaliform nail dystrophy is an unusual condition of the nail, most often affecting the thumb (1). It is characterized by a longitudinal split or canal in the nail with small transversal fissures, in a fir-tree configuration. The condition is diagnosed based on its clinical features (2, 3). While the underlying mechanism is unknown, it has been suggested that median canaliform nail dystrophy is the result of a temporary defect in the nail matrix, following dyskeratinization or focal infection, or alternatively is due to self-inflicted trauma to the nail or nail bed. Familial cases have been reported (2, 3). Spontaneous remission is often seen, but the condition can be recurrent (1).
Three case reports of median canaliform nail dystrophy as an adverse effect of acne treatment with isotretinoin (13-cis-retinoic acid) have been published (3–5). Alitretinoin (9-cis-retinoic acid), on the other hand, is used in the treatment of severe chronic hand eczema (6–8). We report here a case of median canaliform nail dystrophy that developed in a patient treated with alitretinoin for severe hand eczema.
CASE REPORT
A 53-year-old man, with a history of chronic dyshidrotic and keratotic hand and foot eczema, developed nail changes after receiving alitretinoin treatment for 16 months. The changes were most prominent on the thumbnails, where he presented median longitudinal ridging and splitting with transversal fissures. There were both horizontal and fir-tree shaped fissures among the transversal changes. Minor nail plate dystrophy was seen on the other nails, and all nails on both hands had ragged cuticles and enlarged lunulae.
The patient’s eczema was diagnosed in 1998 and initial treatment with topical and systemic steroids, azathioprine, methotrexate, acitretin, cyclosporine or mycophenolate mofetil had either adverse effects or worked insufficiently. In 2008, alitretinoin became available on the Danish market and it was prescribed to the patient in 2009. He initially received 30 mg daily, but developed adverse effects, such as headache, vertigo and universal dry skin with pruritus, after less than 1 month’s treatment. A reduction in the dose was tried, first to 30 mg every third day, and later to 10 mg daily, but the adverse effects remained and the treatment was discontinued after 6 months. In 2012, the patient’s eczema worsened and alitretinoin was reintroduced at a daily dose of 10 mg. After being treated with alitretinoin for 16 months, the patient developed the characteristic nail findings, which were diagnosed as median canaliform nail dystrophy (Fig. 1A). The patient had no personal or family history of nail diseases. He denied self-inflicted trauma to the nail. The nail folds were neither red nor swollen, but the cuticles on all fingers were retracted and torn, which they had been since the onset of his hand eczema. The patient had enlarged lunulae on all nails. This condition did not disappear after the discontinuation of alitretinoin. He did not receive other medications known to interact with alitretinoin and he had normal blood tests apart from slightly elevated lipids. Alitretinoin was discontinued, and follow-up visits after 3 and 6 months documented outgrowth of normal nail on both thumbs (Fig. 1B and 1C). At present the patient is being treated with cyclosporine, 150 mg daily, and his hand eczema is in remission.
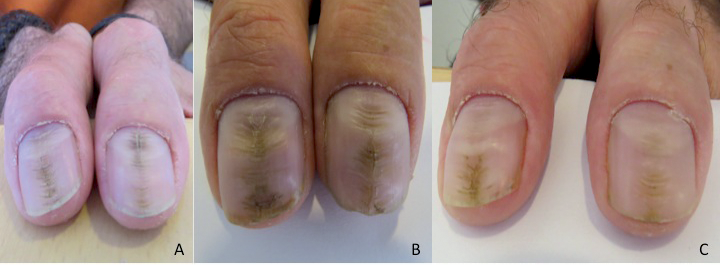
Fig. 1. (A) Median nail dystrophy of both thumbs after 16 months’ treatment with alitretinoin and outgrowth of normal nails (B) 3 months and (C) 6 months after discontinuation of treatment.
DISCUSSION
The pathogenesis of median canaliform nail dystrophy is unknown, but it is believed to be caused by a dyskeratotic reaction in a predisposed individual (4, 5). Idiopathic cases are most often self-healing, but when persistent, excision of the nail matrix abnormality can be tried. When caused by medication, the treatment is discontinuation of the suspected drug.
In the reported cases of isotretinoin-induced median canaliform nail dystrophy, nail changes occurred after 6–8 weeks, and attenuated when treatment was discontinued (3–5). Alitretinoin, like other licensed retinoids, affects cell formation, cell differentiation, keratinization, apoptosis and immune regulation, and therefore, adverse effects could be expected to be similar to those of isotretinoin (7). Several adverse effects have been described for alitretinoin, such as headache, blushing, elevated blood lipids, hypothyroidism, depression, and dryness of the skin and lips (7, 8). As the drug is relatively new, reports of novel adverse effects, especially of long-term treatment, may be expected.
In this case, the nail changes occurred after approximately 16 months of treatment, and the patient had not developed median canaliform nail dystrophy during his previous alitretinoin treatment period of 6 months. The longitudinal nail ridges support the patient’s claim that changes were not self-inflicted, as self-inflicted trauma most often causes transverse changes (2). It was deemed improbable that the nail changes were caused by the patient’s chronic hand eczema, as he had not experienced similar changes in the 15 years since diagnosis. Alitretinoin treatment was discontinued after the nail changes were discovered, and follow-up visits after 3 and 6 months demonstrated outgrowth of normal nails on both thumbs. While idiopathic cases of median canaliform nail dystrophy can go into spontaneous remission, the immediate discontinuation response makes it unlikely in this patient.
In conclusion, we suggest that median canaliform nail dystrophy is an adverse effect of long-term treatment with alitretinoin, which may limit the usefulness of this drug in the treatment of chronic hand eczema.
The authors declare no conflicts of interest.
REFERENCES

