


Alexander Börve1, Johan Dahlén Gyllencreutz2, Karin Terstappen2, Eva Johansson Backman3, Anette Aldenbratt4, Markus Danielsson3, Martin Gillstedt3, Carin Sandberg3 and John Paoli3
Departments of 1Orthopaedics and 3Dermatology and Venereology, Sahlgrenska University Hospital, Institute of Clinical Sciences at the Sahlgrenska Academy, University of Gothenburg, Gothenburg, 2Department of Dermatology and Venereology, Skaraborg Hospital, Skövde and 4Mölnlycke Primary Health Care and Research Center, Mölnlycke and Department of Public Health and Community Medicine/Primary Health Care, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
In this open, controlled, multicentre and prospective observational study, smartphone teledermoscopy referrals were sent from 20 primary healthcare centres to 2 dermatology departments for triage of skin lesions of concern using a smartphone application and a compatible digital dermoscope. The outcome for 816 patients referred via smartphone teledermoscopy was compared with 746 patients referred via the traditional paper-based system. When surgical treatment was required, the waiting time was significantly shorter using teledermoscopy for patients with melanoma, melanoma in situ, squamous cell carcinoma, squamous cell carcinoma in situ and basal cell carcinoma. Triage decisions were also more reliable with teledermoscopy and over 40% of the teledermoscopy patients could potentially have avoided face-to-face visits. Only 4 teledermoscopy referrals (0.4%) had to be excluded due to poor image quality. Smartphone teledermoscopy referrals allow for faster and more efficient management of patients with skin cancer as compared to traditional paper referrals. Key words: teledermatology; teledermoscopy; melanoma; non-melanoma skin cancer; triage; E-health.
Accepted Jun 5, 2014; Epub ahead of print Jun 10, 2014
Acta Derm Venereol
John Paoli, MD, Assoc Prof, Department of Dermatology and Venereology, Sahlgrenska University Hospital, SE-413 45 Gothenburg, Sweden. E-mail: john.paoli@vgregion.se
In Sweden, the incidence of malignant melanoma (MM) has increased with almost 6% annually over the past decade in both sexes. In addition, squamous cell carcinoma (SCC) is now the second most common cancer among Swedish men and women (1). Furthermore, the cumulative probability of developing basal cell carcinoma (BCC) before the age of 75 years is more than 15% (2). Meanwhile, the number of dermatologists in Sweden has remained unchanged during the past decade causing long waiting times for patients and greater responsibilities in diagnosing skin cancer for the general practitioners (GPs) (3).
Today’s clinical pathway for patients with skin lesions of concern is based on referrals written on paper and sent to a dermatologist by post. As an alternative, store-and-forward teledermatology (TD) has proven to be an effective way of triaging patients with skin lesions of concern with improved access to dermatologists and reduced costs (4–6). Teledermoscopy (TDS), which involves the addition of both clinical and dermoscopic images to the referral, can increase the diagnostic accuracy of TD by 15% (7). To simplify the TDS process, our group recently showed the feasibility of a novel mobile, cable-free and hand-held TDS system based on referrals sent through a smartphone application (“app”), with images obtained with the smartphone’s built-in camera and a digital dermoscope connected to the phone (8). The primary purpose of this study was to investigate whether such smartphone TDS referrals could provide faster management of patients with skin cancer and more accurate prioritisation of patients with skin lesions of concern compared to normal paper referrals without images.
MATERIAL AND METHODS
This study obtained ethics approval from the Ethical Review Board of the University of Gothenburg (approval number 853-11) and participants gave informed consent before taking part. It was carried out during a one-year period (January 11–December 21, 2012) at 20 primary healthcare centres (PHCs) in western Sweden and the departments of Dermatology at Sahlgrenska University Hospital (SUH), an urban hospital, and Skaraborg Hospital (SH), a rural hospital. PHCs that regularly referred patients with skin lesions of concern to SUH and SH were invited to participate in the study. The GPs at the recruited PHCs were asked to use smartphone TDS referrals for all eligible patients with TDS.
All patients over 18 years of age with one or more skin lesions of concern requiring referral to a dermatologist were eligible for inclusion in the study using the TDS referral system. The control group consisted of an equal number of consecutive patients referred to SUH and SH from other PHCs via the traditional paper-based referral system during the same period.
Patients were excluded if they did not fulfill the inclusion criteria, if they did not attend the face-to-face (FTF) visit(s), in cases of non-compliance or if their skin lesions were located on a body part that could not be photographed.
Each PHC was equipped with a registered version of the app iDoc24 PRO® (iDoc24® AB, Gothenburg, Sweden) pre-installed on a smartphone (iPhone® 4, Apple, Cupertino, California, USA) and a hand-held dermoscope compatible with the smartphone (FotoFinder Handyscope®, FotoFinder® Systems GmbH, Bad Birnbach, Germany). An Internet connection (WiFi, 3G or Edge) was used to send data. The participating GPs received a 30-min demonstration of the technology prior to commencing the study.
The app’s functionality has been described previously (8). In summary, the GP takes one clinical and one dermoscopic image (1,024 ×766 pixels each). Next, a standardised query form is filled out including all relevant clinical information. Upon sending the referral, the data is embedded within seconds on a secure web-based TDS platform (Tele-Dermis®, iDoc24® AB, Gothenburg, Sweden) with a Secure Socket Layer (SSL) encryption. The GP immediately receives a unique 8-digit identification code through the app when the case has been received by the Tele-Dermis® platform. Simultaneously, the participating dermatologists are sent an e-mail notification that a new referral is ready for assessment. The 8-digit identification code is used to retrieve all data at any time.
The dermatologists log on to the Tele-Dermis® platform with individual usernames and passwords to review the referrals on a 17- or 19-inch liquid crystal display monitor. The dermatologist chooses from standardised triage responses, which can be modified and personalised. The triage response includes an assessment of the nature of the lesion (benign, malignant or unclear), one or more possible diagnoses, the priority given (high, within 2 weeks; medium, within 4 weeks or low, within 8–12 weeks), suggested management (none, medical therapy, destructive therapy or surgery) and, finally, a dermoscopic description. Since the patient data was sent anonymously via the app in the study, the GP sent the patient’s national ID number, contact details and 8-digit identification code by fax to the corresponding Department of Dermatology in order for the patient to be called for a FTF visit.
All patients were called for a FTF visit at the corresponding department of Dermatology to evaluate the safety of the method and to study the frequency of incidental findings. All MMs and SCCs were confirmed histopathologically. Keratoacanthomas were classified as SCCs. During the FTF visit, dermatologists used dermoscopy to evaluate the study lesions and also carried out a full body skin examination (FBSE). Data was collected from the patients’ electronic medical records regarding: the final clinical or histopathological diagnosis of the referral lesion(s), the primary therapy applied, the number of visits needed, the waiting times from referral to diagnosis and/or treatment and any incidental findings.
In total, 122 GPs referred patients via the smartphone TDS system at the 20 participating PHCs. The TDS referrals were assessed by 2 specialists in dermatology at SUH (JP and EJB) and by a specialist (KT) and a 4th-year resident in dermatology (JDG) at SH. The paper referrals were all assessed by specialists in dermatology at SUH and SH.
In both groups, a suspicion of MM or SCC was triaged within 2 weeks; MM in situ or SCC in situ was prioritised within 4 weeks and all other diagnoses were offered a FTF visit within 8–12 weeks. It is important to mention that SH generally had much shorter waiting times than SUH during the study period. SH also had a slightly different protocol for triaging their control patients giving higher priority to patients with a suspicion of BCC or AK. After the triage process, all patients were managed according to standard protocols at the hospitals independently of the referral method.
All data were analysed using R version 2.14.2 (The R Foundation for Statistical Computing, Vienna, Austria). The ‘coin’ package was used for hypothesis tests and the ‘ggplot2’ and ‘survival’ packages were used for Figs 1 and 2, respectively. Fisher’s exact test was used to compare proportions between groups. Mantel–Haenszel’s test was used when comparing proportions between groups using stratification. Two-sample tests were performed using Wilcoxon’s rank sum test (using stratification when necessary). p-values smaller than 0.05 were considered statistically significant.
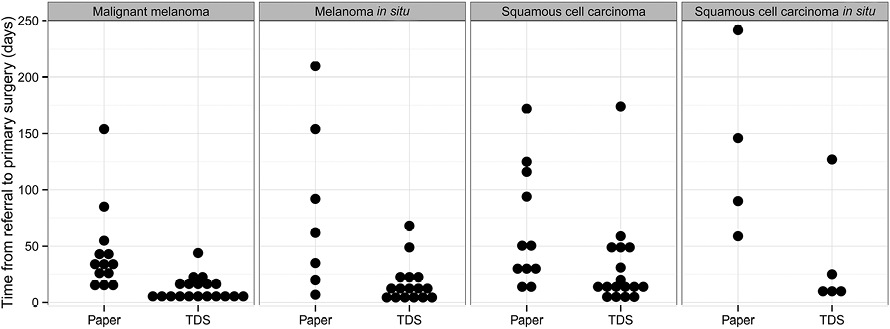
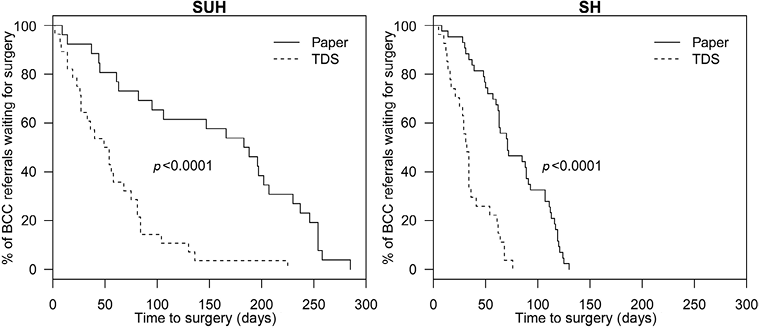
Fig. 2. Waiting times for patients with basal cell carcinomas (BCCs) requiring surgical treatment in the teledermoscopy (TDS) and paper referral groups at Sahlgrenska University Hospital (SUH) and Skaraborg Hospital (SH), respectively.
RESULTS
A total of 902 suspected cancer lesions were referred via TDS from 12 PHCs to SUH (n = 585) and from 8 PHCs to SH (n = 317). The control group consisted of 918 patients from other PHCs via traditional paper-based referrals to SUH (n = 577) and SH (n = 341). In total, 86 referrals were excluded from the TDS group (57 SUH and 29 SH referrals) and 172 referrals were excluded from the control group (143 SUH and 29 SH referrals). The reasons for exclusion are shown in Fig. S11. The final data analysis was therefore based on the 816 eligible TDS referrals from 772 patients (cases) and 746 patients referred with paper referrals (controls).
Among the 772 patients referred via TDS, 474 were female (61.4%). The mean age of all patients was 54 years (range 18–93 years). In the paper referral group (n = 746) there were 426 women (57.1%). The mean age of all control patients was 61 years (range 18–97 years).
The GP received a response from the dermatologist in a mean time of 233 min (3.9 h) and a median time of 109 min (1.8 h). The fastest response time was 2 min and the slowest response time was 46 h. Within 24 h, 798 referrals (98%) had been assessed. The paper referrals, on the other hand, arrived at the Departments of Dermatology after a mean time of 5 days (range 0–82 days) and a median delay of 4 days.
The final clinical or histopathological diagnosis of the lesions referred via TDS and the primary diagnosis of the patients referred via paper referral are presented in Table I. The melanocytic and non-melanocytic nature of the lesions in the TDS and control groups is presented in Table SI1. The final diagnosis was histopathologically confirmed in 292 TDS referrals (36%) and 259 paper referrals (35%).
Table I. Distribution of the final diagnoses in patients referred by smartphone teledermoscopy (TDS) and traditional paper referrals
|
Diagnosis |
TDS n (%) |
Paper n (%) |
|
Malignant |
229 (28.1) |
323 (43.3) |
|
Malignant melanoma |
19 (2.3) |
13 (1.7) |
|
Melanoma in situ |
16 (2.0) |
7 (0.9) |
|
Squamous cell carcinoma |
17 (2.1) |
11 (1.5) |
|
Squamous cell carcinoma in situ |
7 (0.9) |
11 (1.5) |
|
Basal cell carcinoma |
109 (13.4) |
115 (15.4) |
|
Actinic keratosis |
61 (7.5) |
164 (22.0) |
|
Other malignanta |
0 (0.0) |
2 (0.3) |
|
Benign |
587 (71.9) |
423 (56.7) |
|
Dysplastic naevus |
89 (10.9) |
46 (6.2) |
|
Benign naevus |
236 (28.9) |
126 (16.9) |
|
Seborrhoeic keratosis |
125 (15.3) |
97 (13.0) |
|
Other benignb |
137 (16.8) |
154 (20.6) |
|
Total |
816 (100) |
746 100) |
aMalignant lesions including leiomyosarcoma and mycosis fungoides; bBenign lesions including angioma, pyogenic granuloma, chondrodermatitis, dermatofibroma, lentigo solaris, papilloma, benign lichenoid keratosis, inflammatory skin diseases and other unspecified lesions.
TDS rendered 22.6% more referrals given low priority (Table SII1). This difference was mainly seen at SH, which used a different protocol for triaging their paper referrals as mentioned above. Due to this difference, no further analysis of the accuracy of the triage process was carried out for SH paper referrals.
In the TDS group, all of the 19 invasive MMs were prioritised correctly (high priority) and all 16 MM in situ were at least given medium priority as per protocol. In contrast, 3 out of 4 invasive MMs (75%) referred via paper referral to SUH were incorrectly given a medium or low priority and 3 out of 5 MM in situ (60%) were given low priority. In regards to the patients with SCCs, 11 of 17 (65%) were triaged for a visit within 2 weeks in the TDS group as compared to 2 of 5 (40%) in the control group at SUH. Similarly, 5 of 7 SCC in situ (71%) in the TDS group were correctly given high or medium priority in comparison with 4 of 9 SCC in situ (44%) in the control group at SUH.
Although this study was not designed to measure diagnostic accuracy, 346 (42%) of the 816 lesions of concern referred via TDS were assessed as being benign without any differential diagnoses. The final clinical or histopathological diagnoses of these lesions were also benign in 343 cases (99.1%). If the teledermoscopists had chosen to not call these patients for a FTF visit in a real-life situation, only 3 AK lesions (0.9%) would have been missed. In contrast, 196 (24%) of the 816 lesions of concern referred via TDS were deemed to be malignant without any differential diagnoses. In 146 of these cases (74%), the final clinical or histopathological diagnosis was also malignant (62% were confirmed histopathologically).
As shown in Table II, patients requiring surgery with a final clinical or histopathological diagnosis of MM, MM in situ, SCC, SCC in situ or BCC had a significantly shorter waiting time for a first visit with a dermatologist in the TDS group (p < 0.0001). In addition, the waiting times to receive surgical treatment (when required) were also significantly shorter in the TDS group for patients with MM (p < 0.0001), MM in situ (p = 0.028), SCC (p = 0.046), SCC in situ (p = 0.022) and BCC (p < 0.0001) as shown in Figs 1 and 2. The median waiting time for diagnosis and treatment for all patients with malignant lesions was 36 days for TDS referrals and 85 days for paper-based referrals (p < 0.0001). However, no statistically significant differences were observed in the median waiting times for diagnosis and treatment (when necessary) for patients with benign lesions between the TDS group (55 days) and the control group (46 days, p = 0.49).
Table II. Median number of days that patients with malignant lesions requiring surgical treatment had to wait for a first visit with a dermatologist and for the first excision in the smartphone teledermoscopy (TDS) and traditional paper referral groups
|
|
Group |
MM |
MM in situ |
SCC |
SCC in situ |
BCC |
|
Median time to first visit, days |
TDS |
9 |
10 |
13 |
13 |
28 |
|
Paper |
14 |
17 |
21 |
96 |
34 |
|
|
Median time to surgery, days |
TDS |
9 |
12 |
15 |
13 |
34 |
|
Paper |
35 |
62 |
48 |
118 |
89 |
MM: malignant melanoma; SCC: squamous cell carcinomas (including keratoacanthomas); BCC: basal cell carcinoma.
Patients in the TDS group were able to receive primary treatment on a single FTF visit with a dermatologist in 93.4% of the cases (95% CI, 91.5–95.0%) as compared to 82.2% of the paper referral cases (95% CI, 79.2–84.9%). Patients with MM, SCC, BCC and dysplastc naevi required significantly fewer visits in the TDS group to receive their diagnosis and primary management. Patients with AKs were generally managed during their first FTF visit in both groups (data not shown).
Sixteen of the 35 malignant melanocytic lesions in the TDS group (46%) were in situ as compared to 7 of 20 in the paper referral group (35%). The median Breslow thickness of the 19 invasive MMs in the TDS group was 1.0 as compared to 2.2 in the 13 invasive MMs of the control group. The malignant incidental findings are shown in Table SIII1.
DISCUSSION
We have shown that smartphone TDS referrals could be assessed within 24 h and provided faster management of patients with skin cancer. The median time to diagnosis and treatment for all skin cancer types was significantly reduced using TDS and more patients referred via TDS were able to receive surgical treatment (when required) on their first FTF visit. TDS also diminished the number of inaccurately triaged referrals in patients with potentially life-threatening cancers. Furthermore, fewer patients were triaged to an urgent visit unnecessarily. Finally, over 99% of the images sent via TDS were of sufficient quality to help the teledermoscopists with their triage decision.
This is the largest study to date on patients comparing the clinical outcomes resulting from triage through either TD/TDS or traditional letter referral systems in a real-life clinical scenario. Nevertheless, this study has some limitations. Although all participating PHCs were asked to refer all eligible patients with TDS, we could not make this mandatory. Thus, single GPs at the participating PHCs were able to send paper-based referrals instead of TDS referrals during the inclusion period. The lesion types referred via TDS and paper referrals differed somewhat. TDS referrals were more commonly used for patients with single lesions leading to an increased number of benign and dysplastic naevi. On the other hand, paper referrals were used more often for patients with multiple lesions such as AKs. This could perhaps be explained by the fact that patients were not randomised to TDS or paper referral. Also, the current version of the TDS app only allows the user to refer one lesion at a time. Adding more lesions to each TDS referral is technically possible, but would require better 3G coverage or WiFi at the PHCs. Furthermore, the physicians performing the FTF visits were not blinded to the results of the assessment of the teledermoscopists. Lastly, we could not influence the traditional triage protocol used by SH for their control patients in which most referrals (96.8%) were given high or medium priority. It was interesting, however, to see how dramatically the triage decisions at SH shifted towards lower prioritisation when their dermatologists assessed TDS referrals.
Smartphone TDS referrals reduced the waiting times for a first FTF visit with a dermatologist and for primary treatment in patients with MM, MM in situ, SCC, SCC in situ or BCC. Similarly, Lim et al. (9) showed that the mean waiting time for a first assessment by a dermatologist was reduced from 114 to 39 days using TDS. Morton et al. (5) also showed a decrease in the mean waiting time for patients with MM, SCC and BCC to definitive treatment, albeit not as dramatically.
Although skin cancer patients can potentially be triaged incorrectly using TD and TDS, this risk is lower with TDS than with paper referrals (4, 6, 8). Many of the lesions regarded as benign with no differential diagnoses could potentially lead to avoided FTF visits with a dermatologist freeing up capacity at the hospital. Using a TD system, Knol et al. (10) reported a 53% reduction in FTF visits with a dermatologist. Moreno-Ramirez et al. (4) filtered out 51% of the referred lesions using TD. Using a TDS referral system, Morton et al. (5) showed that 72% of the referred patients could be managed outside the hospital. Furthermore, Tan et al. (6) showed that TDS could spare 74% of the dermatologist’s FTF consultations.
We have shown that smartphone TDS referrals allow GPs and patients to receive a preliminary diagnosis, a treatment plan and an analysis of the dermoscopic images within 24 h in 98% of the cases. Moreno-Ramirez et al. (4) showed that referrals from GPs using store-and-forward TD with 2 clinical images could provide accurate and reliable triage for 2,009 patients with skin lesions of concern in a mean time of 61 h. Other internet-based TD(S) triage systems have also shown clinical effectiveness, reliability, and validity (6, 11). In this study, we have shown similar results using a smartphone-based TDS system, which is mobile, wireless and hand-held (8).
When patients are referred from a GP to a dermatologist for a skin lesion of concern, other malignant lesions are sometimes found after a FBSE (12, 13). Such incidental findings were found in 13–14% of the patients in our study regardless of the referral type. Aldridge et al. (12) found 14 incidental MMs when carrying out FBSEs in 1,851 patients (0.8%). Viola et al. (13) also reported incidental findings in 15% of 400 patients upon FBSE, including 6 MMs (1.5%). In our study, 12 MMs were found in 1,518 patients (0.8%), which supports these authors’ findings. A reminder about the importance of a FBSE can be added to the standardised responses sent back through the TDS platform.
It is known that image quality in TD and TDS can be a problem. Mahendran et al. (14) reported that 15% of TD referrals sent by GPs were not assessable due to insufficient image quality. Some studies have used a melanographer to try to solve this problem (5, 6). In our study, however, only 4 out of 902 TDS referrals (0.4%) had to be excluded due to poor image quality. All the other TDS referrals had images of sufficient quality to allow the dermatologist to suggest one or more preliminary diagnoses and supply a triage decision.
Although the number of patients diagnosed with MM or MM in situ in this study was limited, patients with such lesions had more favourable prognostic characteristics in the TDS group with a greater percentage of in situ lesions and thinner invasive MMs. The Breslow thickness of MMs can increase between 0.05 to 0.5 mm every month, depending on the type of tumour (15, 16). A recent study showed that MMs triaged via TD were on average 1.06 mm in thickness as compared to 1.64 mm in patients who received care after traditional paper referral (17).
In conclusion, smartphone TDS referrals allow for faster and more efficient management of patients with skin cancer as compared to traditional paper referrals, especially in a country like Sweden with long waiting times to see a dermatologist. Moreover, the method is safe and leads to fewer incorrectly triaged skin cancer patients. With the rising incidence of skin cancer, the lack of dermatologists and the number of unnecessary excisions carried out within primary care today in many European countries, smartphone TDS referrals can provide substantial improvements to the clinical pathway for patients with skin lesions of concern.
ACKNOWLEDGEMENTS
This study was financed with grants from The Swedish Association of Local Authorities and Regions, Skaraborg Hospital’s Research and Development Center and Skaraborg’s Research and Development Center. We would also like to thank all the GPs and health care professionals who participated in this study for their excellent collaboration.
Conflicts of interest: Alexander Börve is the founder and owner of iDoc24 AB. John Paoli is a small shareholder in iDoc24 AB. The other authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1906
REFERENCES


