


Seonguk Min1,2#, Seon Yong Park1,2#, Ji Young Yoon2, Hyuck Hoon Kwon1,2 and Dae Hun Suh1,2
1Department of Dermatology, Seoul National University College of Medicine, 2Acne and Rosacea Research Laboratory, Seoul National University Hospital, Seoul, South Korea
#These 2 authors contributed equally to this work.
Post-inflammatory erythema is a common result of acne inflammation and is cosmetically unacceptable without effective treatment. Fractional microneedling radiofrequency (FMR) has potential for treatment of post-inflammatory erythema. The aim of this study was to evaluate the efficacy and safety of this treatment. A retrospective chart review was undertaken of 25 patients treated with 2 sessions of radiofrequency at 4-week intervals and 27 patients treated with oral antibiotics and/or topical agents. Efficacy was assessed through an investigator’s global assessment of photographs, and the analysis of erythema with image analysis software and photometric devices. Histological changes resulting from the treatment were evaluated by skin biopsy. FMR treatment resulted in significant improvements in erythema with no severe adverse effects. Histological study revealed a reduction in vascular markers and inflammation. FMR is a safe and effective treatment for post-inflammatory erythema, with potential anti-inflammatory and anti-angiogenetic properties. Key words: acne; post-inflammatory erythema; fractional microneedling radiofrequency.
Accepted Jun 3, 2015; Epub ahead of print Jun 10, 2015
Acta Derm Venereol 2015; XX: XX–XX.
Dae Hun Suh, Department of Dermatology, Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul 110-744, South Korea. E-mail: daehun@snu.ac.kr
Acne affects approximately 80% of adolescents and young adults (1, 2). Severe acne inflammation can result in subsequent erythema or hyperpigmentation and even permanent acne scarring. There are many reports of various treatments for pigmentation or acne scarring. However, there are few reports concerning treatment for residual erythema induced by acne inflammation. Post-inflammatory erythema (PIE) is very common following inflammatory acne and is often cosmetically unacceptable to patients (3). Patients usually have persistent red marks after clearing of the acute inflammation following acne treatment. Facial PIE improves with time, but very slowly, and in some cases, complete clearance of PIE cannot be achieved (4).
Radiofrequency devices, associated with preservation of the epidermis, and with fewer complications or adverse effects and rapid recovery times, are becoming popular (5, 6). Fractional microneedling radiofrequency (FMR) delivers bipolar radiofrequency directly to the dermis using an array of microneedles (7). FMR has been reported to improve skin laxity and wrinkles (7–9). Bipolar radiofrequency has been reported to induce profound neoelastogenesis and neocollagenesis, which has been suggested as a potential mechanism of clinical efficacy (10). Moreover, FMR has been shown to have a therapeutic effect on inflammatory skin diseases, such as acne (11). We hypothesized that the dermal remodelling and anti-inflammatory effects of FMR may successfully treat PIE caused by persistent inflammation and destruction of the dermal matrix.
To date, no study has evaluated the efficacy of radiofrequency treatment in post-inflammatory erythema. The aim of this retrospective study was to evaluate the efficacy, safety and histological changes of FMR in post-inflammatory erythema. To the best of our knowledge, this is the first report of FMR for the treatment of PIE induced by acne inflammation.
MATERIALS AND METHODS
Study design and subjects
A retrospective chart review was undertaken of 52 patients who visited the Department of Dermatology, Seoul National University Hospital, South Korea, between August 2013 and February 2014. The study protocol was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Seoul National University Hospital (No.1407-136-597). Twenty-five subjects with PIE with few or no active acne lesions, who had been treated with FMR on the face, were included in the FMR-treated group. Twenty-seven patients with PIE and little or no active acne, who had been treated with oral and/or topical antibiotics, were included in the control group. Exclusion criteria were: patients with no photographs, hypertrophic or keloid scarring, patients being treated with any other treatment for acne scarring or erythema, including chemical or mechanical skin resurfacing, or use of topical or oral retinoids, for at least 3 months prior to first study. None of the patients underwent other acne scar treatments, including chemical or laser resurfacing during treatments.
Preparation and laser treatment
All treatment procedures were performed by a single surgeon (SM). Topical anaesthesia with EMLA® (AstraZeneca, Södertälje, Sweden) was administered 30 min before laser treatment commenced. The subjects in the FMR-treated group had received 2 sessions of FMR (INFINI®, Lutronic, Goyang, South Korea) treatment at 4-week intervals. The applicator tip comprised 49 insulated microneedles over an area of 1 cm2. The FMR system delivered the bipolar RF energy to the dermis at a frequency of 1 MHz, and at adjustable power levels ranging from 2.5 W to 50 W in 2.5 W increments. The exposure time, for which the RF energy was flowing per shot, could be adjusted from 10 ms to 1000 ms. In the current study, levels 2 (5 W) to 3 (7.5 W) were used, with exposure times of 50–70 ms. Three passes of treatment were done per each session. Ice packs were applied to reduce pain, followed by application of topical antibiotics, immediately after treatment. Subjects were allowed to use emollient and cosmetics from the next day onwards.
Clinical outcome assessment
On average, subjects in the FMR-treated group were followed up at 4-week intervals during the treatment period (2 treatment sessions) and 8 weeks after the final session of treatment. A standardized medical photograph was taken using identical camera settings (EOS 600D®; Canon, Tokyo, Japan) and lighting conditions. Assessment of the clinical photographs was conducted by 2 independent dermatologists (DHS and SYP). Efficacy was assessed by investigator’s global assessment (IGA), which comprised 5 points associated with degree of improvement (grade 0: no improvement, grade 1: 0–25% improvement, grade 2: 26–50% improvement, grade 3: 51–75% improvement, grade 4: 76–100% improvement). Objective evaluation of erythema was routinely done via 2 photometric devices (Spectrophotometer CM-2002®; Konica Minolta, Tokyo, Japan; Derma-spectrometer®; Cortex Technology, Hadsund, Denmark). At every visit, patients were asked to report any adverse effects. Subjects’ subjective assessment of therapeutic effectiveness was surveyed using a visual analogue scale (VAS) ranging from 0 (initial visit status of PIE) to 5 (complete clearance) for the FMR. Satisfaction was also measured by use of a VAS ranging from 0 to 10 (0: dissatisfied, 10: fully satisfied).
Computer-aided erythema evaluation
Many textural features for quantification of redness, including mean, standard deviation, smoothness, uniformity and entropy, were explored with a computer program, MATLAB® (The MathWorks, Inc., Natick, MA, USA) to distinguish colour differences in PIE from surrounding normal skin. In addition, many colour channel transformations, including grey channel, red channel, blue-red difference channel and a* from L*a*b*, were tested to assess the severity of erythema. Among them, smoothness using a* channel was used in this study to maximize the description of colour difference. “Smoothness” is a measure of the smoothness of intensity according to the following formula: R=1–1/(1+σ2), where R is 0 for a region of contrast intensity and approaches 1 for regions with large excursions in the values of its intensity levels. The medical photographs, taken at baseline and 8 weeks after the second session of treatment in the FMR-treated group, and at baseline and after a similar term in the control group, were analysed with this program and smoothness values were obtained.
Histopathology
Skin specimens were obtained by punch (2-mm) biopsy from the cheek in 6 available patients in each group 8 weeks after the last session of treatment. Written informed consent was obtained from all subjects prior to skin biopsy. Sections were stained with haematoxylin-eosin (H&E) and α smooth muscle actin (αSMA). Tissue was also processed for immunohistochemical (IHC) staining for NF-κB, interleukin-8 (IL-8), and vascular endothelial cell growth factor (VEGF) (Santacruz, Dallas, TX, USA). The intensity of IHC staining was assessed by use of an image analysis program (Leica QWin version 3.5.1, Leica Microsystems, Wetzlar, Germany).
Statistical analysis
Student’s t-test was used to compare the differences between data obtained before and after FMR treatment (SPSS, version 12.0; SPSS Inc., Chicago, IL, USA). Statistical significance was accepted at p-values < 0.05.
RESULTS
Twenty-five patients (12 men, 13 women) in the FMR-treated group and 27 patients (19 men, 8 women) in the control group were included in the study (p = 0.100). The participants all had Fitzpatrick skin types III–IV. The mean age of the subjects was 21.4 and 20.0 years in FMR-treated group and control group, respectively, with no significant difference. The mean baseline erythema indices were 19.6 and 19.3, and mean baseline a* scale 9.9 and 9.7, respectively, with no significant differences between the 2 groups. The number of FMR treatment sessions was 2. There were no serious adverse effects that resulted in stopping treatment.
Erythema improvement
The grade of PIE improved in all patients (25/25) in the FMR-treated group and in 5 patients (5/27) in the control group. Inter-rater agreement was evaluated with κ statistics (κ value = 0.73, p < 0.001), demonstrating congruence between the 2 raters. There was a significant difference between the FMR-treated group and the control group in IGA score (p < 0.001). The mean IGA score for the FMR-treated group was 2.72, which indicates an improvement of approximately 45%. By contrast, the IGA score for the control group was 0.32 (a 7.5% improvement).
Photometric measurements of erythema revealed consistently decreased redness after FMR treatment compared with the baseline or control group (Fig. 1). There were significant reductions in the erythema index (p = 0.002) and a* scale (p < 0.001) in the FMR-treated group compared with the control group.
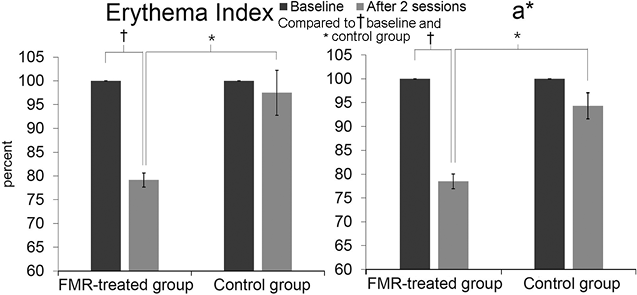
Fig. 1. Photometric measurements of the fractional microneedling radiofrequency (FMR)-treated group and control group. Decreased (A) erythema index and (B) a* scale in the FMR-treated group after 2 sessions of treatment (*, † p < 0.05).
Clinical photographs illustrating the improvement in redness in the FMR-treated group and the lack of improvement in the control group are shown in Fig. 2.

There were no severe adverse effects of FMR, other than mild adverse effects, such as pain during the procedure and erythema lasting for 3–5 days. No subjects dropped out due to erythema.
Erythema analysis by software
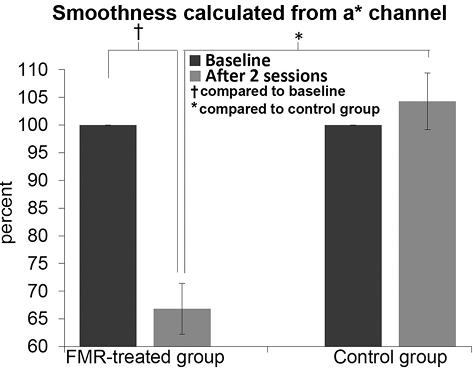
Smoothness from the a* channel was calculated with the MATLAB® program. There were no statistical differences in smoothness between the 2 groups at baseline (0.000219 vs. 0.000214) or between baseline and final evaluation in the control group (0.000214 vs. 0.000211). However, the FMR-treated group had a lower smoothness value from a* channel than the control group at final evaluation (0.000138 vs. 0.000211; p = 0.008), and a significant decrease in smoothness from a* channel was seen in the treated group compared with baseline (0.000138 vs. 0.000219; p < 0.001). The mean ratio of smoothness between final evaluation and baseline was significantly less in the FMR-treated (66.8%) than in the control group (104.3%) (p < 0.001) (Fig. 3).
Patient’s subjective assessment
The satisfaction score and the therapeutic effectiveness for the FMR treatment were 7.8 ± 0.3 and 3.6 ± 0.3, respectively. All subjects scored greater than 5 for satisfaction. Out of 25 subjects, 18 (71.4%) scored greater than 4 for effectiveness.
Histological findings
H&E staining revealed reduced inflammation, and αSMA staining showed decreased microvessels after 2 sessions of treatment with FMR (Fig. S11). Reductions in IL-8, NF-κB and VEGF staining intensity were also observed 8 weeks after the second session of treatment. Image analysis showed significant differences in the mean area percentages for controls and FMR-treated patients, respectively; 20.3% and 9.7% for IL-8 (p = 0.049), 15.7% and 7.5% for NF-κB (p = 0.032), and 24.8% and 9.4% for VEGF (p = 0.008), (Fig. 4).
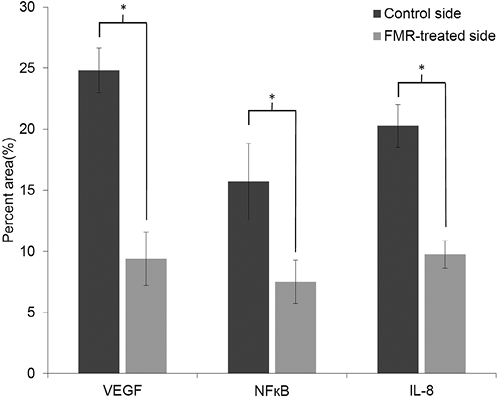
Fig. 4. Image analysis of immunohistochemistry staining of specimen from fractional microneedling radiofrequency (FMR)-treated group and control group. Significantly decreased intensity of vascular endothelial cell growth factor (VEGF) was observed after FMR treatment (compared with control group, p = 0.008). Significant down-regulation of NF-κB (compared with control group, p = 0.032) and interleukin (IL)-8 (compared with control group, p = 0.049), which is associated with inflammatory reaction, was shown after FMR treatment (*p < 0.05).
DISCUSSION
There is no established treatment for acne-related PIE. FMR treatment was first introduced to improve skin aging; however, there have been several reports that it can improve acne inflammation (11, 12). Therefore, we conducted the present retrospective study to determine whether FMR can improve PIE associated with inflammation.
To date there have been few studies of PIE treatment. Pulsed-dye laser and non-ablative 1550-nm fractional laser has been shown to improve PIE (4, 12, 13). The present study demonstrated dramatic improvements in PIE according to the investigators’ and patient’s subjective assessments and evaluation using photometric devices and image analysis. The adverse effects of FMR were minimal. Facial PIE contributes to the emotional, social and psychological disability induced by acne (14). FMR could be an effective and safe treatment method of resolving this stressful skin condition.
Erythema has been evaluated in some previous studies via clinical photographs with computer-aided image analysis. Zhao et al. (15) analysed changes in erythema index after photodynamic therapy for port-wine stains using ImageJ (free software). The current study developed a novel variable smoothness for PIE evaluation by assessing the colour differences between the lesional area and normal area of skin, and it showed similar degrees of improvement, as measured by photometric devices. Smoothness calculated from a* channel could be used to evaluate macular erythema in other dermatoses, but its usefulness has not yet been evaluated objectively.
Previous studies on PIE treatment with other lasers have shown clinical improvement, but have not clearly demonstrated the mechanism of the effect. Bae-Harboe & Graber (3) used pulsed-dye laser to treat PIE and suggested that its effectiveness is attributable to targeting haemoglobin and small-diameter vascular processes. Park et al. (4) proposed that 1550-nm fractional laser treatment targets tissue water and causes photothermal destruction of dermal vasculature, resulting in improvement in erythema. A suggested mechanism for FMR is remodelling of the dermal structure and decreased sebaceous gland activity due to the thermal effect of radiofrequency (16, 17). In the present study, decreased intensity of NF-κB, IL-8, and VEGF was observed under IHC staining. We hypothesize that inflammation may contribute to neovasculogenesis, resulting in residual erythema after resolution of active acne lesions. Therefore, FMR could improve PIE by modulating inflammatory and vascular components.
NF-κB plays a key role in regulating the immune reaction, and controls many genes involved in inflammation. NF-κB is chronically active in many inflammatory diseases (18). NF-κB can activate IL-8 and VEGF expression via binding to NF-κB sites of the promoter of these genes (19). NF-κB inhibitors lower the levels of VEGF production, and overexpression of NF-κB inhibitor (IκBa) results in decreased VEGF levels (20, 21). IL-8 can also up-regulate VEGF expression via various molecular pathways (20). In tumour formation, the tumourigenic process can be enhanced by inflammatory cytokines, by up-regulating angiogenesis mediators, such as IL-8 and VEGF (21). Moreover, the vascular changes associated with angiogenesis could occur not only in cancer but also in other diseases, including cardiovascular disease, rheumatoid arthritis, hypersensitivity and asthma (21).
Although the mechanism by which FMR regulates NF-κB or IL-8 is unknown, we suggest that FMR treatment may reduce inflammation of the PIE lesion, and this is supported by decreased expression of NF-κB, resulting in down-regulation of VEGF via a direct or indirect (via lowering IL-8) pathway.
This study was done by retrospective review. Thus, we tried to avoid information bias of study results. First, clinical assessment was done by independent two dermatologists. We also evaluated the inter-rater agreement by Cohen’s kappa test. Second, objective measurements using photometric devices were done. Third, clinical photographs were analyzed by digital image processing program (MATLAB®). However, there is still more risk of selection bias compared with prospective study.
In conclusion, PIE is an under-studied sequelae of acne, and its clinical significance can be overlooked compared with active acne or depressive acne scarring. This study demonstrates that FMR is a safe and effective method for PIE treatment; its effectiveness is proven by several objective and subjective assessments. FMR treatment could improve erythema by reducing inflammation and abnormal vessel proliferation. Anti-inflammatory and anti-angiogenetic effects of FMR may have therapeutic effects in skin diseases other than PIE. Further research may reveal other indications for FMR treatment and other options for treatment of PIE.
Acknowlegement
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (No. 2014R1A2A1A11049397).
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2164
REFERENCES


