


1Melanoma Unit, Dermatology Department, Hospital Clínic & IDIBAPS (Institut d’Investigacions Biomèdiques August Pi i Sunyer), 2Centro Investigación Biomédica en Red de Enfermedades Raras (CIBERER), Instituto de Salud Carlos III (ISCIII), 3Departament de Medicina, Universitat de Barcelona, Barcelona, 4La Roche-Posay Laboratoire Dermatologique, Madrid, Spain, and 5La Roche-Posay Laboratoire Dermatologique, Asnières, France
#These authors contributed equally to this work.
Patients with photodermatoses or actinic keratosis benefit from very high ultraviolet B-ultraviolet A (UVB-UVA) photoprotection. However, poor compliance is an issue that jeopardizes adequate protection, leading to disease recurrence. This study evaluated the efficacy of a daily protective moisturizer with high UVB and UVA photoprotection applied 8 h before irradiation. A monocentric, open-label, prospective, control pilot study was performed including 10 patients. Patients were irradiated with UVB and UVA before and 8 h after topical application of the product. Reflectance confocal microscopy (RCM) assessment was performed 24 h later. Clinical assessment showed a statistically significant increase in minimal erythema dose (MED) after application of the product (p < 0.001). Signs of UV damage according to RCM were not observed on photoprotected skin (p < 0.05). Skin irradiated 8 h after applying a daily protective moisturizer presented an increase in MED and RCM findings that equal the findings for non-irradiated skin.
Key words: photosensitivity disorders; polymorphic light eruption; topical; sunscreen agent; confocal microscopy.
Accepted Jun 28, 2017; Epub ahead of print Jun 29, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Susana Puig, Melanoma Unit, Dermatology Department, Hospital Clinic Barcelona, Villarroel 170, ES-08036, Barcelona. Spain. E-mail: susipuig@gmail.com; spuig@clinic.ub.es
Human exposure to ultraviolet (UV) radiation from sunlight can have many adverse effects. Ultraviolet B (UVB) radiation (290–320 nm) is mainly responsible for the most severe damage: acute sunburn and long-term damage, including skin cancer. It has a direct effect on cell DNA and proteins (1). Unlike UVB, UVA radiation (320–400 nm) is not directly absorbed by biological targets (2), but can dramatically impair cell and tissue functions. UVA penetrates deeper into the skin than UVB. It particularly affects connective tissue, where it produces detrimental reactive oxygen species (ROS), also known as free radicals. As with UVB, UVA has been implicated in depression of the immune system (3, 4) and in the development of skin cancer, principally melanoma and squamous cell carcinoma (5, 6). Photosensitivity reactions, as well as photodermatoses, are mainly induced by UVA (7).
Polymorphic light eruption (PLE) is the most common photosensitivity disease: approximately 15–20% of Europeans appear to have the condition (8, 9) as do 10–15% of those living in the northern USA (10), although only 5% of Australians (11) have the disease.
PLE is characterized clinically by the occurrence within hours to days of ultraviolet radiation (UVR) exposure of non-scarring, pruritic, erythematous papules, papulovesicles, vesicles or plaques on sun-exposed skin areas, generally symmetrically, which then resolve completely over several days to a week. It is commonly most severe in the spring or early summer, often diminishing in severity as summer progresses, before disappearing completely during the winter. The minimal erythema dose (MED) is usually normal.
The mild disease in many patients is usually controlled by moderation of sun exposure at times of high UV intensity, use of protective clothing, and regular application of broad-spectrum sunscreens with high sun protection, particularly against UVA.
The effects of acute and chronic exposure to UV have been studied mainly by histology and immunostaining. However, novel non-invasive imaging techniques, such as RCM and optical coherence tomography (OCT), have recently been used to evaluate UV-exposed skin sites (12, 13). These techniques have the advantages of allowing the detection of morphological changes in the skin in vivo without removing the tissue and of allowing the possibility of repeated investigations of the same skin at different times. As melanin provides strong contrast on RCM, resulting in bright reflectance on RCM images, this technique has been used to evaluate pigmentation after repeated radiation with UVA and UVB in several studies (14, 15). In this regard, an increase in epidermal thickness, and a decrease in dermal reflectivity and vasodilatation have been shown in a recent comparative study of OCT and RCM after application of 1 and 3 MED of solar-simulated radiation (14).
Acute and chronic effects of UVA exposure have also been shown by RCM, including epidermal hyperplasia and increased pigmentation. Furthermore, a recent study (16) compared superficial burn caused by UV and heat, showing an increase in stratum corneum thickness in sunburned sites, and a decrease in this layer was observed after thermal injury. Recently, Ulrich et al. (17) and Koller et al. (18) reported that RCM allowed the detection of morphological changes induced by UV, including spongiosis, sunburn cells, microvesicles and blood vessel dilatation. The appearance of sunburn cells and microvesicles was dependent on the dose of UVB and on the individual susceptibility of the study participants. It is possible to perform repeated skin assessments over different periods of time, hence allowing an architectural and cytological assessment. Furthermore, RCM provides a more detailed visualization of inflammatory cells and epidermal blood flow than does histological examination (19).
Since UV protection is one of the key preventive and prophylactic measures available for patients with PLE, a condition that can greatly affect the quality of life of patients, guaranteeing commitment to treatment is fundamental. Good compliance can be affected by uncomfortable posology and/or unpleasant cosmeticity of a product, amongst other factors.
A daily protective moisturizer that contains high-broad UVB and UVA protection has been shown to have remnants of UV protection in vivo after 8 h of application. Such a characteristic could be very useful for patients who could benefit from daily high-broad UV protection, such as those with photosensitivity disorders.
The objective of the present study was to determine the efficacy of a single application of a product with high broad UVB and UVA protection, applied 8 h before UV irradiation, in decreasing UV photodamage markers, as evaluated clinically and by RCM in patients with PLE.
Ten patients with PLE were included in the study (7 females and 3 males): 1 patient with skin phototype I, 1 with skin phototype II, and 8 with skin phototype III. The mean age of the patients was 36.7 years and median age was 39 years (range 17–60 years).
Exclusion criteria were: age <16 years; pregnancy; history of being exposed to other forms of radiation (other than sunlight); current use of known photosensitizing drugs.
For patients between 16 years and 17 years and 11 months, signed consent was obtained from the patient’s parents.
This study was approved by the local Institutional Review Board and all clinical investigation was conducted according to the principles of the Declaration of Helsinki and was performed following Good Clinical Practice standards. Patients were given an Informed Consent Document concerning their agreement to participate in the study.
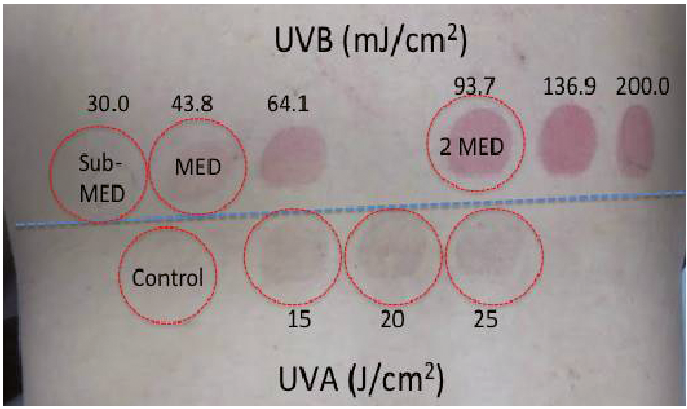
Patients were instructed not to change any of their photoprotection practices during the duration of the study. Patients were irradiated on the back with 6 increasing doses of UVB for detection of MED (20.5, 30.0, 43.8, 64.1, 93.7, 136.9 mJ/cm2 for phototype I patients and 30.0, 43.8, 64.1, 93.7, 136.9, 200.0 mJ/cm2 for phototype II–III patients, in agreement with the Spanish Group of Photobiology protocol for phototests (20)) and 3 fixed doses of UVA (15, 20, 25 J/cm2) through a UV-opaque fenestrated adhesive patch. Appropriate UV-opaque shields were used to protect surrounding untreated areas. RCM assessment was performed 24 h later on non-irradiated skin, on 1 MED, 2 MED and subMED sites (UVB), and on all UVA-irradiated sites (Fig. 1). Not more than 2 weeks later, the same procedure was repeated after topical application of 2 mg/cm2 of the study product on the lower back 8 h before irradiation. UVA irradiation was performed with a specific device (UVA700 L; Herbert Waldmann GmbH & Co., Villingen-Schwenningen, Germany), containing UVA lamps with main emission ranging from 330 to 450 nm and maximum emission at 390–410 nm. UVB irradiation was performed with a specific device (UV 801 BL; Herbert Waldmann GmbH & Co.), containing UVB lamps with main emission ranging from 280 to 350 nm and maximum emission at 306 nm. Correct dosage irradiation was controlled by a dosimeter for UVA and UVB connected to the fenestrated adhesive patch (Variocontrol; Herbert Waldmann GmbH & Co.).
Fig. 1. Example of study areas from one of the patients. Patient’s measurements were reassessed 24 h after irradiation without application of the product. 1 minimal erythema dose (MED) was defined, as well as areas considered subMED and 2 MED. A random unexposed area was considered control.
Assessment of clinical signs of acute photodamage (erythema, vesicles, pigmentation) and MED was performed 24 h after each irradiation session, i.e. pre- and post-application of the product.
A commercially available RCM system was used in this study for in vivo assessment of the skin (Vivascope 1500; Mavig GmbH, Munich, Lucid-Tech Inc., Henrietta, NY, USA).
At each site subjected to RCM assessment images were taken from 4 randomly selected spots. At each spot 50 images of 500 × 500 µm were saved, starting immediately above the stratum corneum, with each new image obtained 3 µm deeper until approximately 150 μm. This is termed a “vivastack”. A total of approximately 26,000 500 × 500 μm bitmap (.BMP) images were taken and stored.
Changes seen through RCM assessment in inflammatory skin conditions have been described by Ardigo et al. (19). Ulrich et al. (17) and Koller et al. (18) have described RCM findings after UVB irradiation, correlating them with histological findings. Based on these previous publications, some of the criteria described as relevant in assessing these conditions were considered and selected for evaluation in the current study. RCM images were evaluated by 3 independent dermatologists and classified according to the criteria described in Table SI.
In order to confirm the clinical diagnosis of PLE and to correlate the RCM findings with the histological findings obtained by conventional light microscopy, a 3-mm punch biopsy sample was obtained from each patient at the assessment performed 24 h after UV irradiation on the non-protected skin site at a 2 MED dose, following RCM assessment. The specimen was fixed in formalin and embedded in paraffin for routine haematoxylin and eosin evaluation.
The product used in this study is a commercially available daily protective moisturizer with high UVB and UVA photoprotection (Anthelios KA; La Roche-Posay Laboratoire Dermatologique, Asnières, France), which has a SPF of 100 and a UVA-protection factor (UVA-PF, PPD [persistent pigment darkening]) of 40. Also, it has been tested in vivo for SPF after 8 h of application, with a maintained SPF of 62. The product contains the following UV filters: organic: ethylhexyl salicylate (Octisalate), bis-Ethylhexyloxyphenol methoxyphenol triazine (bemotrizinol; Tinosorb®S), butyl methoxydibenzoylmethane (Avobenzone), Ethylhexyl triazone (Uvinul®T150), octocrylene, drometrizole trisiloxane (silatriazole; Mexoryl®XL), terephthalylidene dicamphor sulphonic acid (ecamsule; Mexoryl®SX); inorganic: titanium dioxide (nano and regular). The product was applied at a dosage of 2 mg/cm2 using its high-precision-dispensing pump system (1.05 g/pump).
The mean MED after UVB irradiation at follow-up visit 1 was 56.46 mJ/cm2 (Table I). Only one patient from the PLE group had detectable MED at post-product irradiation assessment (24 h after UVA and UVB skin irradiation with the product applied to the back 8 h prior to irradiation), with a 2-fold MED increase compared with the unprotected MED at follow-up visit 1. All other patients had undetectable MED at the highest irradiation dosage of the test (> 136.9 mJ/cm2 for phototype I and > 200.0 mJ/cm2 for phototypes II and III patients). The increase in MED after the use of the product was statistically significant (p < 0.0001).
Table I. Ultraviolet B minimal erythema dose (MED) values before and after application of the product
No patients presented erythema after UVA irradiation on either assessment (pre- or post-product application). No patients presented systemic adverse events during the study.
The comparison of the scored RCM images from non-irradiated skin and irradiated unprotected skin at different doses (subMED, MED and 2MED) did not show statistically significant changes at the suberythematous level (SubMED). There are significant differences at the higher-dose unprotected exposed sites, as expected (1 MED and 2 MED; p < 0.0001).
On erythematous dose, at the 1 MED level all assessed criteria showed statistically significant differences except for parakeratosis and presence of microvesicles. The presence of microvesicles and parakeratosis, however, are both significant at 2 MED (p = 0.01 and p = 0.002, respectively).
Regarding UVA irradiation, there were no differences seen at all fixed doses (15, 20 and 25 J/cm2) when comparing non-irradiated with irradiated non-protected skin.
After assessment and scoring of the RCM images obtained from irradiated skin without product and with product, at sub-erythematous levels (subMED) there is a statistically significant difference in the presence of small bright epidermal cells between groups (p = 0.007). At 1 MED
the only criterion without a statistically significant difference was the presence of parakeratosis. This difference is, however, significant at 2 MED (p = 0.001). There were statistically significant differences for all the other criteria at 1 MED and 2 MED comparing non-protected with protected skin.
Regarding UVA irradiation when comparing non-protected with protected skin, there were no differences seen at 15 J/cm2 and at 20 J/cm2. At 25 J/cm2 one criterion showed statistically significant differences when comparing non-protected with protected skin: small bright epidermic cells (p = 0.02). Complete data can be seen in Table SII.
Assessment of RCM images showed an improvement in signs of UV damage at the cellular level, where signs found after unprotected UV irradiation, such as spongiosis, microvesicles, sunburn cells and blood vessel dilatation, were not observed on photoprotected skin at all irradiated doses (p < 0.05) (Figs 2 and 3). Fig. 4 shows the correlation between some histological findings of acute UV damage in the epidermis and its representation in RCM.
Fig. 2. Reflectance confocal microscopy images from the same patient as shown in Fig. 1 at different doses of UVB (stratum spinosum images). Left to right: unexposed and skin irradiated with UVB without product; at 1MED, areas of spongiosis are seen (red dashed circles); at 2 MED, microvesicles can be detected (yellow dashed circle) as well as sunburn cells (blue arrows).
Fig. 3. Same patient from figure above, stratum spinosum images, UVB irradiated skin with product applied 8 hours prior to irradiation and unexposed skin: no signs of spongiosis, microvesicles, sunburn cells or other signs of photodamage on UVB irradiated sites. Similar findings were noticed in unexposed skin and skin irradiated with product.
Fig. 4. Correlation between findings with reflectance confocal microscopy (left column) and histological structures seen with optical light microscopy (right column). In the upper panel, yellow arrows indicate sunburn cells (apoptotic keratinocytes). In the lower panel, blue dashed circle highlights a microvesicle.
Sun exposure has been coupled with numerous types of acute and chronic reactions in the skin, for example, sunburn, photoimmune suppression, photodermatoses, photoaging, and skin cancer. When scrutinizing our growing understanding of the potentially unfavourable long-term side-effects of solar irradiation, there is a universal call for harmless and effective photoprotective agents. Several studies have demonstrated the immuno-suppressive effects of UVB, and of UVA (21), and the induction of DNA damage by UVA in addition to UVB (22).These studies clearly demonstrate the role of UVA in the induction of photoimmunosuppression and DNA damage induction, together with the need for sunscreen products providing efficient photoprotection throughout the entire UV spectrum.
Histological changes in the skin associated with UVR exposure include apoptotic keratinocytes (sunburn cells), vacuolated Langerhans cells, intracellular oedema (spongiosis) and hypogranulation/degranulation of mast cells within 24 h after exposure (23, 24). At the clinical level, the initial skin response is erythema, due to dilation of superficial skin vessels. The pigment response that follows the erythema is stimulated by UVR-induced DNA damage and/or repair of keratinocytes (25, 26) or through changes in melanin distribution from the basal layer to the suprabasal layer (27). The observations reported from histological studies of spongiosis, sunburn cells and microvesicles following exposure to UVR have been confirmed in non-invasive studies using RCM (15, 17, 28). Although skin changes following exposure to UVR are well documented with RCM, little is known about the modification of these changes with different UV doses and photoprotection. The current study evaluated these UV-induced changes by RCM in patients with the most common of the idiopathic photodermatoses, PLE, and tested the efficacy of a moisturizing cream with photoprotection after 8 h of application in terms of reduction in these UV-induced changes.
The mean MED of UVB was 56.46 mJ/cm2, inside the normal range described by phototype in our population (20). It has already been reported that patients with PLE have normal sun sensitivity in terms of MED of UVB, although 10–20% of patients can have lower UVB MED. In those patients with lower MEDs, the higher UVB irradiation doses can photo-induce the PLE lesions.
Irradiation with a UVA source did not induce any abnormal response. This is consistent with results reported by other authors (29), who set the cut-off for an abnormal response at a level of irradiance of less than 20 J/cm2. We were not able to see any changes in RCM when comparing non-irradiated with irradiated non-protected skin at different doses; however, at 25 J/cm2 UVA we found differences between protected and non-protected skin. The unprotected skin showed more small bright epidermal cells than protected skin at 25 J/cm2 UVA irradiation (p = 0.02). This is an example of how RCM is able to detect cellular changes induced by UVR that are not clinically visible; in this case as pigmentation.
The current testing of sunscreen efficacy focuses only on MED determination and does not allow the identification of structural or cellular changes in UV-irradiated skin. In this study, we applied RCM for the in vivo evaluation of acute changes after UV radiation and correlated these with protected skin 8 h after application of high photoprotection. We aimed to identify morphological changes of sunburn reaction over a time course of 24 h.
Although there are some studies that demonstrate morphological and biophysical changes in skin barrier lipids with chronic suberythemal dose exposure (30), our results indicated that no RCM changes at suberythemal acute doses are produced compared with non-irradiated skin. We were able to identify changes at MED and 2 MED that were consistent with acute effects of UVR and that, in most cases, were not visible clinically (e.g. the presence of parakeratosis, spongiosis and microvesicles) (Table SII).
This is the first study to assess the efficacy of a single application of a product containing high broad-spectrum UV filters 8 h before UV irradiation. As a main result we found that only one patient had a detectable MED after skin irradiation with the product applied 8 h previously, although that MED increased 2-fold compared with without the product. All other patients had undetectable MED at the highest irradiation doses (>136.9 mJ/cm2 for skin type I and > 200 mJ/cm2 for skin types II and III), indicating the efficacy of the product even 8 h after application. Taking into account the difficulty of achieving the correct photoprotection, even in those patients with photodermatoses (31), the fact that the product remains active against UV effects after 8 h, enables a more comfortable posology and a better result.
With UVA irradiation we found differences only at the highest dose (25 J/cm2), with the presence of small bright epidermal cells in the non-protected area. The fact that we did not find any differences at the other doses could be explained because the normal population does not present any UVA clinical response below 20 J/cm2, and our study shows that, at these doses, no cellular or structural damage is produced in our patients.
It is notable that, with RCM, we found differences even in suberythematous levels of UVB, with the presence of small bright epidermal cells in the non-protected area. At 1 MED and 2 MED levels we found differences in all the criteria (except for parakeratosis at 1MED), signifying that the product is able to prevent all the structural and cellular effects produced by acute UV irradiation (Table SIII).
In this study RCM was able to visualize morphological changes of acute UVR, including sunburn cells, microvesicles, spongiosis, blood vessel dilatation and inflammation.
The skin sites treated with the tested sunscreens did not show any signs of cellular or structural damage. Microvesicle formation could be visualized by RCM without becoming clinically apparent, representing a sign of severe UV damage, which may be useful for an improved classification of sunburn reaction. This microvesicle formation can be seen clinically in those patients with PLE with a diminished MED, in which microvesicles can be seen in the highest dose as a photo-provoked PLE lesion. Furthermore, the detection of sunburn cells may be another marker for the grading of UV-damage by RCM. In this regard RCM might allow detection of UV-induced damage on a cellular and structural level and may be used for further characterization and grading of UV damage. In the future RCM may be used for testing sunscreens with a higher sensitivity for cellular and structural changes occurring after UVR.
We are indebted to the photodermatology nurses of Hospital Clinic de Barcelona and to all the patients who voluntarily participated in the study.
Funding/support: The main funding for the study was provided by La Roche Posay. The research at the Melanoma Unit in Barcelona was partially funded by Spanish Fondo de Investigaciones Sanitarias grants PI12/00840, PI15/00716 and PI15/00956; CIBER de Enfermedades Raras of the Instituto de Salud Carlos III, Spain, co-financed by European Development Regional Fund “A way to achieve Europe” ERDF; AGAUR 2014_SGR_603 of the Catalan Government, Spain; European Commission under the 6th Framework Programme, Contract No. LSHC-CT-2006-018702 (GenoMEL) and by the European Commission under the 7th Framework Programme, Diagnoptics; A grant from “Fundació La Marató de TV3, 201331-30”, Catalonia, Spain; a grant from Telemaraton of Spain “Todos somos raros” and a grant from “Asociación Española Contra el Cáncer (AECC)”. The work was carried out at the Esther Koplowitz Center, Barcelona.
The sponsors had no role in the design and conduct of the study; or in the collection, analysis and interpretation of data.
Conflicts of interest: Leonor Prieto, Sophie Seite and Dominique Moyal are employed by La Roche-Posay Dermatological Laboratories, the sponsor of the study. The authors report no other conflicts of interest in this work.


 Click to show fullsize
Click to show fullsize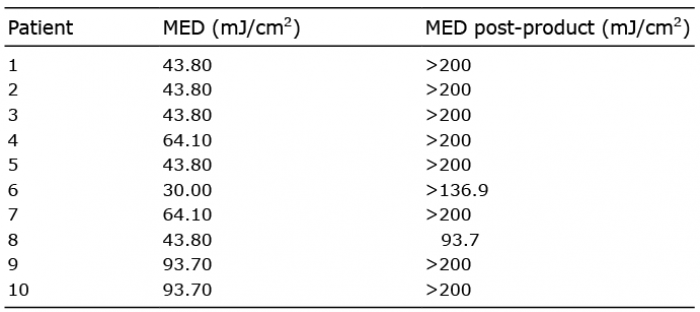 Click to show fullsize
Click to show fullsize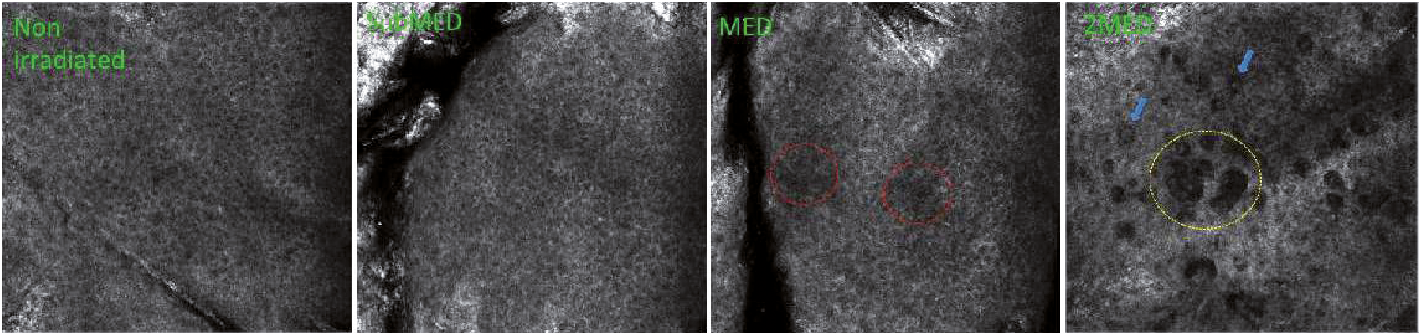 Click to show fullsize
Click to show fullsize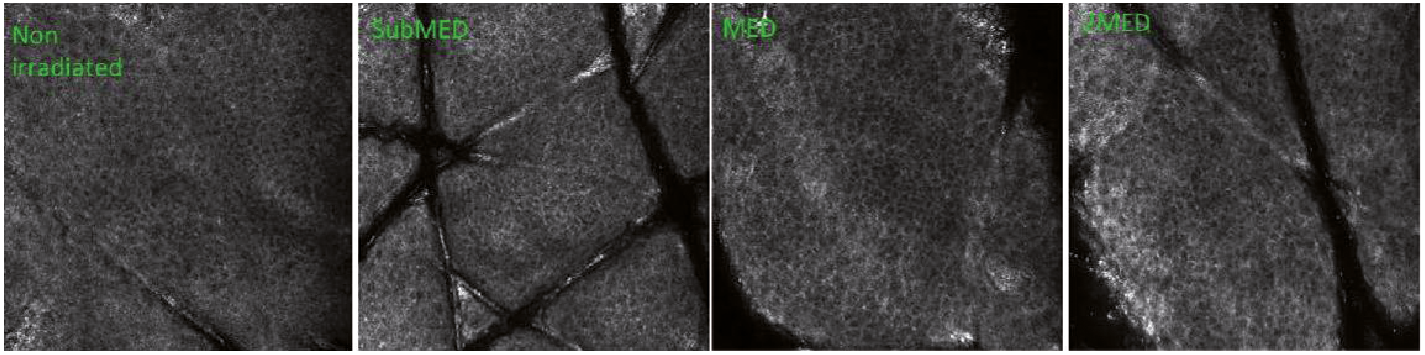 Click to show fullsize
Click to show fullsize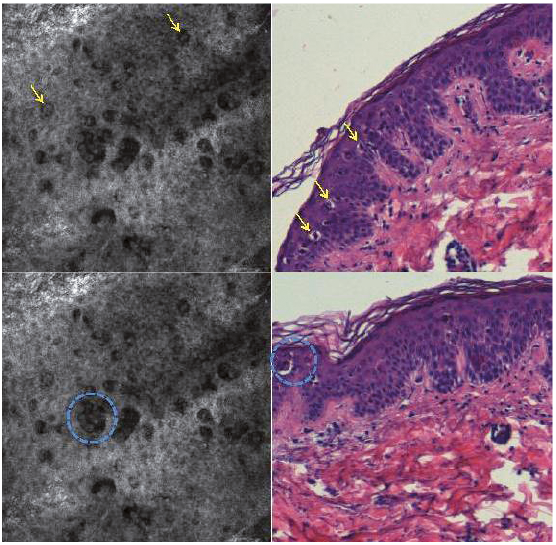 Click to show fullsize
Click to show fullsize