


1Division of Dermatology, UO Multizonale ’Santa Chiara’ Hospital, Trento, 2Skin Cancer Unit IRCCS IRST, Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori, Meldola (FC), 3Anatomic Pathology Unit, University Hospital of Parma, 4Section of Dermatology, Department of Medicine and Surgery, Parma Medical School, via Gramsci 14, IT-43100 Parma, Italy, Italy. E-mail: calogero.pagliarello@libero.it
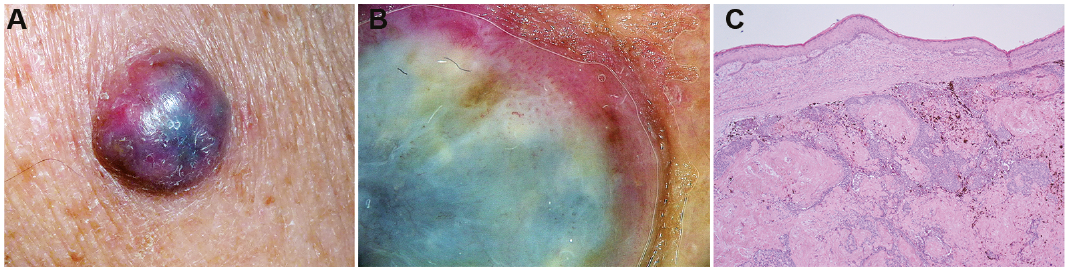
An otherwise healthy man in his 60s was concerned about an asymptomatic nodule on his left arm that showed rapid growth (Fig. 1A). The patient stated that it had been growing for approximately 2 months, and he was certain of the absence of any prior lesion at that site. Clinical examination revealed a 1-cm, firm, exophytic nodule, with colour ranging from pink to blue, with well-defined and regular borders, indolent and homogeneously hard on palpation, seated on photo-damaged skin. No ulceration or peripheral macular pigmentation was observed to extend beyond the base of the lesion. Dermoscopy revealed homogeneous blue pigmentation, patchy brown, scattered pigmentation and hairpin-like vessels at the borders, sometimes extending into whitish structureless areas (Fig. 1B). An excisional biopsy specimen was obtained (Fig.1C and D).
Fig. 1. (A) Clinical image. (B) Dermoscopy of the lesion. (C) Histopathological picture, haematoxylin-eosin. Original magnification ×4.
What is your diagnosis? See next page for answer.
Acta Derm Venereol 2017; 97: xx–xx.
Diagnosis: Melanocytic matricoma
Histologically, a well-circumscribed and asymmetrically pigmented dermal nodule composed of variably pigmented basaloid matrical cells forming clusters of “shadow” or “ghost cells” admixed with numerous melanized dendritic melanocytes was present in the underlying dermis (Fig. 2); this last component of the neoplasm was identical to a recently described entity, melanocytic matricoma (1). No local recurrence was noted at the site of the original biopsy after a 2-year follow-up.
Fig. 2. Close-up view of Fig. 1C; ×20.
Melanocytic matricoma represents a benign, pigmented papule occurring on sun-damaged skin of elderly men. It is formed by a nodular proliferation of neoplastic matrical and supramatrical cells admixed with an apparently normal, abundant population of melanin-laden dendritic melanocytes. Although some authors suggest that melanocytic matricoma is a variant of pilomatricoma (2, 3), these entities are considered to be clinically different. Moreover, an agminated variant has been reported in a young Japanese patient (4) presenting with sessile 5-cm nodules surrounded by indurations.
A review of the literature revealed a small number of reports (26 papers retrieved from PubMed using the following search strategy: melanocytic [All Fields] AND matricoma [All Fields], mainly from the dermatopathology literature, with only 3 clinical pictures, all published, from very uncharacteristic cases: one from a woman’s cheek (5), one from the above-cited young Japanese patient (4), in which the lesions presented as agminated, and one of malignant melanocytic matricoma, presenting as a crusted, exophytic, pigmented papule on the helical rim (6). No clinical pictures of the usual presentation or dermatoscopic pictures of this entity have been published to date.
Indeed, our main clinical concern was to rule out nodular melanoma; dermoscopy suggested both the diagnosis of dermal melanoma metastasis or primitive dermal melanoma, ruling out nodular melanoma for the lack of certain key features (atypical vascular pattern, milky-red areas, ulceration, or black pigmentation). If a rare tumour had been hypothesized, then pigmented epithelioid melanocytoma might have represented the better choice, not considering the patient’s age (7). It is notable that, due to the lesion’s rapid growth, excision was the treatment of choice, since cases of malignant melanocytic matricoma have been reported (6, 8–10). Finally, since pathologists themselves, to understand whether melanocytic matricoma represents a bona fide entity or is simply a variant of matricoma, advocate for a better description of clinical features of these tumours. Inasmuch as this seems lacking at present, dermatologists should be aware of this rare entity.


 Click to show fullsize
Click to show fullsize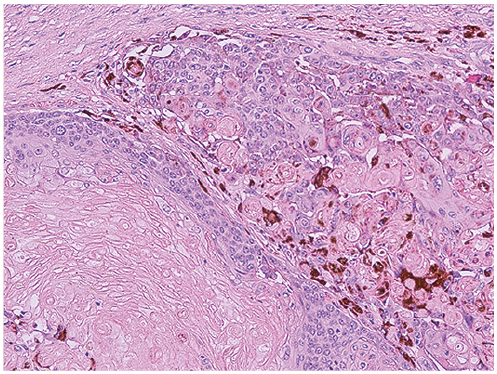 Click to show fullsize
Click to show fullsize