


1Department of Infectious Diseases, Public Health Service Amsterdam, Nieuwe Achtergracht 100, NL-1018 WT Amsterdam, 2Amsterdam Infection and Immunity Institute (AI&II), Academic Medical Center, University of Amsterdam, 3Department of Blood-borne Infections, Sanquin Blood Supply, Amsterdam, 4Public Health Service Flevoland, Lelystad, 5Department of Medical Microbiology, OLGV General Hospital, 6Laboratory of Experimental Virology, Department of Medical Microbiology, and 7Department of Dermatology, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands. E-mail: h.j.devries@amc.uva.nl
Accepted Aug 9, 2017; Epub ahead of print Aug 10, 2017
Hepatitis C virus (HCV) has emerged as a sexually transmitted infection (STI) in human immunodeficiency virus (HIV)-positive men who have sex with men (MSM), whereas HIV-negative MSM remain largely unaffected. This case report describes 2 HIV-negative MSM in a long-term relationship who sequentially acquired a highly similar HCV strain based on NS5B sequencing (340 nt). Screening of high-risk MSM for HCV, irrespective of HIV status, should be considered.
After the introduction of combination antiretroviral therapy (cART) in 1996, hepatitis C virus (HCV) has rapidly emerged as a STI among (HIV)-positive MSM (1). Although HIV is no prerequisite for sexual transmission of HCV, HIV-negative MSM have remained largely unaffected (2). In recent years, however, the number of case reports of sexually acquired HCV among HIV-negative MSM is increasing steadily (2–5). We previously described 4 HIV-negative MSM who were infected with HCV strains that specifically circulated among HIV-positive MSM (2). All 4 HIV-negative MSM reported HIV-positive sexual partners, which suggested incidental sexual transmission of HCV from HIV-positive MSM to HIV-negative MSM. The current case report describes 2 HIV-negative MSM in a long-term relationship, who sequentially acquired HCV strains with nearly identical NS5B gene fragments. Both strains are part of a cluster of equally similar HCV strains that have been circulating among HIV-positive MSM. This case report underlines once again that HCV sexual transmission occurs in HIV-negative MSM and emphasizes the potential threat of HCV spreading to, and within, the HIV-negative population.
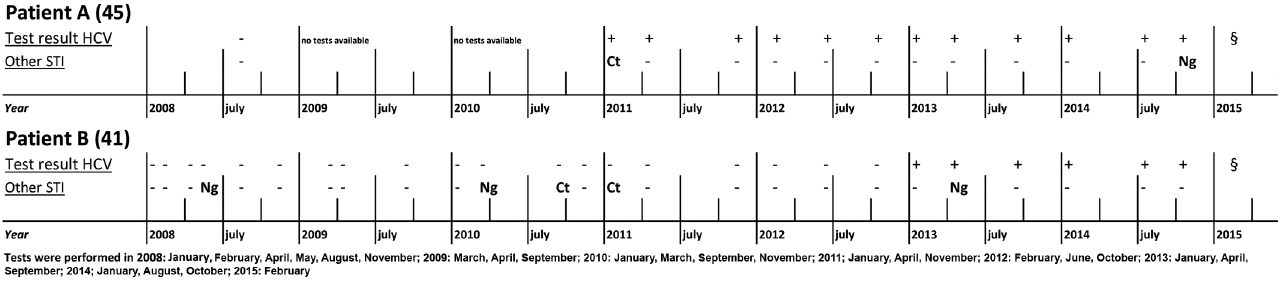
In February 2015, 2 HIV-negative men in a long-term open relationship, tested positive for HCV antibodies after being warned about an HCV infection by a third partner with symptoms of acute HCV with whom both had had sexual contact. The presence of HCV infection was confirmed by HCV RNA testing. Patient A (45 years) and B (41 years) both reported serosorting, by jointly engaging in sex parties for presumed HIV-negative men only. Both men had receptive and insertive anal sex with approximately 20 partners in the last 6 months. They reported practicing negotiated safety (i.e. they always used condoms with third partners, but not when having sex with each other). Both men participated in group sex, and reported performing anal fisting but never without using nitrile gloves. Sex toys were shared but always cleaned with anti-bacterial soap before changing partners. Both men reported recreational oral and intranasal drugs during sex, e.g. gammahydroxybutrate (GHB), ketamine and cocaine, but they had never injected drugs. Despite their attempts to reduce the risk of STI, both men had been diagnosed with multiple STIs at the Amsterdam STI clinic; patient A with anorectal chlamydia (2011) and anorectal gonorrhoea (2014), patient B with gonorrhoea (2008, 2010 and 2013) and urogenital chlamydia (2010) (Fig. 1). At the time of HCV diagnosis they had no other STIs. Both men were seronegative for HIV and syphilis 3 months after their HCV diagnosis. Contact tracing was initiated to detect additional HCV cases among the sexual partners of patients A and B. Of the 20 sexual partners during the 6 months prior to HCV diagnosis, 11 were reached. All tested HCV-negative. Unfortunately the person who initially warned the couple could not be reached, and another sexual partner who was allegedly HIV-negative and HCV-positive refused testing.
Fig. 1. Timeline of 2 human immunodeficiency virus (HIV)-negative men who have sex with men (MSM) who seroconverted for hepatitis C virus (HCV) antibodies. Tests were performed respectedly since 2008. Ng: Neisseria gonorrhoea; Ct: Chlamydia trachomatis; –: negative sexual transmitted infection (STI) test. §Warned by a third partner with symptoms of acute HCV.
To determine the time of HCV seroconversion, we retrospectively tested stored serum samples from previous STI clinic visits. Patient A seroconverted between October 2008 and January 2011, and patient B between October 2012 and January 2013 (Fig. 1). Both men were infected with HCV genotype 1a. A 436-bp fragment of the NS5B gene was amplified, sequenced and compared with 73 HCV strains obtained from HIV-positive MSM diagnosed with HCV-1a during the period 2000 to 2010 (1, 6). A phylogenetic tree was constructed using the maximum-likelihood approach using a general time-reversed substitution model with γ distribution assuming a certain fraction of evolutionary invariable sites (GTR+G+I) (Fig. S1). Both patients A and B were part of a large MSM-specific HCV cluster (MSM-1) along with 34 HIV-positive MSM.
Interestingly, both patients A and B were Δ32 CCR5 heterozygous and therefore less susceptible for HIV.
We previously described 4 HIV-negative MSM infected with HCV, of whom 2 also had an innate immunological variation that provided relative protection against HIV infection, either via a Δ32 CCR5 mutation or via reduced susceptibility of peripheral T cells to HIV (2). Despite repeated high-risk behaviour with known HIV-positive partners, these 4 men did not become infected with HIV. Patients A and B, however, claimed to only have sex with (allegedly) HIV-negative men. They further limited their risk of HIV infection and other STIs through negotiated safety.
Although HCV infections are relatively rare in non-injecting HIV-negative MSM, some recent disquieting reports indicate an increased HCV rate among HIV-negative MSM using, or interested in using, Pre-Exposure Prophylaxis (PrEP). In an ongoing biannual cross-sectional survey among attendees of the Amsterdam STI outpatient clinic, HCV prevalence among HIV-negative MSM remained stable and low (0.6%) from 2007 until November 2010 (6). Swedish data showed a similarly low (0.5%) HCV prevalence among HIV-negative MSM in Stockholm in 2013 (7). In contrast, 18/375 (4.8%) of HIV-negative MSM participating in the Amsterdam PrEP (AMPrEP) study tested HCV-positive at baseline in the period August 2015 to June 2016 (8). In IPERGAY 10 participants acquired HCV, while on PrEP, and 5 PROUD participants, which corresponds to an HCV incidence of 1.06 and 1.19 per 100 person years, respectively (9–11)2. HCV infection rates were not as high in all PrEP projects (3). Given the availability of PrEP, cART and highly effective direct antiviral agents (DAAs) for HCV, an increase in sexual high-risk behaviour caused by optimism among HIV-negative MSM is feared. Bridging between the HIV-positive and HIV-negative population might result in an expanding HCV epidemic irrespective of HIV status. This case report is in agreement with previous reports showing that HCV infection rates in HIV-negative MSM might be increasing, and emphasizes that HCV might also increase among high-risk HIV-negative MSM, outside the context of HIV co-infection.
This case report has the following weaknesses. Confirmed sexual transmission of HCV from patient A to patient B, hence from one HIV-negative MSM to the other, would invigorate the risk of HCV spreading within the HIV-negative population. However, NS5B sequencing, as performed in this study, cannot be used to confirm direct HCV transmission between patients. Short stretches of the relatively conserved NS5B gene have a low phylogenetic signal, which is reflected in the low genetic distances within our MSM-specific HCV clusters. Patients A and B frequently engaged in sex with others, and although they tried to limit their risk of HIV infection by practicing serosorting and negotiated safety, both men acquired various STI, including HCV. Although patients A and B have highly similar NS5B sequences, we cannot exclude that patient B acquired his HCV-infection through a joint (HIV-positive) third, or perhaps even fourth, casual partner. The HCV MSM-1 strain is highly prevalent among HIV/HCV co-infected MSM, and the HCV infection in patient A preceded that in patient B by almost 2 years. Sequencing of a more variable HCV genomic region (e.g. the hypervariable region, HVR) could bolster the claim of direct transmission, but will remain insufficient to distinguish this from transmission via joint sexual partners. Secondly, we assume that HCV transmission has occurred through unprotected anal intercourse. Yet, we cannot entirely exclude HCV transmission between patients A and B via sharing household equipment, such as toothbrushes, etc.
Although HCV infections in HIV-negative MSM have been described earlier, most international guidelines still do not advise who should be screened for HCV. This case report is illustrative of a population of high-risk HIV-negative MSM in which HCV infections are overlooked. Recent reports of HCV infections in MSM seeking PrEP further stress the need for guidelines for HCV testing in HIV-negative MSM. In conclusion, the number of case reports of sexually acquired HCV among HIV-negative MSM is gradually increasing and HCV screening of high-risk HIV-negative MSM may be needed. Awaiting more differentiated advice, the Dutch national testing policy for STI clinics advises testing MSM with newly diagnosed HIV and LGV and those seeking PrEP (12, 13); however, this is already proving to be a challenge due to financial issues.


 Click to show fullsize
Click to show fullsize