

Elizabeth Lee1, Tejesh Patel1, Gillian Hale2, Sherif Zaki3 and Kristopher Fisher1*
1Department of Dermatology, University of Tennessee Health Science Center, 930 Madison Ave suite 840, Memphis, TN 38163, 2Division of High-Consequence Pathogens & Pathology, and 3Infectious Disease Pathology Branch, Centers for Disease Control and Prevention, Atlanta, USA. *E-mail: kfisher5@uthsc.edu
A 38-year-old man presented with a 3-day history of painful erythematous papules clustered on the dorsal hands, with few papules on the palmar surface of the fingers (Fig. 1). No oral/peri-oral involvement was noted, and only a solitary incipient vesicle was identified. Skin manifestations were preceded by two days of fever and sore throat. Sick contacts include the patient’s 4-year-old child, who had a similar, more widespread eruption two weeks prior.
What is your diagnosis? See next page for answer.
Fig. 1. Erythematous papules, clustered in arcuate configuration on the 4th proximal interphalangeal joint, with scattered erythematous macules and papules on the 5th digit and dorsal hand.
Acta Derm Venereol
Diagnosis: Atypical Hand, Foot and Mouth Disease
Hand, Foot, and Mouth Disease (HFMD) classically affects young children during the summer and fall, and is transmitted via fecal-oral route. The most common causative viruses are coxsackievirus A16 or enterovirus 71, and after a 3–6 day incubation period, the infection generally follows a mild or asymptomatic course (1). Adults are rarely infected by these strains; however, since 2008 worldwide and 2011 in the USA, adult cases of the atypical variant of HFMD caused by coxsackievirus A6 have been described. These infections predominately result from familial transmission via a previously infected child, and have more widespread skin involvement with an increased severity of disease course than the typical counterpart (2–4).
Coxsackie A6 infection causing Atypical HFMD in adults has a variable mucocutaneous presentation, unlike typical HFMD, which characteristically presents with erythematous vesicular lesions of the palms and soles (1). Atypical HFMD can present with papules, rather than vesicles, can also appear purpuric, even targetoid, often involving the perioral mouth and groin. Because of inconsistent presentation and lesional morphologic variability, coxsackievirus A6 HFMD may be confused with Rocky Mountain Spotted Fever, eczema herpeticum, vasculitis, and secondary syphilis, bullous impetigo, and erythema multiforme (5–7). The variability of presentation and distribution of the exanthem in adults, with or without enanthem, makes accurate and swift diagnosis necessary in order to avoid unnecessary testing and potentially harmful intervention. Treatment of atypical HFMD is supportive with follow-up to ensure complete resolution and to screen for complications (1).
RT-PCR of vesicular fluid is the diagnostic test of choice for CVA6, as commercial serologic assays against this strain are not available (8). Although PCR can detect enteroviruses with a sensitivity of approximately 90% (3), it does not allow the serotype identification. Coxsackievirus A6 nucleotide sequencing can be performed on PCR positive specimens to confirm the diagnosis, if desired (2, 3).
Nearly all reported cases of coxsackieA6 infection, regardless of clinical heterogeneity, have described similar histologic findings (2, 6, 7). Specifically, these findings include necrotic keratinocytes scattered and clustered
throughout the epidermis (including the upper levels), papillary dermal edema and a superficial lymphocytic infiltrate (Fig. 2).
Fig. 2. a) Superficial peri-vascular dermatitis with mild papillary dermal edema, vacuolar changes along the junction, necrotic keratinocytes and scale-crust. H&E, × 40X. b) Necrotic keratinocytes scattered within the epidermis, clustered and concentrated in the upper levels, with lymphocyte extension into the epidermis. H&E, × 200.


 Click to show fullsize
Click to show fullsize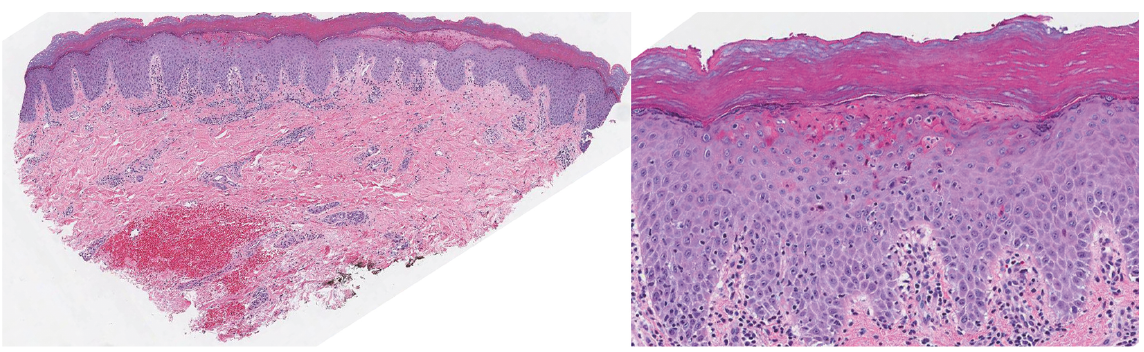 Click to show fullsize
Click to show fullsize