


Departments of Dermatology, 1Radboud University Medical Centre, Nijmegen, 2Erasmus Medical Centre, Rotterdam, 3Amsterdam Medical Centre, Amsterdam, 4Amphia Ziekenhuis, Breda, 5Zuyderland Medical Centre Heerlen, Heerlen, 6University Medical Centre Groningen, Groningen, 7Ziekenhuisgroep Twente, Hengelo, 8Máxima Medical Centre, Eindhoven, 9Ziekenhuisgroep Twente, Almelo, 10University Medical Centre Utrecht, Utrecht, 11Antonius Ziekenhuis, Sneek, 12St Anna Ziekenhuis, Geldrop, 13Zuyderland Medical Centre Sittard-Geleen, Geleen, 14Radboud University Medical Centre, Radboud Institute for Health Sciences, and 15Radboud University, Nijmegen, The Netherlands
#Shared first authorship. These authors contributed equally to this paper. °Shared second authorship. These authors contributed equally to this paper.
Interleukin 17-antagonist secukinumab demonstrated high efficacy for treatment of psoriasis in randomized controlled trials. However, performance in daily practice may differ from trials. Drug survival is a comprehensive outcome covering effectiveness and safety, suitable for analyses of daily practice. The aim of this study was to evaluate drug survival of secukinumab in a daily practice psoriasis cohort. Data were collected from 13 hospitals. Drug survival was analysed using Kaplan–Meier survival curves, split for reason of discontinuation. In total, 196 patients were included (83% biologic experienced). Overall, 12 and 18 months drug survival of secukinumab was 76% and 67%, respectively, and was mostly determined by ineffectiveness. There was a trend towards shorter drug survival in women and in biologic experienced patients. Thirteen percent of patients experienced at least one episode of fungal infection. This is one of the first studies of drug survival of secukinumab in patients with psoriasis treated in daily practice.
Secukinumab is the first interleukin-17 inhibitor registered for treatment of plaque psoriasis. This study describes drug survival, defined as the time a patient remains on a specific agent, for patients with psoriasis treated with secukinumab in daily practice. Our cohort comprised 196 patients: 96 from academic and 100 from non-academic hospitals. The majority of patients had been treated with other biologics prior to commencing secukinumab therapy (biologic experienced). Drug survival of secukinumab was 76% after 12 and 67% after 18 months, and was mostly determined by ineffectiveness. Drug survival rates were higher for biologic-naive patients compared to biologic experienced patients.
Key words: psoriasis; secukinumab; biologics; drug survival; effectiveness.
Accepted Feb 5, 2018; Epub ahead of print Feb 6, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Juul M. P. A. van den Reek and Lieke J. van Vugt, Department of Dermatology, Radboud University Medical Centre, PO Box 9101, NL-6500 HB Nijmegen, The Netherlands. E-mail: Juul.vandenReek@Radboudumc.nl, Lieke.vanVugt@Radboudumc.nl
Secukinumab, a monoclonal antibody targeting interleukin (IL)17A, has been registered for treatment of moderate-to-severe plaque psoriasis since 2015 (1, 2). The approved regimen for psoriasis is 300 mg subcutaneous every week for 4 weeks and once every 4 weeks thereafter. Phase III trials reported high response rates for this regimen, with 76–91% of patients reaching Psoriasis Area and Severity Index (PASI)75 and 54–73% reaching PASI90 after 12 weeks of therapy (3–6). Based on the biological function of IL17A, fungal infections were anticipated as a possible side-effect of secukinumab treatment. In the FIXTURE trial, Candida infections occurred in 5% of patients treated according to the label regimen, but all Candida events resolved spontaneously or with standard treatment, and none led to discontinuation of the study drug (3). It is important to realize, however, that trial results reflect efficacy and safety in a highly controlled setting, in a patient population shaped by stringent inclusion and exclusion criteria. Therefore, results from daily practice may differ from trial results and are important in evaluating an agents’ effectiveness and safety profile (7).
Data on the performance of secukinumab in daily practice is scarce. Drug survival, defined as the time a patient remains on a specific agent, is a comprehensive outcome covering effectiveness, safety and patients’ and doctors’ preferences (8). It is a suitable parameter for chronic diseases requiring long-term treatment, reflecting therapeutic success in a real-life setting (8–10). Subanalyses can be performed to gain insight into different reasons of drug discontinuation. Moreover, variables associated with long or short drug survival may be identified.
Our objective was to evaluate the drug survival of secukinumab in a multicentre psoriasis cohort, comprising the first patients treated with secukinumab in daily practice.
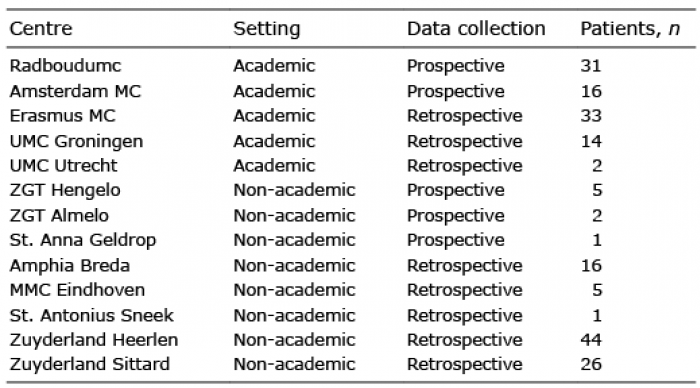
A multicentre daily practice cohort study was performed, focusing on drug survival of secukinumab in patients with psoriasis. Data from 2 prospective psoriasis registries (BioCAPTURE and the local database of the Academic Medical Centre (AMC), Amsterdam) were combined with retrospective data from other centres in the Netherlands. In total, 196 patients from 5 academic and 8 non-academic centres were included (Table I). Written informed consent was obtained for patients included in the BioCAPTURE and AMC registry. The medical ethics committee declared that written informed consent was not needed for the retrospective, anonymized collection of regular care data from other hospitals.
Table I. Participating centres
All patients had a clinical diagnosis of plaque psoriasis and were treated with secukinumab in a daily practice setting between May 2015 and May 2017. Inclusion took place during the entire study period, meaning that follow-up durations vary between patients, from several months to the entire study period. Patients who had previously received secukinumab in a clinical trial were excluded. Patients who were treated with secukinumab primarily for psoriatic arthritis by the rheumatologist were also excluded. If patients were treated with secukinumab multiple times, only the first treatment episode was used for the analyses.
Patients were treated according to the psoriasis label with 300 mg secukinumab at week 0, 1, 2, 3 and 4 and once every 4 weeks there-after. Deviations from this schedule were analysed and described. Patients using combination treatments with other anti-psoriatic agents (systemic or topical) were also included in the analyses. In general, physicians follow the Dutch guidelines, in which it is advised to monitor patients every 3 months for PASI, Dermatology Life Quality Index (DLQI) and laboratory investigations (11).
Anonymized data on patient characteristics, secukinumab start and stop dates, reasons for treatment discontinuation, treatment regimens, concomitant medication and adverse events were collected from all participating centres, according to a predesigned data collection form. Prospective data were retrieved from the registry databases and retrospective data were collected from patient files.
The following adverse events were collected: any adverse events classified by the physician as important or severe, any infection classified as severe, all fungal infections, and cardiovascular events. Incidence rates were calculated as first occurrence of an adverse event per patient, divided by the sum of follow-up years for this cohort. Normally, only time until the first occurrence of an adverse event is taken into account. However, as the exact time until occurrence of an adverse event was often not available, total follow-up time was used, leading to a slight underestimation of incidence rates. As a sensitivity analysis, cumulative number of events was divided by the sum of follow-up years for this cohort, for events that occurred more than once per patient (e.g. fungal infections).
Drug survival was analysed descriptively using Kaplan–Meier survival curves. Survival curves were generated for discontinuation; (i) in general; (ii) due to ineffectiveness; and (iii) due to side-effects. Patients were censored at the moment of their last visit, when lost to follow-up, or when secukinumab was discontinued for reasons other than inefficacy or side-effects for > 90 days. When patients stopped due to a combination of ineffectiveness and side-effects, they were counted as having had an event in all 3 analyses. Subanalyses were performed split for prior biologic use, method of data collection and sex. Secukinumab drug survival was not directly compared with other biologics, but for contextual purposes, drug survival of other biologics (source: BioCAPTURE) is presented as a supplement (Fig. S1). Also a sub-analysis in which a 60-day threshold as a maximum gap to determine discontinuation was performed. Log-rank tests were performed if possible (no crossing of survival curves). The following baseline variables were assessed as possible predictors for drug survival in univariate Cox regression analysis: age, sex, age at onset of psoriasis, prior biologic use, baseline PASI, body mass index (BMI), weight, diagnosis of psoriatic arthritis, baseline C-reactive protein (CRP) and treatment setting (academic vs. non-academic). Data were analysed using IBM SPSS Statistics, version 22.0.
A total of 196 patients was included: 96 (49%) from academic and 100 (51%) from non-academic hospitals. The mean and median follow-up duration of patients was 10.8 and 10.5 months, respectively. The total follow-up amounted to 176 patient years. Follow-up was ended when patients discontinued secukinumab, when the end of the study’s follow-up period (18 months) was reached or when patients were lost to follow-up. The mean age at start of secukinumab was 48.9 years (SD 13.6) and 119 patients were male (61%). Median baseline PASI was 10.9 (range 1.8–45.4). Median BMI was 28.7 kg/m2. Diabetes mellitus and hypertension affected 39 (20%) and 37 (19%) patients, respectively. Forty-six patients (23%) had a diagnosis of psoriatic arthritis and 33 patients (17%) were naive to biologics.
Most patients (79%) received secukinumab according to the psoriasis label. The most common deviation (12%) entailed dose tapering of secukinumab, either by prolonging the interval or by reducing the dose from 300 to 150 mg per 4 weeks. Other deviations were: use of 150 mg in the first weeks or months of treatment because patients mistakenly used 1 instead of 2 injections a time (4%), use of increased drug dosage by shortening the interval to 300 mg per 3 weeks (2%), and other deviations (2%). Concomitant systemic antipsoriatic drugs were used in 11% of patients. Methotrexate was the most common concomitant drug, used in 9% of patients. Methotrexate was given continuously (6 patients), as bridging therapy (4 patients) or started up later during secukinumab therapy (10 patients). Detailed patient and treatment characteristics are shown in Table II. In general, physicians follow the Dutch guidelines, in which it is advised to monitor patients every 3 months for PASI, DLQI and laboratory investigations (11). The exact frequency of visits was adequately registered in the leading research hospital (Radboudumc). The mean ± standard deviation interval between visits was 84 ± 40.4 days. This number is based on the last visit before secukinumab start, and all subsequent on-drug visits (122 visits in total).
Table II. Patient and treatment characteristics of patients with secukinumab (n = 196)
In total, 49 patients (25%) discontinued secukinumab. Ineffectiveness was the most frequent reason for discontinuation of secukinumab (30 patients). Other reasons for treatment discontinuation were: side-effects (8 patients), a combination of ineffectiveness and side-effects (8 patients), and other/unknown (3 patients). Amongst patients who discontinued due to ineffectiveness (either alone or in combination with side-effects), 13 showed primary non-response (no response to secukinumab within the first 3 months) and 25 experienced loss of effect at a later stage. Side-effects leading to treatment discontinuation were heterogeneous, but fungal infections were the most frequently reported reason (Table III).
Table III. Adverse events in psoriasis patients with secukinumab
Adverse events that developed during treatment are reported in Table III. Twenty-five of 196 patients (13%) experienced at least one episode of fungal infection, and 13 patients (7%) experienced at least one oropharyngeal fungal infection. The incidence rate (IR; first event per 100 patient years) was 14.2 (95% CI 9.4–20.6) for fungal infections in general, and 7.4 (95% CI 4.1–12.3) for oropharyngeal fungal infections. IRs based on cumulative number of events (in case events occurred more than once per patient) are shown in Table III.
The 12 and 18 months overall drug survival of secukinumab was 76% and 67%, respectively (Fig. 1a). The 12 and 18 months drug survival related to ineffectiveness was 80% and 72% (Fig. 1b); the 12 and 18 months drug survival related to side-effects was 91% and 90% (Fig. 1c). Median survival time could not be determined, because the Kaplan–Meier survival curve remains above 50% for the whole observation period. Mean drug survival time was 15.0 months (95% CI 14.2–15.8). Mean drug survival may lack clinical relevance, however, as it is dependent on the follow-up duration.
Fig. 1. Drug survival of secukinumab, split for reason of discontinuation. (a–c) “n” at risk was 196 at baseline, 146 at 6 months, 83 at 12 months, and 33 at 18 months.
Fig. 2 shows drug survival rates for separate groups based on treatment history. Fig. 2a shows biologic naive vs. experienced patients; however, this graph should be interpreted with care due to the small number of naive patients (33 patients; 17%). Split for patients with ≤ 1 (naive or “near naive”) vs. > 1 prior biologic (Fig. 2b), the 18 months overall drug survival was 82% and 62%, respectively (no log-rank test performed due to crossing of curves). Drug survival related to ineffectiveness after 18 months was 90% for patients with ≤ 1 prior biologics, vs. 65% for patients with > 1 prior biologic (p = 0.021; see Fig. S2b). The side-effects-related drug survival at 18 months was comparable for the two groups (90% and 89%, respectively).
Fig. 2. Overall drug survival of secukinumab, split for prior biologic use. (a) “n” at risk for naive patients: 33 at baseline, 25 at 6 months, 11 at 12 months, and 3 at 18 months. “n” at risk for experienced patients: 163 at baseline, 121 at 6 months, 72 at 12 months, and 30 at 18 months. (b) “n” at risk for naive or near-naive patients: 71 at baseline, 53 at 6 months, 26 at 12 months, and 7 at 18 months. “n” at risk for experienced patients: 125 at baseline, 93 at 6 months, 57 at 12 months, and 26 at 18 months. §No log-rank test performed due to crossing of curves.
Split according to sex, the overall drug survival was 78% for men vs. 73% for women after 12 months, and 66% for men vs. 68% for women after 18 months (Fig. S3a). Drug survival related to ineffectiveness after 12 and 18 months was similar across sexes: 80% vs. 79% and 70% vs. 74% for men vs. women, respectively. In contrast, side-effects related drug survival emphasized sex differences, with 12-month survival 95% for men vs. 84% for women, and 18-month survival of 93% in men vs. 84% in women (Fig. S3c). Drug survival did not differ when comparing retrospectively vs. prospectively collected data (Fig. S3).
Univariate Cox regression analysis of determinants of drug survival is shown in Table SI. Univariate analysis showed that higher age, higher baseline weight and prior use of >1 biologic could be associated with decreased secukinumab drug survival (p < 0.05, or 95% CI > 1). Psoriatic arthritis was not associated with drug survival in univariate analyses. A multivariate Cox regression analysis would be needed to establish the strength of the independent associations of these variables, but such regression analyses were not performed because of the many (non-random) missing data for baseline variables.
This daily practice study, based on 196 patients receiving secukinumab for psoriasis, showed an overall drug survival rate of 76% after 12 and 67% after 18 months. Drug survival was predominantly determined by discontinuation due to ineffectiveness (64% of all discontinuations). A smaller part (15%) of discontinuations was related to side-effects, concerning mostly fungal infections of the oropharyngeal mucosa. Sixteen percent of discontinuations were due to a combination of ineffectiveness and side-effects. The majority (66%) of patients who discontinued secukinumab due to ineffectiveness, comprised cases who showed a good initial response, but later experienced loss of effect. Another group recently published a case series describing secondary ineffectiveness in 19% of patients, occurring mostly after 24–32 weeks of treatment (12). Drug survival curves in our study did not suggest a sudden loss of secukinumab efficacy after 6 months of treatment. Rather, discontinuations occurred spread over the entire follow-up period, leading to a gradual decrease in drug survival over time (Fig. 1).
Comparing the current results with existing literature, drug survival rates of secukinumab were in the range of those reported for anti-TNF agents. The 12-month drug survival of adalimumab and etanercept, as reported in literature, ranged from 75% to 84% and from 70% to 86%, respectively (10, 13–16). Ustekinumab showed superior drug survival in previous drug survival studies, with 12-month drug survival rates ranging from 84% to 95% (10, 13–16). In addition, drug survival rates from Dutch psoriasis patients (adalimumab, etanercept, ustekinumab, infliximab; BioCAPTURE registry) are visualized and added as a supplemental file, and positioned next to secukinumab drug survival (Fig. S1). It is surprising to find higher drug survival rates for ustekinumab compared with secukinumab in both literature and our own data, given that secukinumab showed superior efficacy to ustekinumab in a head-to-head trial (CLEAR study) (6). A recent drug survival analysis of Egeberg et al. showed slightly lower drug survival rates for secukinumab (estimated 1-year drug survival 68%) (17). The authors used a 60-day threshold as a maximum gap to determine discontinuation, where in the present analysis and other drug survival studies 90 days was used (9, 10, 13, 14, 18–21). In our present study, drug survival was compared using 90 and 60 days thresholds, which were virtually similar (Fig. S5). Al-though not directly translatable to drug survival, Huang et al. (12) also showed a substantial proportion (30%) of patients stopping secukinumab within 32 weeks. However, comparisons between drug survival rates of other biologics and secukinumab data are hindered by patient population differences. For instance, our cohort comprises patients who started secukinumab treatment soon after it became available. New agents are generally introduced more promptly in patients who have failed on (all) other treatments. As a consequence, difficult-to-treat patients were possibly over-represented in the present study. This may be reflected by the small proportion of biologic-naive patients in our cohort (17%), compared with cohorts from previous drug survival studies. For biologic experienced patients, reason of prior treatment discontinuation was often unknown. However, previous studies on drug survival of biologics in psoriasis have shown that the majority of patients discontinue due to ineffectiveness, and only a minority due to side-effects.
To explore whether naivety for biologics was a factor influencing drug survival rates for secukinumab, we performed subanalyses for naive patients, patients with ≤ 1 prior biologics (naive or “near naive”) and patients who had received multiple prior biologics. A striking difference in 18 months drug survival rates was found between patients with ≤ 1 biologics and patients with > 1 prior biologic (82% vs. 62%, respectively). The difference between naive and experienced patients followed the same pattern, but sample size of truly naive patients was limited (33 patients). The difference in drug survival curves between patients with ≤ 1 and patients with > 1 biologic was mainly determined by a higher number of discontinuations due to ineffectiveness in the (near) naive biologic group. Discontinuation due to side-effects did not differ between the ≤ 1 and > 1 prior biologic group (Fig. S2). Previous biologic use was not an exclusion criterion for secukinumab trials, but the trial population was dominated by naive patients nonetheless, with 71–88% of patients being biologic-naive (3). This differs clearly from the composition of the present study cohort. Comparing other characteristics of trial patients with our cohort, we found that the present study included more female patients (39%, vs. 23–36% in trials) and that patients were slightly older (mean 48.9 years vs. 43.9–46.6 years in trials) (3–6). Mean baseline PASI in our cohort was 13.4 (median 10.9), but there were many missing values. In comparison, the mean baseline PASI ranged from 18.9 to 23.9 in the secukinumab trials (3–6). Our findings demonstrate that, due to specific differences in population characteristics, daily practice results may diverge from trial findings, stressing the importance of the former when assessing an agents’ effectiveness.
In drug survival analyses performed for other biologics, sex differences were often noticed. Women frequently showed lower biologic drug survival rates than men (10, 13, 14, 22). A specific relation to side-effects (women stopping a drug due to side-effects more often than men) was previously observed in our BioCAPTURE cohort (13). In the present study, there was a trend towards shorter secukinumab drug survival for women after 12 months, but not after 18 months. A trend for shorter drug survival related to side-effects was detected in women compared with men.
Fungal infections were common in our population, with 13% of patients experiencing at least one episode of a fungal infection during treatment. The incidence rates per 100 patient years for fungal infections were 14.2 (counting only the first event per patient) and 21.6 (counting all events), which is higher than incidence rates of Candida infections found in trials (IR 3.6 in patients on 300 mg every 4 weeks; IR 1.9 in patients on 150 mg every 4 weeks) (23). Notably, adverse events could be under-reported in our cohort, given that part of the data was retrospectively collected. The mucosa was predominantly affected in the current study, with 7% of patients experiencing at least one episode of oropharyngeal fungal infection. Four patients in the current cohort ultimately stopped secukinumab treatment due to (recurrent) fungal infections, in contrast to the secukinumab trials where treatment discontinuations due to fungal infections did not occur (3–6, 24).
The main limitation of the current study is that part of the data was retrospectively collected. This probably did not influence drug survival itself as variables related to such analyses (medication start and stop dates) are normally properly registered in daily practice. Correspondingly, we did not find differences in drug survival curves when splitting for method of data collection (Fig. S4). Reporting of adverse events, however, may differ in retrospective cases when compared with prospectively followed patients. Subanalyses of adverse events showed that fungal infections were reported more frequently in prospectively followed patients than in retrospective cases, although the number of oropharyngeal fungal infections did not differ (data not shown). Another limitation is the small number of biologic naive patients, hampering the analysis of naive vs. experienced patients.
In summary, there was a 76% overall drug survival of secukinumab after 12 months, which is comparable to drug survival of adalimumab and etanercept, and inferior to drug survival of ustekinumab as described in literature. However, direct comparisons are not possible due to the observational nature of data, and differences in patient characteristics (amongst others, included secukinumab patients often failed multiple prior biologics). Patients stopped mostly due to ineffectiveness and less frequently due to side-effects. A trend towards shorter drug survival related to side-effects was detected in women compared with men. It is important to realise that the reported drug survival represents secukinumab performance in an initial cohort of secukinumab-treated patients, where patients with difficult-to-treat psoriasis are possibly overrepresented. Indeed, drug survival rates of patients who had used ≤ 1 prior biologic were higher when compared with patients who had used multiple prior biologics. Furthermore, we found that oropharyngeal fungal infections were more common than expected based on trial data, and were reason for treatment discontinuation in some cases. Our findings illustrate the importance of daily practice studies in complementing data from randomized controlled trials.
The authors would like to thank the following persons for data collection: S Atalay, M Bijen, F Garritsen, L de Koning, ME Kooijmans-Otero, L Schalkwijk, M van der Stok and NMC van de Wijngaart-Pouw.
Disclosures. JMPAvdR carried out clinical trials for AbbVie, Janssen, and Celgene; received speaking fees from AbbVie, Eli Lily, and Jansen and reimbursement for attending symposia of Janssen, Pfizer, Celgene and AbbVie. Fees were paid directly to the institution. All funding is not personal but goes to the independent research fund of the department of dermatology of Radboud University Medical Centre Nijmegen, the Netherlands. LJvV has performed clinical trials for AbbVie, Celgene and Janssen. All funding is not personal but goes to the independent research fund of the department of dermatology of Radboud University Medical Centre Nijmegen, the Netherlands. MBAvD has acted as a consultant for AbbVie, Janssen, LEO Pharma, Pfizer, Prosensa and TEVA, and has been an investigator for Cutanea Life Sciences, Eli Lilly, Idera Pharmaceuticals and Novartis. GEvdK has performed clinical trials for Celgene, Janssen and Novartis. WJAdK has performed clinical trials for AbbVie, Amgen, Celgene, Eli Lilly, Janssen, LEO Pharma, Merck, Novartis and UCB. W.J.A. de Kort has acted as consultant and/or paid speaker for and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including Amgen, Celgene, Eli Lilly, Janssen, LEO Pharma, Novartis and UCB. GPHL has no conflicts of interest to declare. BH has been on the advisory board for Abbvie, Janssen, Novartis, Solenne and UCB Pharma, and has performed clinical trials for Abbvie, Janssen, Novartis and Solenne. BH has received educational grants from Abbvie. MSdB-W has acted as a consultant for Regeneron/Sanofi and as an advisory board member for AbbVie and Regeneron/Sanofi. M.S. de Bruin-Weller has participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie and Regeneron/Sanofi. MdG has performed clinical trials for Celgene and Novartis. MdG has acted as a consultant and/or paid speaker and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including Abbvie, Celgene, Janssen and Novartis. RM has acted as a consultant for Celgene and as a paid speaker for AbbVie and Janssen. PCMvdK has consultancy services for Abbott, Allmirall, Amgen, Celgene, Centocor, Eli Lilly, Galderma, Janssen, LEO Pharma, Mitsibishu, Novartis, Pfizer, Philips, Sandoz. He has carried out clinical trials for: Abbvie, Amgen, Basilea, Eli Lilly, Jansses, LEO Pharma, Pfizer, Philips. PIS has acted as a consultant for AbbVie, LEO Pharma and Novartis and has received independent research grants from LEO Pharma and Schering Plough. PIS has participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis and atopic dermatitis. All funding is not personal but goes to the research fund of the department of dermatology of Amsterdam Medical Centre, Amsterdam, the Netherlands. EMGJdJ has received research grants for the independent research fund of the department of dermatology of Radboud University Medical Centre Nijmegen, the Netherlands from AbbVie, Janssen and Pfizer. EMGJdJ has acted as consultant and/or paid speaker for and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie, Amgen, Celgene, Eli Lilly, Janssen, LEO Pharma, Novartis and Pfizer. All funding is not personal but goes to the independent research fund of the department of dermatology of Radboud University Medical Centre Nijmegen, the Netherlands. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize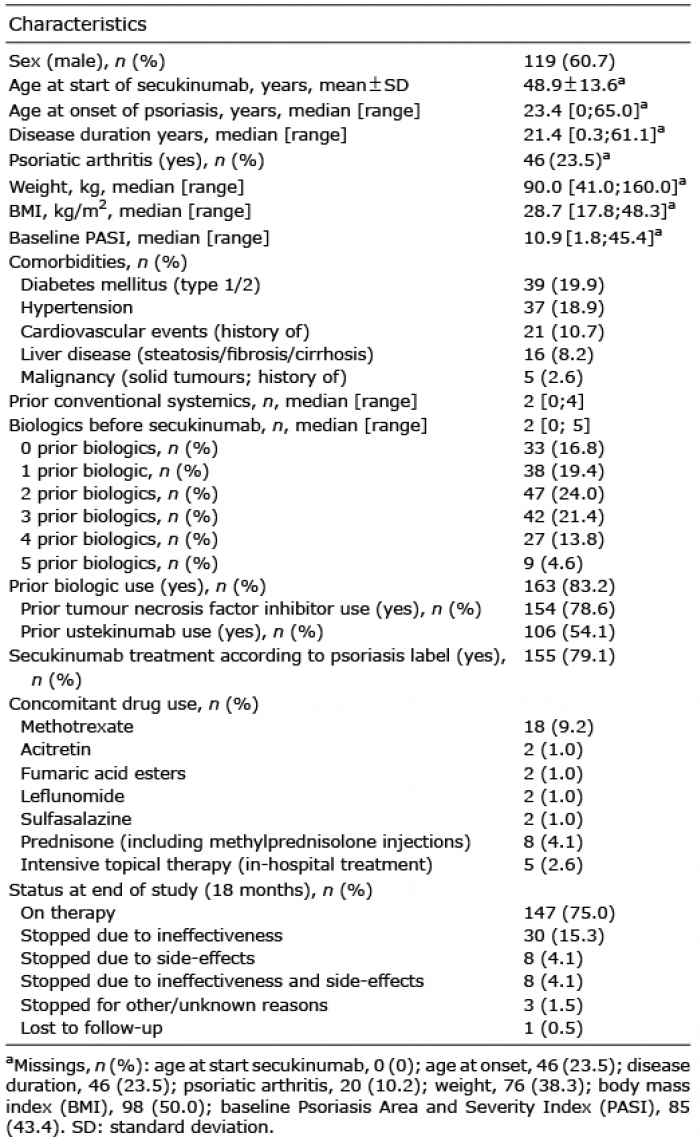 Click to show fullsize
Click to show fullsize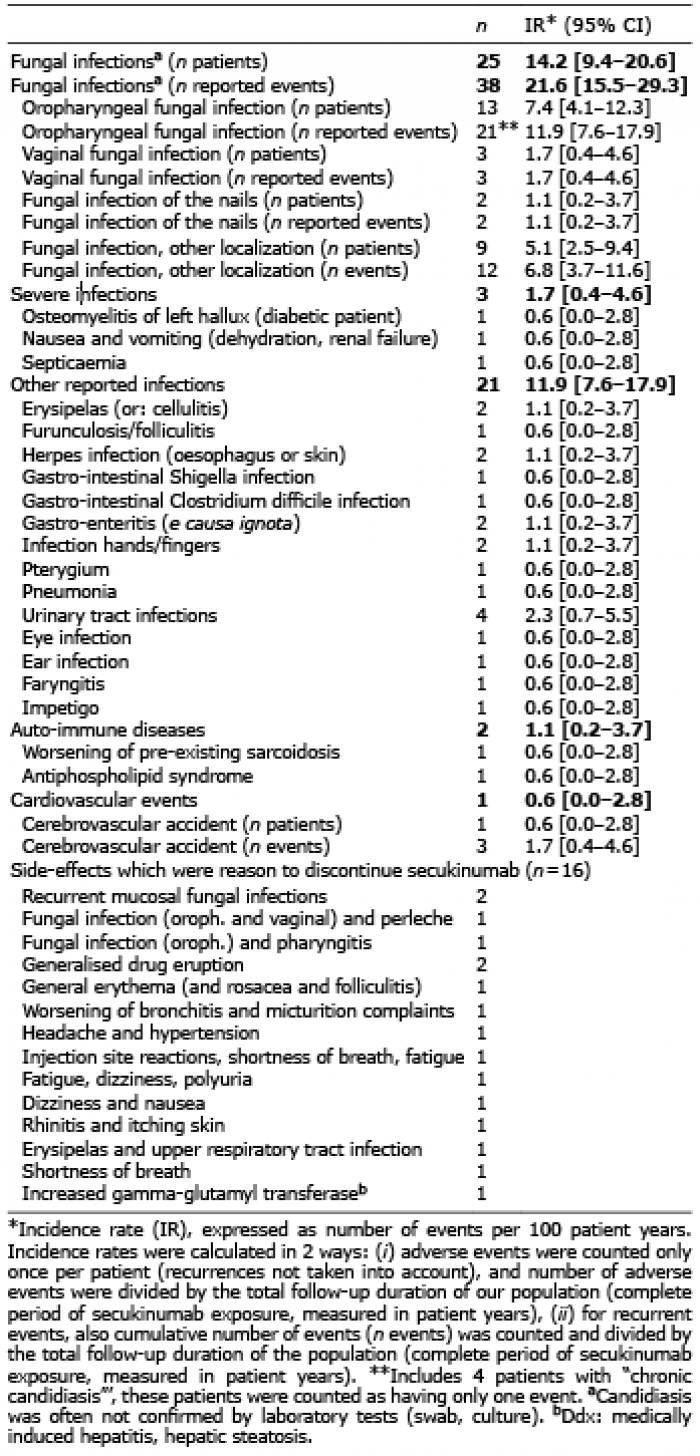 Click to show fullsize
Click to show fullsize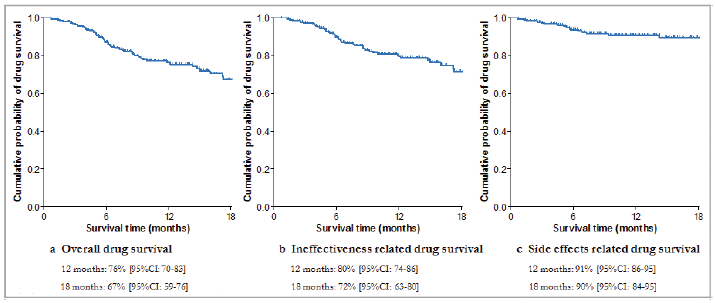 Click to show fullsize
Click to show fullsize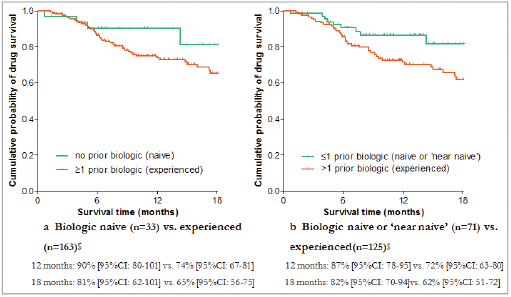 Click to show fullsize
Click to show fullsize