


1Department of Dermatology, Leiden University Medical Centre, Leiden, The Netherlands, 2Statistics Unit, and 3Cancer and Population studies, QIMR Berghofer Medical Research Institute, Brisbane, Australia
Organ transplant recipients (OTRs) have a high incidence of cutaneous squamous cell carcinoma (cSCC), and immunosuppression has been reported to be an important risk factor for metastasis. The aim of this study was to identify the metastasis risk over a 10-year period for 593 patients with cSCC, of whom 134 were OTR and 459 were immunocompetent. Metastasis incidence rate was 1,046 (95% confidence interval (95% CI) 524–2,096) per 100,000 person years in OTR and 656 (95% CI; 388–1,107) in immunocompetent patients, yielding an incidence rate ratio of 1.6 (95% CI 0.67–3.81). In OTRs head/neck location, older age at transplantation and older age at diagnosis of first cSCC were associated with metastatic risk, and 7 out of 8 metastasized tumours were smaller than 2 cm. In immunocompetent patients tumour size and tumour depth were associated with metastasis. In conclusion, we were not able to demonstrate an increased incidence rate of metastasis in OTRs compared with immunocompetent patients. However, OTRs and immunocompetent patients differed with regard to risk factors for metastasis.
Key words: organ transplant recipients; cutaneous squamous cell carcinoma; metastasis; immunocompetent.
Accepted Feb 5, 2018; Epub ahead of print Feb 6, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Roel E. Genders, Department of Dermatology Leiden University Medical Centre, Albinusdreef 2, NL-2333 ZA Leiden, The Netherlands. E-mail: r.e.genders@lumc.nl
Cutaneous squamous cell carcinoma (cSCC) is the second most frequent form of keratinocyte carcinoma (KC) (1, 2). The incidence of cSCC varies globally, with a higher incidence closer to the equator. In Finland the reported incidence for men is 6 per 100,000 person years and for women 4 per 100,000 person years. In Australia, these numbers are reported to be 1,035 and 472 per 100,000 person years, respectively (3, 4).
The incidence of cSCC metastasis varies, with higher incidence often reported from tertiary hospitals (5–10). The risk of developing metastasis from low-risk cSCC in the general population is between 0.5% and 5%, but may be as high as 45% in high-risk cSCC, i.e. tumours located on the lip and ear, large tumours and recurrent tumours (5, 11, 12).
The risk of developing cSCC in organ transplant recipients (OTRs) is 40–250 times increased compared with the general population (13). In some reports, it has been suggested that cSCC in OTRs frequently exhibit aggressive behaviour irrespective of size, that in-transit metastases are more frequent, and that cSCC in OTRs have a worse prognosis than cSCC in immunocompetent patients (14, 15). Between 5% and 23% of all patients with metastatic cSCC, have been reported to be immunosuppressed, many of whom were OTR, and therefore immunosuppression has been reported to be a risk factor for metastasis (16–18).
In clinical practice, it is difficult to identify high-risk cSCC and to detect metastasis at an early stage, both in immunosuppressed and immunocompetent patients (19–21). Tumour size, Clark’s level, Breslow’s thickness, degree of differentiation, perineural invasion and location are associated with the development of metastasis (22). Staging systems are developed to help determine high-risk tumours (23–25). The American Joint Committee on Cancer (AJCC) classification is the most commonly used staging system, and is subject to regular modifications. Since 2010 the AJCC classification is based on several high-risk features of cSCC (23). Though immunosuppression is mentioned as a risk factor, it does not influence tumour stage in any of the staging systems.
OTR are subject to lifelong immunosuppressive therapy and therefore are an ideal population with regard to analysing the influence of immunosuppression on cSCC metastatic behaviour. Comparative studies between OTR and immunocompetent patients focusing on the metastasis risk of cSCC are scarce. The aim of this study was to identify the risk of cSCC metastasis in a defined cohort of OTRs and immunocompetent patients, calculated both per patient as well as per individual tumour.
For this retrospective study, all consecutive patients with primary cSCC who were diagnosed from January 2004 to December 2013 were identified from the institutional oncology database of Leiden University Medical Centre. Each patient’s medical record was cross-checked with pathology records of cSCC in the same period. Missing patients and/or tumours were added to the database manually. Each tumour was given its own record; one individual patient could have had more records in case of multiple primary cSCC. Detailed histopathological information on all tumours was extracted from the Dutch pathology registry (PALGA). Tumours were categorized by differentiation grade (good, moderate, poor, undifferentiated), presence of lymphovascular invasion, presence of perineural invasion, tumour depth, location and tumour size (26). All tumours were classified using the TNM staging classification (AJCC 7th edition).
Patient data were extracted from the institutional oncology database. When missing, additional data were collected from patient files. Status and data of immunosuppression were retrieved from the institutional patient database and patient files.
Patient files for all patients were checked for information on possible development of metastasis in December 2015, i.e. a minimum follow-up of 2 years. In case of metastasis, the cSCC that was most likely to be the index tumour was identified. Cases were defined as patients who developed a metastasis from a cSCC that was diagnosed during the study period.
Follow-up time was defined as the time from cSCC diagnosis to diagnosis of metastasis, death or end of study or to censoring. In our institution OTRs were examined at least every 3 months. Immunocompetent patients were followed clinically based on tumour stage according to national guidelines, i.e. twice a year for the first 1–2 years and once a year in year 3–5 for patients with low-risk cSCC, and every 3 months first year, every 4, 6 and 12 months in year 2, 3 and 4–5, respectively for patients with high-risk cSCC. Screening for metastasis was performed routinely by lymph node palpation, and on indication in high-risk tumours by radiological imaging (ultrasound, X-ray, magnetic resonance imaging (MRI), computed tomography (CT) or positron emission tomography (PET) scan). Sentinel lymph node procedure was not performed.
Descriptive statistics were used for patient and tumour characteristics at baseline. Frequencies, percentages, median, mean and range were calculated, when appropriate. Patients that were immunosuppressed for other reasons than organ transplantation were excluded. Univariable Cox regression analysis was used to identify risk factors for metastasis, excluding cases with missing values for each variable. Multivariable analyses were not carried out due to limited number of events. A p-value < 0.05 was set as statistically significant for all analyses. Statistical analysis was performed using SPSS version 23 (SPSS, Chicago, IL, USA). Incidence rate per person year of metastasis was calculated using STATA 13.1.
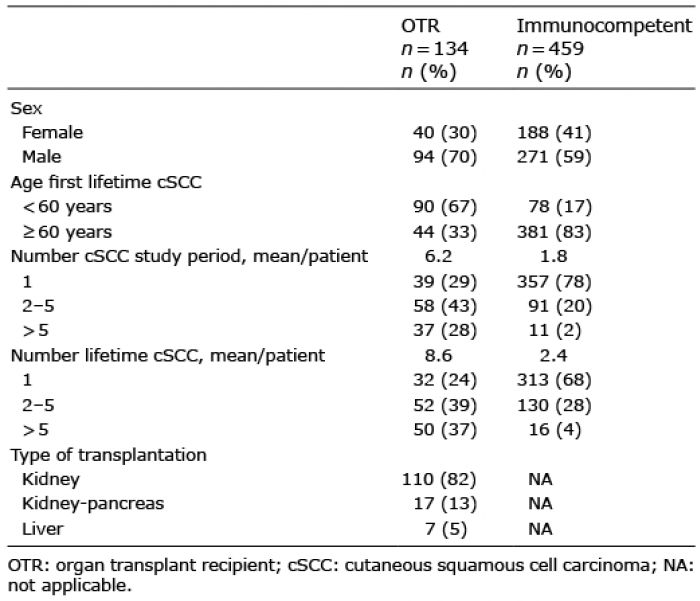
During the follow-up time of median 4.0 years (range 1 month–10.8 years), 1,792 cSCCs were diagnosed in 665 patients, with up to 116 cSCCs in one patient. After exclusion of one OTR who had developed a cSCC one year before transplantation, 66 patients who were immuno-suppressed for reasons other than organ transplantation (inflammatory disease or haematological malignancy) and 6 patients who had developed a metastasis from a cSCC diagnosed prior to the study period, the study cohort consisted of 134 OTRs and 459 immunocompetent patients (Table I).
Table I. Baseline characteristics of 593 patients with cutaneous squamous cell carcinoma (cSSC)
In all, 23 patients (3.9%; 95% CI 2.6–5.8) developed a metastasis from a cSCC diagnosed in the study period, 8 (6.0; 95% CI 3.1–11.3) OTRs and 15 (3.3%; 95% CI 2.0–5.3) immunocompetent patients. The incidence rate (IR) for metastasis was 1,046 (95% CI 524–2,096) per 100,000 person years in the OTR group and 656 (95% CI; 388–1,107) in the immunocompetent patient group, yielding an incidence rate ratio (IRR) between OTRs vs. immunocompetent patients of 1.6 (95% CI 0.67–3.8). Median time between cSCC diagnosis and metastasis diagnosis was longer in the OTR group than in the immunocompetent group, 17.5 and 10.5 months, respectively. Distant site metastasis was found in 1 OTR and in 5 immunocompetent patients, of whom 3 also had concomitant nodal metastasis.
Patient, tumour and metastasis characteristics are shown in Table II and Table III. Univariate hazard ratios for metastasis are listed in Table III. Having a first cSCC at an older age was significantly associated with an increased risk of metastasis in OTRs (Hazard ratio (HR) 8.3, 95% CI: 1.7–41.8). In the immunocompetent group, all patients (15) with metastasis developed their first cSCC after the age of 60 years. In OTRs, being transplanted at 60 years or older (HR 5.0, 95% CI 1.2–21.7), increased the risk of metastasis. Having multiple cSCCs was not associated with increased risk for metastasis in either group. cSCC located in the head and neck area was a risk factor for metastasis, both in the OTR group (HR 16.9, 95% CI 2.1–138.5) and in the immunocompetent group (HR 3.8, 95% CI 0.85–16.9), but statistically significant only in the OTR group. In the OTR group T stage, tumour size, differentiation grade and depth of invasion were not associated with increased metastasis risk. T stage of 2 or higher, tumour size and tumour depth beyond the dermis were associated with increased risk of metastasis in the immunocompetent group. In the OTR group, perineural invasion was not found in any metastatic cSCC and in 3 non-metastatic cSCC, but was observed in 1 metastatic cSCC and in 9 non-metastatic cSCC in the immunocompetent population. Lymphovascular invasion was only seen in 1 non-metastatic cSCC in OTR and in 2 non-metastatic cSCC in immunocompetent patients.
Table II. Patient and tumour characteristics in 23 patients with metastatic cutaneous squamous cell carcinoma (cSCC)
Table III. Univariate hazard ratios for patient and tumour characteristics as risk factors for metastasis in patients with cutaneous squamous cell carcinoma (cSCC)
This study was not able to demonstrate a significantly increased risk for metastasis from cSCC in OTRs compared with immunocompetent patients with cSCC. However, the risk factors appeared to be different between the 2 groups.
With cSCC metastases incidences of 6.0% in OTR and 3.3% in the immunocompetent patients the incidence of metastasis from this study was lower than in other studies. In OTR metastases incidences of 7–14% are reported for low-risk tumours and 10–20% for high-risk tumours (1, 9, 18, 27–30). In the general population, the overall incidence varies between 2.3% and 9.9% (31). For low-risk tumours the risk is between 0.5% and 5% and may increase to more than 20% in high-risk cSCC (5, 11, 12).
The mean time between diagnosing the cSCC and detecting metastasis was longer in the OTR group than in the immunocompetent group. The OTR group had a median time of 17.5 months to develop metastasis, compared with 10.5 months in the immunocompetent group. This was a surprising finding, considering both the immunosuppressed state leading to decreased immunological tumour surveillance and the increased clinical surveillance of OTRs. As the majority of tumours in OTRs were not located in the head and neck area, in contrast to the immunocompetent group, this difference in tumour distribution could contribute to the relatively low risk of metastasis in OTRs. In other studies, the median time to develop metastasis is reported from 4 to 12 months (32, 33).
In OTR, age over 60 years at transplantation and at time of first cSCC diagnosis were risk factors for metastasis. This is in line with previous studies (34). As OTRs developed their first cSCC at a younger age than immunocompetent patients, this could explain the relatively low number of metastasis in OTRs. Most OTRs in our study were renal transplant recipients and have somewhat different immunosuppressive treatment regimens than other OTRs, especially heart transplant recipients (35–37). This could contribute to different incidence rates of cSCC metastasis across the literature.
In our immunocompetent patients, tumour size and depth, and subsequently T-stage, were significant risk factors for metastasis, as shown in other studies (5, 9, 28, 38, 39). In our OTRs we did not find these associations. Tumour size is a well-known risk factor for metastatic lesions (5, 9, 19, 40–43) with an association between increasing tumour thickness and lesion size (18). In our study, 7 out of 8 cSCC that metastasized in OTR were less than 2 cm in diameter and most of the tumours were low-risk T1 tumours. This suggests that OTRs with relatively small tumours (<2 cm) are already at an increased risk of developing metastasis from cSCC, and are less dependent on specific tumour characteristics (18, 44). OTRs have regular clinical follow-ups, and small tumours should therefore be diagnosed before they grow into large tumours. Although it is published that patients with multiple cSCC are at an increased risk of metastasis (45), we were unable to confirm that having multiple tumours led to a higher risk of metastasis. Given the low number of metastases in our OTR group and with metastases developing mainly from relatively small tumours, frequent follow-up of OTRs should continue.
This study has several limitations. First, there was only a small number of patients with metastasizing cSCCs in the OTR group. It was, therefore, difficult to estimate the effect size for risk factors. We acknowledge that statistical analysis should be considered insufficient and only indicative. We also had too few cases to perform multivariable analyses to control for possible confounders. Secondly, the Leiden University Medical Centre is a tertiary referral centre for selected patients with cSCC. Due to this selection bias, extrapolation of our results is difficult, as one should expect a higher rate of metastasis in immunocompetent patients with cSCC referred to the hospital. Finally, the cSCCs in our cohort were diagnosed by several pathologists without a systematic re-evaluation of the histopathological slides. This might have introduced some error, but probably not bias, as no differences are expected in how pathologists will evaluate tumours from OTRs and immunocompetent patients.
To conclude, the metastatic rate of cSCC in OTRs and immunocompetent patients in this study is lower than in most other studies. We were not able to demonstrate an increased risk of metastasis in OTRs compared with immunocompetent patients. Most tumours that did metastasize in OTRs were small tumours without high-risk features. Close and regular inspection of the skin with adequate and rapid diagnosis and treatment of cSCC is important to prevent metastasis.
The authors thank Jan Molenaar, Jan Oosting and Mandy Way for their contributions to this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize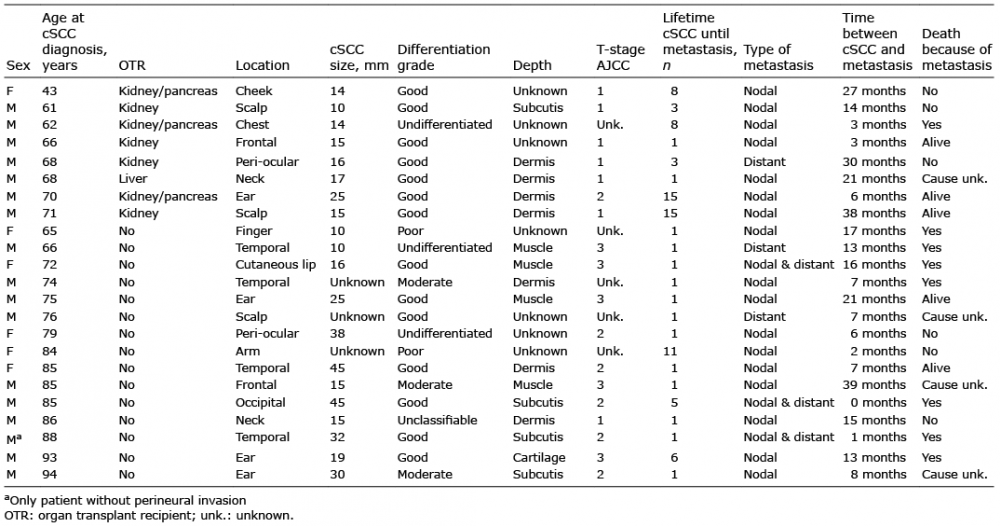 Click to show fullsize
Click to show fullsize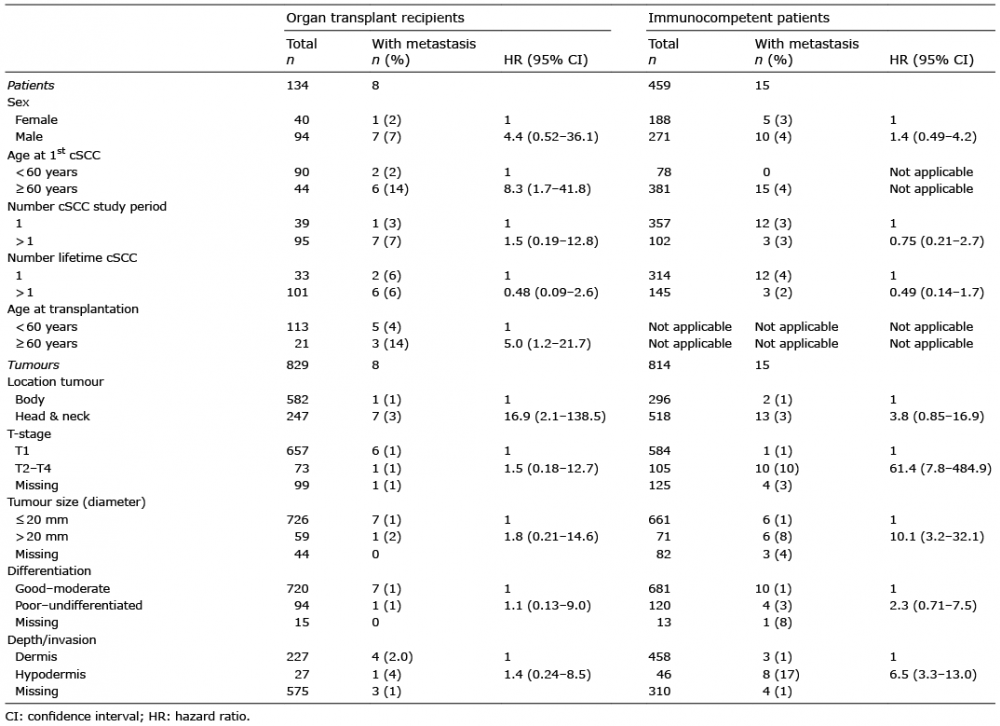 Click to show fullsize
Click to show fullsize