


1Dermatology Department, Gregorio Marañon General University Hospital & Hospital Dermatológico Internacional, Madrid, 2Dermatology Department, 3Molecular Biology Laboratory and 4Pathology Department, Instituto Valenciano de Oncología, Valencia, Spain, 5Division of Molecular Genetic Epidemiology, German Cancer Research Center, Heidelberg, Germany, and 6School of Medicine, Universidad Católica de Valencia “San Vicente Ferrer”, València, Spain
The aim of this case-case study was to determine the differences between dysplastic and common naevus-associated melanomas (NAM) and de novo melanomas. A total of 1,021 prospectively collected patients with invasive cutaneous melanoma from an oncology referral centre were included in the study. Of these, 75.51% had de novo melanomas, 12.93% dysplastic NAM, and 11.56% common NAM. Dysplastic NAM, compared with de novo melanomas, were associated with intermittently photo-exposed sites, atypical melanocytic naevi, decreased tumour thickness, and presence of MC1R non-synonymous variants. Common NAM presented more frequently on the trunk and were of the superficial spreading type. Comparison of dysplastic with common NAM showed significant difference only with regard to mitoses. Both subtypes of NAM shared less aggressive traits than de novo melanomas, albeit with no significant differences in survival after multivariate adjustment. In conclusion, NAM present with less aggressive traits, mostly due to a greater aware-ness among patients of changing moles than due to their intrinsic biological characteristics.
Key words: cutaneous malignant melanoma; naevus, pigmented; sunburn; pathology; molecular biology; MC1R.
Accepted Feb 13, 2018; Epub ahead of print Feb 13, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Eduardo Nagore, School of Medicine, Universidad Católica de Valencia, c/Quevedo, 2, ES-46001 València, Spain. E-mail: eduardo_nagore@ono.com
In Caucasians 5–85% of cutaneous melanomas are clinically or histologically associated with pre-existing melanocytic naevi. These figures are generally lower when the remnants of pre-existing naevi are histologically determined (4.7–50%) (1–3) and higher if based on patients’ recall of a clinically evident precursor lesion (42–85%) (4, 5). A recent meta-analysis estimates that 29.1% of melanomas probably arise from a pre-existing naevus (6).
Melanomas that are histologically associated with melanocytic naevi (NAM) may be associated with almost any melanocytic proliferative lesion; however, they are mainly found in conjunction with dysplastic or common acquired naevi and, to a lesser extent, with congenital naevi (7). Current evidence supports the view that NAM, regardless of the type of melanocytic benign lesions, are associated with relatively young age at diagnosis, personal history of sunburns, and high melanocytic naevi count. In addition, NAM have been linked with location (predominantly on the trunk), superficial spreading melanoma subtype, and have less surrounding solar elastosis, thinner Breslow’s index, and absence of ulceration (1–3, 8, 9). Nonetheless, many studies report no differences in ulceration (4, 5, 10).
Common acquired naevi differ from dysplastic naevi clinically, histologically and at the molecular level, usually with divergent traits and risks that lead to their formation. It has been suggested that a medical history of high level of cumulative sun exposure plays a role in the appearance of multiple common naevi, while intense sunburns during childhood lead to the development of dysplastic naevi (11–15).
To our knowledge, there are no published studies separately comparing common and dysplastic NAM with de novo melanomas. We hypothesize that, given the differences between multiple common naevi and the presence of dysplastic naevi, the melanoma associated with dysplastic and common melanocytic naevi could differ considerably, and similar differences may exist between melanoma associated with naevi and melanomas arising de novo.
The aim of this study was to assess the clinical, epidemiological, histopathological and molecular differences between common and dysplastic NAM, and between each of these subsets and de novo melanomas.
A retrospective, observational study was performed using data (collected before the design and development of the present study) from the melanoma database of the Dermatology Department of the Instituto Valenciano de Oncologia (IVO), Valencia, Spain. This database, launched in 2000, has been regularly updated with data from newly diagnosed and follow-up melanoma patients. Clinical, epidemiological, and histological data are collected prospectively from the medical history and physical examination of patients, and the information regarding disease evolution is updated on a daily basis by dermatologists with experience in management of melanoma (16).
The study was approved by the IVO’s research ethics board. Informed consent was obtained previously from the participants.
Only incident patients with invasive cutaneous melanoma who had received definitive treatment at our institution between 1 January 2000 and 31 December 2012 were included in the study. Patients with in situ melanomas, mucosal or ocular melanomas, metastatic melanomas with unknown primary tumour, and melanomas associated with other melanocytic lesions (congenital naevi, blue naevi, naevus spilus, etc.), and cases with no information about the presence of remnants of previous melanocytic naevi were excluded from the analysis. We also excluded those patients presenting multiple primary melanomas, since this could bias and modify the survival analyses.
Patients were classified according to whether remnants of pre-existent dysplastic or common melanocytic naevus were observed during pathological examination. Thus, patients were not classified in this group based on clinical criteria (17). Common melanocytic naevi included junctional, compound and intradermal naevi, exhibiting no architectural or cytological dysplastic features. Dysplastic or Clark naevi were defined based on the pathology subgroup of the European Organisation for Research and Treatment of Cancer (EORTC) Malignant Melanoma Cooperative Group diagnostic criteria (18). Gradation of melanocytic dysplasia was not considered in this study. Three groups were defined: group A: melanomas with no associated naevi (i.e. de novo melanomas); group B: melanomas associated with dysplastic melanocytic naevi (dysplastic NAM); and group C: melanomas associated with common melanocytic naevi (common NAM).
The following variables were used for comparative analysis:
Differences between the distribution of each variable according to the categories were evaluated using Pearson’s χ2 test. Odds ratios (OR) were calculated through univariate and stepwise forward multivariate logistic regression. Logistic regression analyses quantifying the association between the different variables and measures were performed in 3 pairs: common NAM vs. de novo melanomas, common NAM vs. dysplastic NAM, and dysplastic NAM vs. de novo melanomas. For multivariate analyses, missing values were imputed using a complete case (multiple imputation) model (20), for which 5 iterations were run and combined estimates and standard errors using Rubin’s rules. Prior to the development of the model, we tested if the data were randomly missing, using the missing values add-on module in the SPSS statistical package. Survival analyses considering as endpoints separately disease-free survival, overall survival and melanoma-specific survival were performed. Differences in survival probabilities were calculated by the Kaplan–Meier method and the differences evaluated by the log-rank test. Multivariate analyses were performed by forward stepwise Cox regression models to adjust for all selected variables. Proportionality assumption was graphically assessed by log (–log) survival plots. Statistical significance was 2-tail and established for p-value < 0.05. All the statistical analyses were performed using the SPSS statistical package for Windows, version 20.0 (IBM Corporation, Armonk, NY, USA).
Out of 1,430 patients, 1,021 met the inclusion criteria (Fig. S1). The median age of the patients at diagnosis was 56 years (interquartile range (IQR) 43–68 years). A total of 771 patients (75.5%) presented with de novo melanomas, 132 (12.9%) with dysplastic NAM, and 118 (11.6%) with common NAM.
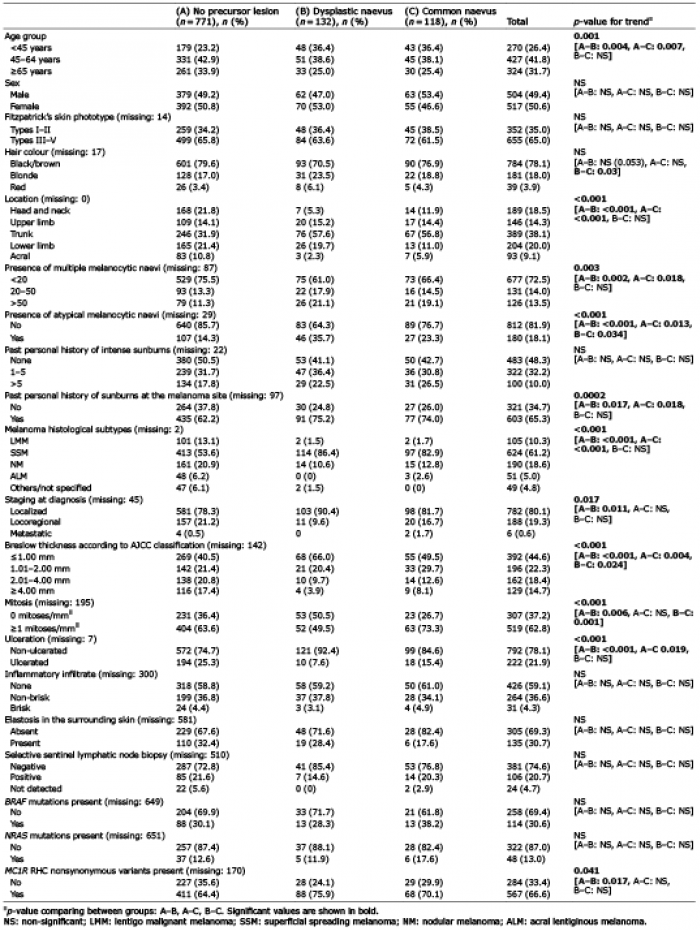
The characteristics of the studied population and results from exploratory χ2 analyses are shown in Table I, and binary logistic regression analyses are shown in Table II.
Table I. Sample description. Univariate (χ2) analyses results
Table II. Univariate and multivariate binary logistic regression analyses results
Dysplastic NAM, compared with de novo melanomas, were associated with young age (< 45 years), location on the trunk and upper extremities, presence of multiple melanocytic naevi (> 50), presence of clinically atypical melanocytic naevi, history of mild or intense sunburns at the melanoma site, SSM histological subtype, lower Breslow thickness and mitosis count, and absence of ulceration. Multivariate analyses confirmed associations with location on the trunk (OR 5.8 (95% confidence interval (95% CI) 1.7–19.7)) or upper extremities (OR 4.5 (1.2–16.9)), presence of clinically atypical melanocytic naevi (OR 1.8 (1.0–3.1)), thinner tumours (< 1 mm: OR 7.3 (2.6–20.6); 1.01–2 mm: OR 4.3 (1.4–12.9)), and the presence of MC1R non-synonymous variants (OR 1.4 (1.1–1.9)). No statistically significant differences were found for presence of BRAF and NRAS mutations among the 3 subgroups investigated.
Common NAM, compared with de novo melanomas, were also associated with young age, location on the trunk, presence of multiple melanocytic naevi (> 50), presence of atypical melanocytic naevi, history of intense sunburns at the melanoma site, superficial spreading and nodular histological subtypes, thinner tumours, 1–5 mitoses/mm2, and absence of ulceration. Multivariate analyses showed that the most significant associations were location on the trunk (OR 2.8 (1.5–5.3)) and SSM subtype (OR 11.9 (2.9–48.6)).
Comparison of 2 NAM subtypes showed that common NAM were less frequent on the lower extremities than in patients with clinically atypical melanocytic naevi, but were more frequently associated with the presence of mitoses. Multivariate logistic regression, however, showed that the only statistically significant differences between the 2 subtypes were in terms of mitosis count; common NAM harboured increased mitoses counts (OR 2.6 (1.3–5.1)).
Analyses with a median follow-up of 55 months showed statistically significant differences in disease-free and melanoma-specific mortality survival (Fig. 1) between NAM subgroups and de novo melanomas. The results showed median disease-free survival of 35.9 months for patients with de novo melanoma, 60.4 months for patients with both subtypes of NAM (48.4 months for patients with dysplastic NAM, and 66.8 months for patients with common NAM). Median overall survival was 44.5 months for patients with de novo melanoma, 61.7 months for patients with both subtypes of NAM (52.8 months for patients with dysplastic NAM and 72.5 months for patients with common NAM). This was also seen when comparing NAM in general with de novo melanomas (Fig. 2). However, multivariate adjustment showed that these differences were dependent on other characteristics rather than histological association with a pre-existing naevus (Table SI).
Fig. 1. Disease-free survival (DFS) and melanoma-specific survival (MSS) comparing de novo melanomas with naevus-associated melanomas (NAM) subgroups.
Fig. 2. Disease-free survival (DFS) and overall survival (OS) comparing de novo melanomas with naevus-associated melanomas (NAM).
Some authors have stated that individual melanocytes undergo clonal expansion and senescence to become melanocytic naevi (21–23). However, naevi very infrequently transform into a melanoma (the estimated individual accumulated risk until 80 years of age for melanoma transformation of an individual naevus has been calculated as 0.03% among men and 0.009% among women) (24). Certain genetic mutations are known to be present in both naevi and melanomas, and the process leading to the change from melanocytes to intermediate lesions and, finally, to melanoma involves a number of additional molecular alterations (25, 26). The melanocyte-naevus-melanoma model includes the patients belonging to 1 of the 2 pathways (the “naevogenic” pathway) proposed for the development of melanoma (27, 28). However, this model does not fit certain histological subtypes of melanoma (mainly LMM and ALM), and cannot be applied to all cases in which clinical evidence suggests a NAM.
The subject of naevus-associated melanomas (NAM) is controversial and some questions remain unanswered. The present study, based on a prospective series of 1,021 patients with cutaneous melanoma, is the first to separately assess dysplastic and common NAM together with clinical, histological and molecular factors. Dysplastic NAM, compared with de novo melanomas, associate with intermittently sun-exposed sites, such as trunk and upper extremities, the presence of clinically atypical melanocytic naevi, thin tumours, and the presence of MC1R non-synonymous variants. Common NAMs, on the other hand, associate with intermittently sun-exposed sites and SSM type. Comparison of dysplastic with common NAM showed that the only difference between the 2 was that the latter had an increased number of mitosis.
The proportion of NAM in our study is similar to that in some of the previously published series, although somewhat lower than in a recently published meta-analysis (9, 29–31). Both subtypes of NAM were associated with intermittently sun-exposed areas; in patients with non-synonymous MC1R variants, dysplastic NAM were more frequent. These factors highlight the importance of sun exposure reflected through high cumulative exposure and a past personal history of sunburns, which have been identified previously as important in NAM (1–3). NAM present more frequently as SSM and, in general terms, share better prognostic characteristics than de novo melanomas, as seen previously (1–3, 8, 9). This study shows that dysplastic NAM characterize tumours with more benign histopathological features than common NAM. However, we did not find differences in survival in multivariate analyses, as indicated previously (9). However, another study showed better survival in NAM vs. de novo melanoma (32).
As the previous findings are in accordance with a divergent pathway model, the case for assessment of the type pre-existing melanocytic in NAM is augmented (28, 32). We hypothesize that, although BRAF and NRAS mutational status was not significant in our analyses, other biological factors may be relevant for those differences (15).
The fact that dysplastic NAM had lower counts of mitoses than common NAM could be an indication of non-compliance with Clark’s theory of naevi-melanoma progression (33). It is accepted that the diagnosis of a dysplastic naevus should be considered as a marker for melanoma risk, but there is currently no clear evidence demonstrating that these naevi have a high predisposition to evolve into a melanoma (34). We also consider that the generally more favourable features among NAM can be attributed to a higher awareness of the need for periodic check-ups of moles and pre-existing lesions. This message has been repeated in melanoma screening campaigns, and has probably reached prominently to those patients with dysplastic naevi. Thus, along with the disparate results exhibited by 2 recent studies (35, 36), we believe that future screening and skin cancer awareness campaigns should insist on identification of new lesions, which may present with worse prognostic traits.
All of the patients in the current study were collected prospectively, following homogeneous criteria, from a national reference centre (with a large geographical referral area, and therefore could probably be extrapolated to most Spanish patients with melanoma). However, this study has certain limitations, such as its relatively limited sample, which may have prevented the detection of some associations, its retrospective approach, which implies certain inherent constraints, and the absence of information of the treatment received by patients after metastatic dissemination, which may have influenced the survival figures. Furthermore, molecular analyses were not performed on all of the specimens and were not specifically directed to confirm that the adjacent melanocytic naevi were indeed precursor lesions, given that most, but not all of NAM, correspond to naevi being precursor lesions to melanoma (37). Finally, although histopathological diagnosis was performed by a single expert dermatopathologist, and difficult-to-diagnose cases were discussed and confirmed by a multidisciplinary committee including subspecialized dermatologists and dermatopathologists, a potential classification bias is possible, which could explain the more benign histopatho-logical features observed among dysplastic NAM (38).
In conclusion, previously published epidemiological and histopathological factors were confirmed in our study, and some other features were identified, thanks to separating common and dysplastic NAM into different groups. NAM are more common on intermittently sun-exposed sites. This is a more important factor among dysplastic NAM, which is more frequent among patients carrying at least 1 RHC MC1R non-synonymous melanoma-associated variant. More benign histopathological features favouring dysplastic NAM (vs. common NAM) have been seen, and both subtypes of NAM are more frequently SSM, sharing less aggressive traits than de novo melanomas, although no significant impact on survival has been observed.


 Click to show fullsize
Click to show fullsize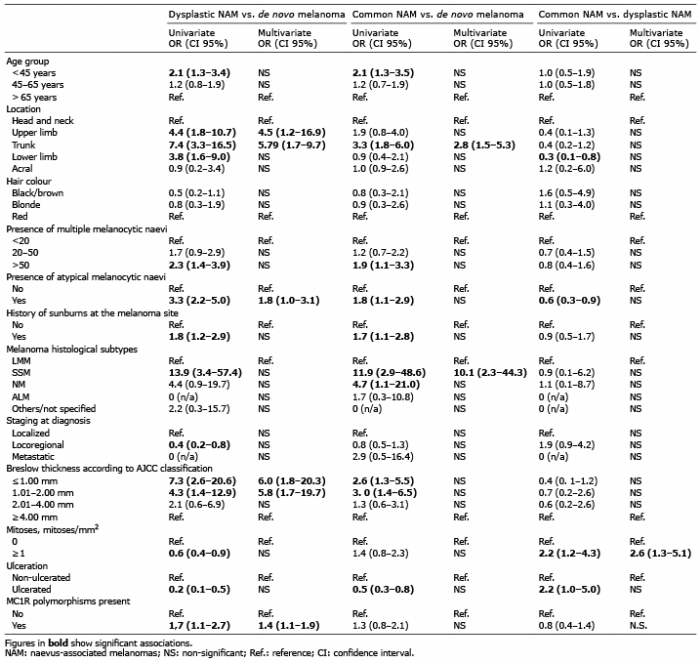 Click to show fullsize
Click to show fullsize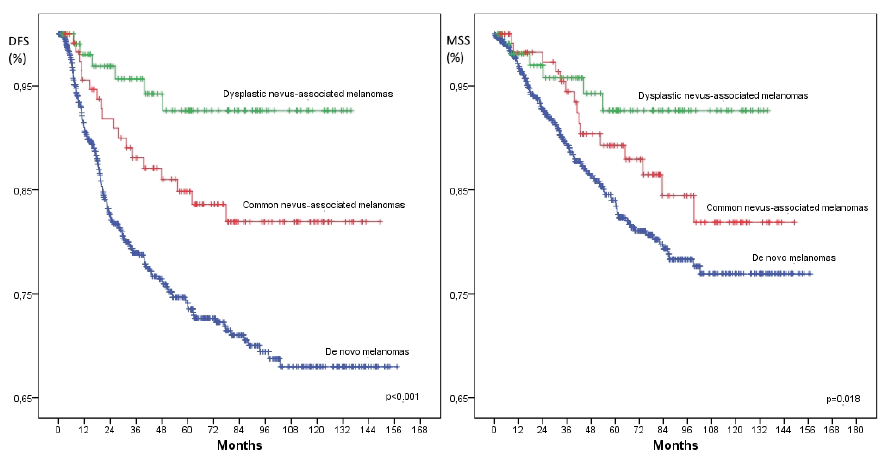 Click to show fullsize
Click to show fullsize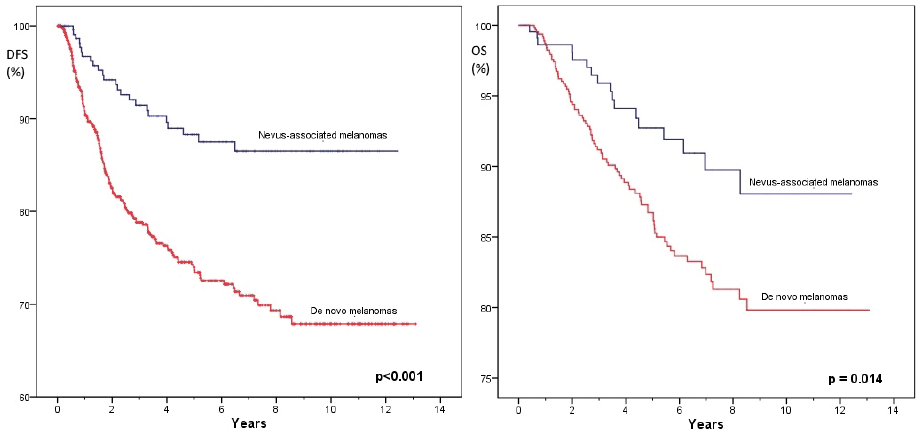 Click to show fullsize
Click to show fullsize