


1Department of Dermatology and Allergy and 2Department of Cardiology, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, 3The Danish Heart Foundation, 4The National Institute of Public Health, University of Southern Denmark, Copenhagen, Denmark, and 5Eli Lilly and Company, Indianapolis, IN, USA
It is unclear whether psoriasis is a progressive disease that requires early aggressive intervention. This population-based study identified patients with psoriasis and psoriatic arthritis (PsA). Survival analysis and Kaplan–Meier life table techniques were used. The study comprised 10,011 psoriasis patients (severe n = 4,618), and 1,269 patients also had PsA. Incidence of PsA increased with duration of cutaneous symptoms (p = 0.0001). Psoriasis diagnosed before age 20 or 30 years, respectively, suggested a lower risk of PsA than psoriasis diagnosed after age 50 years, yet age at first cutaneous symptoms did not predict development of PsA. No clear association with disease severity was found. PsA incidence appeared stable with longer duration of psoriasis, but further data are needed to firmly establish the relationship with age of psoriasis onset.
Accepted Feb 20, 2018; Epub ahead of print Feb 28, 2018
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Alexander Egeberg, Department of Dermatology and Allergy, Herlev and Gentofte Hospital, Kildegårdsvej 28, DK-2900 Hellerup, Denmark. E-mail: alexander.egeberg@gmail.com
Cutaneous psoriasis (henceforth “psoriasis”) is a manifestation of psoriatic disease, a chronic systemic inflammatory condition that affects 2–3% of Europeans, and up to 8% of populations in isolated parts of the northern Europe, in particular Scandinavia (Norway) (1). Plaque psoriasis (psoriasis vulgaris) is the most common form of psoriasis and is reported to account for almost 90% of all cases (2). The majority of patients (approximately 70–80%) have mild disease, i.e. psoriasis that can be managed with topical treatment alone (2, 3). Clinically, psoriasis is characterized by sharply demarcated hyperkeratotic and scaling plaques, which may be either localized or widespread, and a common extracutaneous manifestation includes psoriatic arthritis (PsA) (4).
Psoriasis and PsA frequently co-exist (5, 6). Patients with PsA display increased inflammation of the peripheral joints and skeleton, and may also have extra-articular manifestations, such as enthesitis and other musculoskeletal manifestations (7, 8). While severity and prevalence of the different disease manifestations in PsA can differ greatly, the clinical picture may sometimes overlap with that of seronegative rheumatoid arthritis and ankylosing spondylitis, making the diagnosis difficult (8). It is well-established that most patients with PsA develop psoriasis prior to onset of their arthritic symptoms, but the exact clinical relationship is insufficiently understood (9). For example, some studies have suggested a relationship between both severity and duration of psoriasis and the development of PsA, yet other reports have suggested that the incidence of PsA remains constant after the initial diagnosis of psoriasis (10–12). Nevertheless, on a population level the incidence of PsA is steadily increasing across all age groups (13). To date, predictors for development of PsA have been identified, including severe psoriasis, nail involvement, low educational level, and uveitis, few of which are modifiable (14). The incidence of PsA is highest among patients in their fifth decade, the male-to-female ratio is 1:1, and the disease is most frequent among Caucasians (13, 15). Obesity is a reasonably well-established risk factor for PsA among patients with psoriasis, yet while some studies have suggested that smoking, alcohol use, and the anatomical location of psoriasis may also be risk factors, the evidence for these are scarce and there is a need for additional studies to predict development of PsA in patients with psoriasis (16). We therefore examined the effect of duration of psoriasis on the risk of developing PsA in a nationwide cohort in Denmark.
Study approval was obtained from the Danish Data Protection Agency (ref. 2007-58-0015, int. ref. GEH-2014-018, I-Suite 02736). Danish register-based studies are exempted from ethics committee and institutional review board approvals. We conducted and reported the study in accordance with the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (17). All records, including source codes for the present study, are kept at secured and encrypted servers held by Statistics Denmark.
Individual-level information was linked from nationwide administrative registers using a unique and unambiguous personal identification number that all Danish residents are assigned at birth or migration. The Civil Registration System (18) contains information on sex, date of birth, and updated information on vital status and emigration, thus minimizing loss to follow-up. All inpatient and outpatient (ambulatory) hospital consultations are recorded in the Danish National Patient Register (19) (DNPR) according to the International Classification of Diseases, 8th revision (ICD-8) prior to 1994, and according to the 10th revision (ICD-10) thereafter. Since 1994, all pharmacy-dispensed medication has been registered in the Danish Registry of Medicinal Products Statistics according to the Anatomical Therapeutic Chemical (ATC) classification (20), and drugs given directly from hospital clinics or during admission are recorded in the DNPR.
Among the entire population alive and resident in Denmark on 31 December 2012, were identified all patients with a first-time hospital dermatologist diagnosis of psoriasis vulgaris (ICD-10 L40.0, ICD-8 696.19) within the 18-year period up until 31 December 2012 (i.e. from 1 January 1995 until 31 December 2012). As patients may display cutaneous symptoms for some time prior to being diagnosed by a dermatologist, we also collected data regarding the date of their first claimed prescription for topical corticosteroids (ATC D07) or topical vitamin D analogues (ATC D05AX) as these therapies may have been prescribed for the condition before a dermatologist has formally diagnosed the patient. Among patients with cutaneous psoriasis, all patients with a rheumatologist diagnosis of PsA (ICD-10 M07.0-3 and M09.0, ICD-8 696.09) were identified. To ensure accuracy of diagnoses only those diagnoses made by dermatologists (psoriasis) and rheumatologists (PsA), respectively, were included. Patients were classified as having severe cutaneous psoriasis if they received systemic therapy for the condition (biological drugs (adalimumab, efalizumab, etanercept, infliximab, or ustekinumab), ciclosporin, psoralen plus ultraviolet A (PUVA), retinoids, or methotrexate) after the onset of psoriasis but before diagnosis of PsA.
For comparability with previous published findings, we used a similar statistical method to Christophers et al. (10). Thus, we dichotomized patients (psoriasis with PsA/psoriasis without PsA), and compared age, sex, duration of psoriasis, and age at time of diagnosis using Students t-test and Fischer’s exact test. The per-year incidence and prevalence of PsA was estimated using survival analysis, and the cumulative risk of PsA was calculated through use of Kaplan–Meier life tables; i.e. estimates were made based on the length at which psoriasis had been diagnosed at the time of PsA development. The per-year incidence of PsA was calculated based on the number of patients developing PsA of the total number of patients still at risk of incident PsA derived from the ltable function in Stata. Patients (n = 139) who had received a diagnosis of PsA before or on the same day as they were diagnosed with psoriasis were excluded. Two different sets of analyses were performed; first the date when patients were diagnosed with psoriasis by a dermatologist was used as the exposure, and thereafter the time of first cutaneous symptoms (defined as the time of first claimed prescription of topical corticosteroids or topical vitamin D analogues) was used as the exposure. In both sets of analyses, follow-up time was determined as the difference between diagnosis of psoriasis, or time of first cutaneous symptoms, respectively, and 31 December, 2012. A Poisson regression model was used to assess the incidence rate ratio (IRR) of PsA over time following prescription of first cutaneous symptoms. In addition, analyses were performed to assess the potential impact of age at psoriasis diagnosis on the risk of developing PsA. Therefore, individuals diagnosed with psoriasis before the age of 30 years,; and those diagnosed after the age of 50 years were compared using Fischer’s exact test, and a logistic regression model was applied to control for sex and time since diagnosis of psoriasis. In these analyses, individuals diagnosed with psoriasis between the ages of 30 and 50 years were excluded. Since using the age of 30 years as the cut-off was an arbitrary choice, similar analyses were performed, in which psoriasis diagnosed before the age of 20 years was used as the cut-off instead. Finally, these analyses were then repeated using logistic regression with data from the entire study group and treating age as a continuous variable. Analyses were performed using SAS v9.4 (SAS Institute Inc., Cary, NC, USA) and STATA v13.0 (StataCorp, College Station, TX, USA).
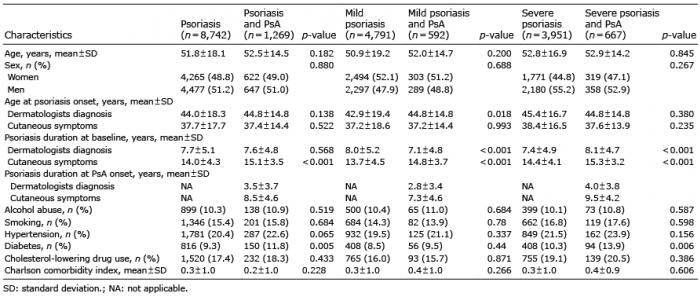
A total of 10,011 patients with psoriasis were included in these analyses (4,618 with severe disease). Of the total, 1,269 (12.7%) were diagnosed with both psoriasis and PsA (Table I). All patients (100%) had received topical treatment. Patients with psoriasis with and without PsA were of similar age, had a longer duration of psoriasis, but a comparable male-to-female ratio as those with psoriasis without PsA.
Table I. Demographics and characteristics of patients with psoriasis with or without psoriatic arthritis (PsA)
Fig. 1 shows the incidence and prevalence of PsA associated with time since psoriasis diagnosis (p for trend = 0.6593) and since first cutaneous symptoms (p for trend = 0.0001), respectively. Stratified analyses (time since diagnosis) by disease severity showed no significant trend (p = 0.4936) for those with mild disease, but a significant trend for those with severe psoriasis (p = 0.0002). Moreover, analyses of time since the first cutaneous symptoms showed that the trend was significant across severities (both p < 0.0001).
Fig. 1. Incidence and cumulative prevalence of psoriatic arthritis (PsA) over time in the population of psoriasis patients. (A) Percentage of patients with psoriasis who develop PsA per annum (years since psoriasis diagnosis). (B) Percentage of patients with psoriasis who develop PsA per annum (years since first cutaneous symptoms). (C) Cumulative percentage of patients with psoriasis who develop PsA (years since psoriasis diagnosis). (D) Cumulative percentage of patients with psoriasis who develop PsA (years since first cutaneous symptoms). Blue: any psoriasis; red: mild psoriasis; green: severe psoriasis.
Comparing patients with early onset of cutaneous psoriasis symptoms (before age 30 years, total: 3,471, mild: 1,932, severe: 1,539) with those with late onset (after age 50 years, n = 2,676; mild: 1,452, severe: 1,224) yielded a significantly higher PsA occurrence in early onset compared with late onset of any psoriasis (11.5% vs. 9.5%; p = 0.012), mild psoriasis (9.4% vs. 7.9%; p = 0.078) and severe psoriasis (14.1% vs. 11.2%; p = 0.030), respectively. Duration of cutaneous symptoms was slightly longer for those with early- vs. late-onset psoriasis (mean length of time with cutaneous symptoms: 13.9 ± 4.1 years vs. 13.6 ± 4.7 years; p = 0.0011). No significant difference in duration of cutaneous symptoms was found in early vs. late psoriasis in mild cases (mean 13.5 ± 4.4 years vs. 13.3 ± 4.8 years; p = 0.1561), but a significant difference was observed for severe disease (mean 14.5 ± 3.8 years vs. 13.9 ± 4.5 years; p = 0.0003). PsA risk was compared in those with early- vs. late-onset psoriasis (Table II), showing that early onset of psoriasis (age < 30 years) was insignificantly associated with a lower risk of PsA development when compared with those with late (age > 50 years) psoriasis onset (odds ratio (OR) 0.84; 95% confidence interval (CI) 0.71–1.00; p < 0.051). Conversely, when time of first cutaneous symptoms was used, rather than time of psoriasis diagnosis a slightly higher risk was shown (p = 0.018). No clear signal was observed with either diagnosis or cutaneous symptoms across severities (Table II). Psoriasis diagnosed before the age of 20 years (total: 1,011, mild: 704, severe: 307), was associated with a lower risk of PsA development (early- vs. late-onset psoriasis, OR 0.52; 95% CI 0.39–0.69, p < 0.001). Notably however, presence of cutaneous symptoms before the age of 20 years (total: 1,743, mild: 1,059, severe: 684) was not significantly associated with increased risk of PsA (OR 1.03; 95% CI 0.84–1.27, p = 0.777). PsA risk was not significantly different among those receiving systemic treatment (severe psoriasis) or among patients receiving topical therapy (Table II). When age at psoriasis diagnosis was treated as a continuous variable this did not predict the risk PsA (OR 1.00 for an additional year of age; 95% CI 1.00–1.00; p = 0.7613). Including patients diagnosed between the age of 20–50 years into the analysis did also not predict development of PsA (OR 1.00 for an additional year of age; 95% CI 1.00–1.00; p = 0.1597). Using a Poisson regression model, the IRR of PsA over time following onset of cutaneous symptoms was 1.03 (95% CI 1.02–1.05, p < 0.0001).
Table II. Logistic regression models assessing early (< 20a or < 30b years) vs. late (> 50 years) onset psoriasis and risk of psoriatic arthritis (PsA)
In this nationwide study of dermatologist-diagnosed patients with psoriasis, the incidence of PsA appeared to be stable with longer duration of psoriasis. Moreover, we observed no clear signal between age at psoriasis diagnosis or onset of cutaneous symptoms, and future development of PsA. Duration of cutaneous symptoms was significantly associated with risk of PsA in a Poisson regression model.
To date, very few studies have examined the association between psoriasis duration and risk of PsA. Christophers et al. (10) examined 1,560 patients with psoriasis, including 126 with PsA, seen in dermatology clinics across the UK, Italy, France, Spain and Germany, respectively. While the study found a growing prevalence of PsA of up to 20.5% with longer psoriasis disease duration, the authors reported that the incidence of PsA remained constant in any given year after the initial diagnosis of psoriasis. However, as indicated in their study discussion, the PsA diagnosis was made by dermatologists rather than by rheumatologists, which could have led to diagnostic uncertainty, and the study may also have suffered from bias in selection of study cases.
Speculative, prolonged exposure to systemic low-grade psoriatic inflammation could, at least in theory, affect PsA incidence among those with longer duration of psoriasis. Along this line, several observational studies have reported beneficial effects of anti-inflammatory agents, such as tumour necrosis factor (TNF) inhibitors, on cardiovascular comorbidities in patients with psoriasis (21) and other inflammatory diseases, such as rheumatoid arthritis (22), their impact on the effect of disease duration remains unclear. Since TNF inhibitors have proven efficacy, not only in psoriasis, but also in PsA, early and aggressive treatment of psoriasis symptoms with anti-TNF and other biological agents could potentially affect the development of overt symptoms of PsA. However, as with cardiovascular comorbidities where recent experimental studies have failed to replicate observational findings (23), our hypothesis remains to be tested in a clinical setting. It is currently being discussed whether early- and late-onset psoriasis are genetically distinct entities. Interestingly, the HLA-Cw*06 and HLA-DRB1*07 genes are associated with increased risk of PsA, especially in early-onset psoriasis (24).
Certain limitations apply to the interpretation of the present findings, the most important being that observational studies inherently cannot establish causality. We used systemic treatment as a measure of severe psoriasis. This method has previously been validated and is widely accepted in epidemiological psoriasis research (25). Nevertheless, we lacked important data on clinical measures of psoriasis severity, such as the Psoriasis Area and Severity Index, or the degree of affected body surface area, and our results should be interpreted accordingly. While the association between duration of cutaneous symptoms and risk of PsA seen in the Poisson regression model is intriguing, this finding warrants replication in other cohorts, and we emphasize that onset of psoriasis based on observational data is only an estimation. We found a lower risk among patients diagnosed <20 and <30 years, respectively, compared with those with late-onset (>50 years) psoriasis, yet the results for onset of cutaneous symptoms were conflicting in this regard, since the risk tended to be higher among those with early onset of cutaneous symptoms. Thus, based on the present findings we are unable to establish any firm conclusions regarding risk of PsA associated with age of psoriasis onset. We limited PsA diagnoses to those made by rheumatologists, in order to ensure diagnostic accuracy; however, this may have led to a selection of patients with more severe disease. Important strengths of our study include the completeness and accuracy of the Danish nationwide registries with minimal loss to follow-up, the ascertainment of diagnoses by dermatologists and rheumatologist, respectively, and the high number of included patients.
In conclusion, our data suggested that the PsA incidence remains stable with longer duration of psoriasis. Conflicting data were found with regards to PsA risk associated with age of psoriasis onset. There remains a lack of data in this area, and further studies are warranted to assess the effect of age of psoriasis onset on the risk of future development of PsA.
Declaration of interests: AE has received research funding from Pfizer and Eli Lilly, and honoraria as consultant and/or speaker from Pfizer, Eli Lilly, Novartis, Galderma, and Janssen Pharmaceuticals. LS has received consultancy and/or speaker honoraria from Abbvie, Pfizer, Janssen-Cilag, Eli Lilly, and Leo Pharma and is a member of the advisory boards of Abbvie, Pfizer, Janssen-Cilag, Almirall, Eli Lilly, Celgene, Leo Pharma and Novartis. CZ has served as a scientific consultant for Abbvie, Pfizer, Janssen-Cilag, Merck & Co., Inc., Eli Lilly, Takeda and Novartis and clinical study investigator for AbbVie, Amgen, Eli Lilly, Merck & Co., Inc., Takeda, Almirall and Novartis. GHG is supported by an unrestricted research scholarship from the Novo Nordisk Foundation. JPT is supported by an unrestricted grant from the Lundbeck Foundation and has received speaker honoraria from Galderma and MEDA and attended an advisory board meeting for Roche. LM is currently employed by Eli Lilly and Company.
Funding sources: Eli Lilly and Co. The funding sources participated in interpretation of the final analysed study results, but had no access to the raw data, and did not participate in data collection, management, or analysis.


 Click to show fullsize
Click to show fullsize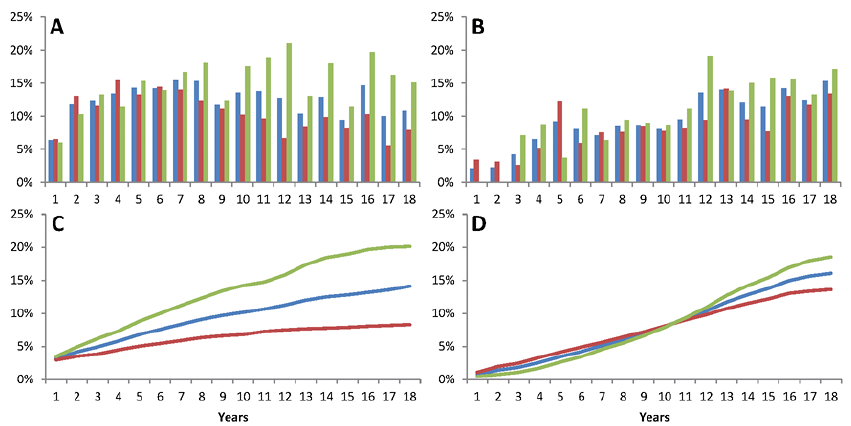 Click to show fullsize
Click to show fullsize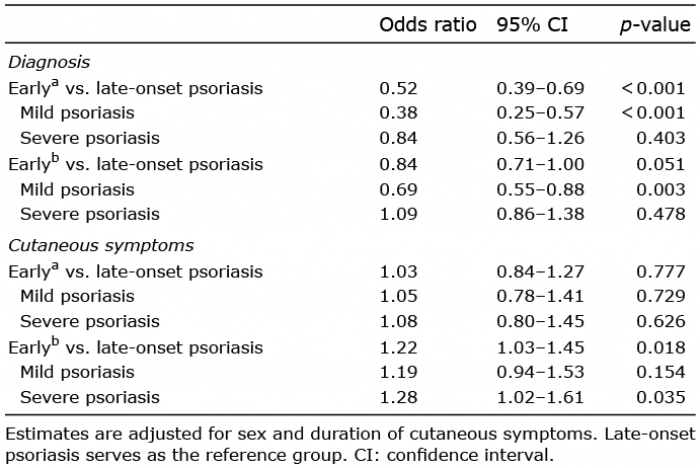 Click to show fullsize
Click to show fullsize