


Department of Dermatology B-1-Q, Leiden University Medical Center, Leiden, The Netherlands
Approximately 10% of all melanomas occur in subjects with a family history of melanoma. This retrospective follow-up study investigated the characteristics of patients with familial melanoma who made unscheduled visits to our pigmented lesions clinic, and the diagnosis of excised lesions. A total of 110 (9%) out of 1,267 patients made at least one unscheduled visit between May 2011 and February 2016. Histopathology was taken from 59 patients. Thirty-four naevi, 7 melanomas and 3 basal cell carcinomas were detected. All patients with melanoma were CDKN2A carriers and all melanomas were discovered at a very early stage. In this patient population it appears to be safe to limit visits to once or twice yearly, provided patients are easily able to make an unscheduled extra visit if they have a worrisome lesion. We recommend supporting patients’ self-reliance by stimulating them to carry out self-examination of their skin.
This study investigated if patients with a high risk for melanoma who visited a pigmented lesion clinic at least once per year also returned for unscheduled visits and we report on the lesions that were found. Nine percent of the patients came for an unscheduled visit and 7 early melanomas were found in carriers of a high risk mutation for melanoma.
In this population it is safe to limit regular visits to once or twice yearly, as long as patients get instructions for skin self-examination and have readily access to pay an extra visit when they have a worrisome lesion.
Key words: familial atypical multiple mole melanoma; p16; CDKN2A; melanoma; skin self-examination; unscheduled visit.
Acta Derm Venereol 2018; XX: XX–XX.
Accepted Mar 15, 2018; Epub ahead of print Mar 15, 2018
Corr: Nicole A. Kukutsch, Department of Dermatology B-1-Q, Leiden University Medical Center, PO Box 9600, 2300 ZA Leiden, The Netherlands. E-mail: N.A.Kukutsch@lumc.nl
Familial aggregation of melanomas is reported to occur in approximately 5–10% of all melanomas (1). In up to 40% of these families a mutation is present in the high penetrance melanoma susceptibility gene CDKN2A (2). In the Netherlands, the most prevalent CDKN2A germline mutation is a specific founder mutation (c.225-243del19), known as the p16-Leiden mutation (3). The second known mutation is found on the CDK4 gene on chromosome 12, which occurs in approximately 3% of melanoma families (4). Reports on the mean age of diagnosis of the first melanoma in these families range from 33–36 years in patients with CDKN2A gene mutation, to 41–45 years in patients without a CDKN2A gene mutation (with an unknown mutation) (2, 5, 6). In patients with a CDKN2A mutation the lifetime risk for developing melanoma is 70% at the age of 80 years, with a 30% chance of developing multiple melanomas (5, 7).
The Leiden University Medical Center is a tertiary referral centre for (familial) melanoma, where the first surveillance programme for familial melanoma was initiated in 1981. Family members at high risk of developing melanoma visit the pigmented lesions clinic (PLC) for a total skin examination at least once a year.
It is not known what proportion of patients return for an unscheduled visit and what the characteristics of these patients are. Moreover, it is not known if these visits lead to the discovery of melanomas. To investigate these questions, patients’ characteristics and pathology outcomes for high-risk family members who paid at least one interval visit during the period of the study were analysed. It was hypothesized that younger patients and those who were carriers of a gene mutation would return for an unscheduled visit more often. In addition, it was hypothesized that most patients would present with a lesion on the front of the body, due to its visibility.
This retrospective study investigated the clinical and histological characteristics of patients who had paid one or more unscheduled visit to the PLC of the Department of Dermatolog, Leiden University Medical Centre (LUMC), Leiden, the Netherlands, over a 5-year period.
Patients at high risk of developing melanoma visit the PLC for a total skin examination at least once a year. Like all other patients who visit the PLC they repeatedly receive information and practical tips on how to perform adequate skin self-examination, including instructions on how to use 2 mirrors to examine their back, or to ask their partner to assist with the skin check. Patients are also instructed to make unscheduled visits whenever they are worried about a particular lesion.
The study period was May 2011 to February 2016 and, during this period, patients were routinely scheduled once a year. Eligible patients were 12 years old and over and had an indication for screening at this clinic: they carried a CDKN2A or CDK4 mutation; had 25% and 50% chance of being a CDKN2A/CDK4 carrier, or were part of a family with an unknown mutation (defined as 3 melanoma cases in a family in which no CDKN2A/CDK4 mutation was found). Patients were included in the study when they attended the clinic for an unscheduled visit, made at the request of the patient, in between annual visits. Patients were excluded if the reason for their visit was unrelated to pigmented lesions. Digital medical charts were used to obtain information on the age and sex of patients, gene mutation status, the reason for the interval visit, and histology reports if an excision was performed after the interval visit.
Descriptive statistics were performed using IBM SPSS Statistics 23.
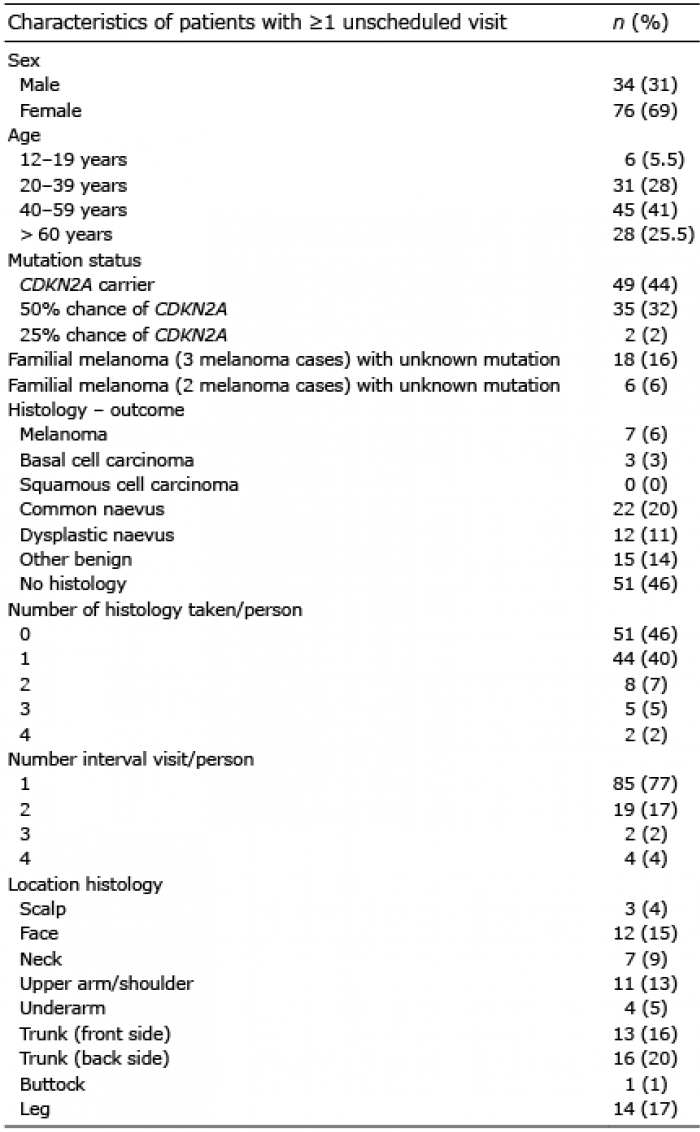
During the study period 1,267 patients visited the PLC at the LUMC at least once a year for a scheduled follow-up. Of these, 544 patients (43%) were male, with a mean age of 39 years (range 1–86 years) and 110 patients (9%) paid at least one unscheduled visit, of whom 34% were male with a mean age of 45 years (range 13–78 years) (Table I). The majority (77%) made only one unscheduled visit. Of 59 patients, histology was most often taken from the trunk (front and back) and the leg. Of these 59 patients 22 carried a CDKN2A mutation, 22 had a 50% chance of being a CDKN2A mutation carrier, 7 were carriers of an unknown mutation, 6 had familial melanoma (2 melanoma cases) with unknown mutation, and 2 had a 25% chance of being a CDKN2A carrier.
Table I. Characteristics of patients with unscheduled visits
A melanoma was found in 7 patients; one in situ melanoma and 6 invasive. Table II shows the characteristics of patients who were diagnosed with a melanoma at the unscheduled visit. Three patients were male, ages ranged from 37 to 67 years. All 7 patients were CDKN2A-mutation carriers, and all have had at least one cutaneous melanoma in the past. All melanomas were indicated by the patients.
Table II. Characteristics of patients/lesions with melanoma outcome (histology taken during unscheduled visit)
This study analysed the characteristics of patients with familial melanoma who returned for an unscheduled visit. Women made more unscheduled visits than men, which could be because they are more likely to visit the doctor earlier when they are worried. Furthermore, women perform skin self-examination more frequently or more accurately than men and therefore discover changing lesions earlier. Mesters et al. (8) found that 59% of patients who performed adequate skin self-examination were female. In the current study the most patients were between 40 and 59 years of age. This might be explained by the assumption that younger people are busier in general and have less time to perform a thorough self-examination or schedule an appointment. On the other hand, patients with hereditary melanomas are more likely to be diagnosed with their first melanoma at an earlier age and, for this reason, they may be more cautious and alert (9). A possible explanation for people over 60 years of age in the current study being less frequent visitors might be that this group was relatively small.
During unscheduled visits histopathology was taken most frequently from patients with a 50% chance of being a CDKN2A-mutation carrier or from proven CDKN2A-mutation carriers. This may be due to doctors being extra alert and cautious when there is a higher a priori chance of a melanoma, or to these patients being extra cautious themselves and insisting on excision, or to a combination of both.
A surprising finding of our study was that most pathology was taken from the back. Because of the difficulty of examining the back, compared with the legs or the front of the body, we expected this to be the area that patients examined the least. However, repeated extensive skin self-examination instruction might be the reason why lesions on the back were presented frequently during an unscheduled visit. The value of adequate instruction for finding melanoma at an early stage has been shown by many studies (10–17).
At our PLC there was a 12% chance of having a melanoma diagnosed during an unscheduled visit when histology was taken. All patients with melanoma during an unscheduled visit (Table II) had had at least one melanoma in the past and indicated the melanoma themselves. The previous melanoma might have made them more alert to recognize a suspicious lesion.
All melanomas found on unscheduled visits were thin melanomas, which is in agreement with other studies (18–20). Whether this is a result of improved surveillance or biological factors, such as the higher proportion of slow-growing superficial spreading melanoma in this population, or a combination of both, is not known. In an earlier study we found that tumour thickness did not correlate with the length of the screening interval for intervals less than 24 months. However, non-compliance with screening resulted in significantly thicker melanomas with a potentially worse outcome (7). Worldwide, members of melanoma families are offered much more frequent screenings, of up to 4 times a year. In a recent review screening frequencies ranging from every 3 to 12 months were advised with higher frequencies for individuals with high numbers of atypical naevi (21). Until recently (January 2016) we offered regular screenings to all members of melanoma families only once a year. Despite less frequent screening the mean Breslow thickness of melanoma in our patients with hereditary melanomas was approximately 0.5 mm, which is comparable to the results found with more frequent screening elsewhere (22, 23). This is probably the case because, from the beginning of our PLC in 1981, we have invested a lot of effort in instruction for skin self-examination and have offered patients unlimited and quickly scheduled appointments to return earlier in case of worrisome skin lesions.
This study has some limitations. The detailed characteristics of patients paying an unscheduled visit were examined. Ideally, this group would have been compared with the total population with familial melanoma in our PLC who did not pay an interval visit. This would also have enabled us to compare the proportion of screen melanomas with the proportion of melanomas found at unscheduled visits. In a retrospective study we found that only approximately half of all melanomas were detected at regular screening appointments (7). Other limitations were the low number of melanoma events in the study period and the fact that no information was available about lesions that were not excised.
Of the whole familial melanoma population of our PLC, 9% paid at least one unscheduled visit during the 5-year study period. Most patients were from CDKN2A-mutation-positive families, with only very early stage melanomas found during these unscheduled visits. We highly recommend encouraging patients with familial melanoma to perform skin self-examination and to initiate unscheduled visits if they are worried about a lesion.
The authors would like to thank Mrs M. A. Etty for technical assistance with collecting the PLC data.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize