


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Chalubinskiego 1, PL-50-368, Wroclaw, Poland. E-mail: ola.batycka@interia.pl
Accepted Mar 27, 2018; Epub ahead of print Mar 27, 2018
Psoriasis is a common, chronic, immune-mediated inflammatory disease with increased risk of cardiovascular disease and metabolic disturbances (1).
The receptor for advanced glycation end products (RAGE) is a multi-ligand, pattern recognition receptor, a member of the immunoglobulin superfamily. It has the ability to engage diverse classes of ligands, including S100 proteins and advanced glycation end products. RAGE-ligand interactions have been shown to amplify and perpetuate the chronic immune-mediated inflammatory process by sustained activation of transcription factor kappa beta (NF-κβ). RAGE-mediated signalling triggers expression of adhesion molecules, proinflammatory cytokines (e.g. tumour necrosis factor alpha (TNF-α), interleukin (IL)-1, -6, and -8) and recruitment of inflammatory cells to the site of inflammation (2, 3). Furthermore, the activation of RAGE appears to have a central role in accelerating atherosclerosis (2, 4, 5). The potential of the RAGE-ligand axis as a target of future therapeutic intervention has been proposed (2, 4–7). The full-length form of RAGE (fl-RAGE) is a transmembrane receptor. Soluble RAGE (sRAGE) is a truncated form of RAGE, lacking the transmembrane and cytoplasmic domains. sRAGE is derived predominantly from proteolytic cleavage of fl-RAGE. sRAGE acts as an extracellular decoy receptor, antagonizing fl-RAGE by binding its ligands without mediation of any cellular activity (2–4). Therefore, it is postulated that sRAGE has protective properties in chronic inflammatory diseases and atherosclerosis (2, 3, 4, 8). Low sRAGE levels have been found in atherosclerosis, cardiovascular disease, vascular complications of diabetes and in some chronic immune-mediated disorders, such as rheumatoid arthritis. A decreased sRAGE level has been proposed as a marker for chronic inflammation and atherosclerosis (2, 3, 4, 8–10).
The objective of the present study was to determine, for the first time, levels of sRAGE in individuals with chronic plaque psoriasis. The associations between sRAGE levels, severity of psoriasis, levels of C-reactive protein (CRP) and some clinical data have been evaluated.
The study was conducted on a group of 65 consecutive patients with chronic plaque psoriasis, aged from 18 to 76 years. A total of 35 healthy volunteers, matched by age and sex, randomly selected, with no history of psoriasis served as controls. Subjects with psoriasis did not receive any systemic therapy and phototherapy at least 4 weeks prior to initiation of the study and have never been treated with biologics. Severity of skin disease was assessed with the Psoriasis Area and Severity Index (PASI) by a single, experienced dermatologist. Exclusion criteria included: cardiovascular disease (defined as history of coronary artery disease, myocardial infarction, stroke, peripheral artery disease), chronic renal or liver disease, diabetes mellitus, malignancies and infectious diseases. Patients with psoriatic arthritis, diagnosed according to the ClASsification criteria for Psoriatic ARthritis (CASPAR), were excluded from the study. Information regarding the presence of traditional cardiovascular risk factors (e.g. arterial hypertension (HA), obesity, dyslipidaemia, smoking habit) and medication use were documented (Table SI). The study was approved by the local Bioethical Committee according to the principles of the Declaration of Helsinki.
The serum concentration of sRAGE was quantified using enzyme-linked immunosorbent assay kits (Human RAGE ELISA kit, Abcam, catalogue number ab100632, Cambrige, UK). All procedures were performed according to the manufacturer’s instructions. Quantitative analysis of sRAGE concentration was performed using the Epoch spectrophotometer (BioTek Instruments, Winooski, VT, USA). Assessment of serum CRP was done using a turbidimetric assay on an Architect ci4100 analyser (Abbott Diagnostics, Lake Forest, IL, USA).
Statistical analysis was performed using the software (Statistica version 12.0, StatSoft and GraphPad Prism version 5.0). Further details are shown in Appendix S1. Statistical significance was set at p < 0.05.
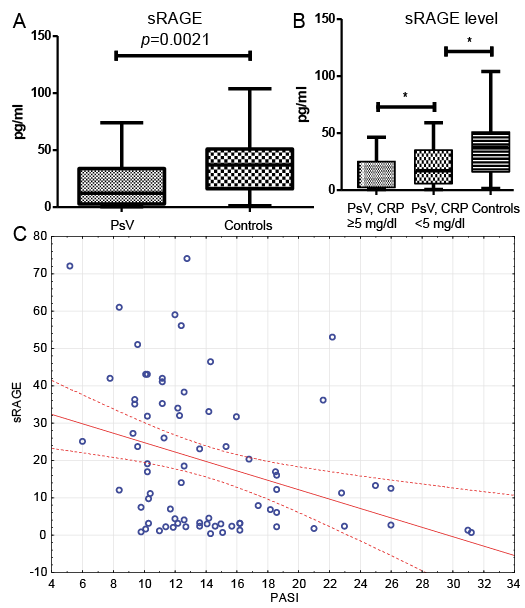
Serum levels of sRAGE were significantly decreased in individuals with psoriasis compared with controls (mean ± SD 19.43 ± 19.26 vs. 35.84 ± 26.66 pg/ml, p = 0.0021) (Fig. 1A). There were no statistically significant differences regarding incidence of HA, dyslipidaemia, smoking, obesity and use of hypotensive or lipid-lowering medications between psoriatic patients and controls. ROC analysis showed an area under the curve (AUC) of 0.68. The optimal cut-off value was 19.0 pg/ml with negative and positive predictive values of 0.464 and 0.836, respectively. Serum sRAGE levels were inversely correlated with PASI (p = 0.001, R= –0.37) (Fig. 1C). This association was independent of other variables. However, sRAGE levels were significantly lower in individuals with psoriasis with elevated CRP levels (≥ 5 mg/dl) than in individuals with psoriasis with CRP within the normal range (≤ 5 mg/dl) and controls (p = 0.019 and p = 0.0003, respectively) (Fig. 1B). No significant difference in sRAGE levels was found after dividing psoriatic patients according to the presence of HA, obesity, smoking, dyslipidaemia, or sex (Table SII).
Fig. 1. (A) Decreased levels of soluble receptor for advanced glycation end products (sRAGE) in patients with psoriasis and (B) with elevated C-reactive protein (CRP) levels compared with psoriatic patients with CRP within normal range (≤ 5 mg/dl) and controls (p = 0.019 and p = 0.0003, respectively). (C) Serum sRAGE products levels were inversely correlated with Psoriasis Area and Severity Index (PASI) (p = 0.001, R = –0.37). PsV: psoriasis vulgaris (chronic plaque psoriasis).
The present study demonstrated significantly lower serum levels of sRAGE in individuals with chronic plaque psoriasis compared with controls. fl-RAGE mediates the activity of several important mediators of inflammation in psoriasis, including S100A8 (calgranulin A), S100A9 (calgranulin B) and S100A12 (calgranulin C) (2, 3, 11, 12). Elevated serum levels of S100A8, S100A9 and S100A12, correlated with the severity of skin involvement, have been found in patients with psoriasis (11, 12). sRAGE acts as a decoy receptor and antagonizes fl-RAGE-mediated signalling. Recombinant sRAGE has been shown to be effective in inhibiting RAGE-mediated signalling in animal models. Administration of recombinant sRAGE had a strong protective effect and suppressed the chronic inflammatory response and atherosclerosis. It has been suggested that recombinant sRAGE may be beneficial in clinical settings (2, 3, 6, 7). The decreased levels of sRAGE found in the present study may indicate deficient inflammatory control and could be a basis for future therapeutic intervention for psoriasis and its cardiovascular comorbidities.
There is a need to search for a biomarker that will be of value to identify psoriatic patients with chronic systemic inflammation who are at increased cardiovascular risk. Low sRAGE level was proposed as a marker for chronic inflammation. Inverse associations between levels of sRAGE and CRP were found in some studies (3, 4, 9). In the present study, we observed significantly decreased sRAGE levels in patients with psoriasis, inversely associated with the severity of skin involvement. Furthermore, sRAGE levels were significantly lower in psoriatic patients with increased CRP levels compared with patients with CRP within the normal range and controls. The results of the present study suggest that low sRAGE levels may be considered as a biomarker for disease severity and the chronic inflammatory state in patients with psoriasis. Furthermore, numerous studies have demonstrated inverse associations between sRAGE levels and measures of atherosclerosis (4, 10).
To the best of our knowledge, this is the first study demonstrating decreased sRAGE levels in patients with chronic plaque psoriasis. Decreased levels of sRAGE may contribute to the chronic inflammatory process and atherosclerosis. Furthermore, sRAGE level may be considered as a biomarker for disease severity and chronic inflammatory state in patients with psoriasis. Recombinant sRAGE could be considered as a future therapeutic strategy for patients with psoriasis and cardiovascular comorbidities. However, further studies are required to assess its clinical value.


 Click to show fullsize
Click to show fullsize