


Department of Dermatology, University of Rzeszow, PL-35-055 Rzeszow, Poland. *E-mail: adi_medicalis@go2.pl
We describe here 2 patients with disseminated telangiectasias who were seen recently in our unit. The same condition was diagnosed in both individuals.
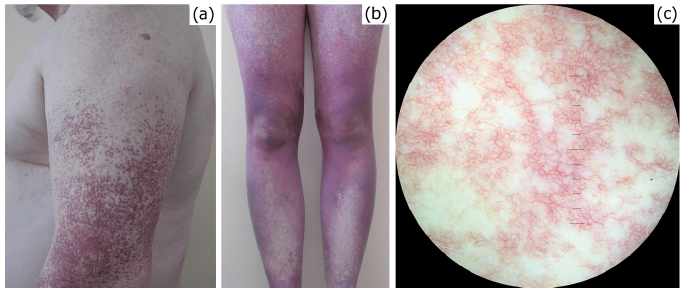
The first case was a 66-year-old man with telangiectasias that had developed when he was 44 years old. The skin lesions were initially located symmetrically on his lower limbs, but over time were slowly progressing towards his upper limbs (Fig. 1a). His face and neck were spared and only singular lesions were noticeable on the chest. On physical examination, the patient demonstrated widespread, symmetrically distributed tree-like branching telangiectasias. Neither oral mucous membrane involvement nor nail plate abnormalities were observed. The patient did not report any additional symptoms.
The second case was a 33-year-old woman with similar skin lesion morphology and pattern, but with more extensive involvement than in the first case. She had symmetrically disseminated telangiectasias, which formed confluent violaceous patches on her lower limbs, buttocks, trunk and arms (Fig. 1b). She first developed skin changes in her late teens. Dermoscopically, the lesions revealed straight and serpentine abundant telangiectatic vessels following a tree-like branched pattern (Fig. 1c). Similarly to the first case, no lesions were observed on her oral mucosa or nail plates. She had no history of abnormal bleeding, and was not diagnosed with any other systemic disorder.
Histological examination of skin biopsies showed almost identical features in both cases. Thickening of the walls of the multiple superficial dermal blood vessels containing hyaline material was identified by Periodic acid-Schiff (PAS) staining (Fig. 2a) and trichrome staining (Fig. 2b).
What is your diagnosis? See next page for answer.
Fig. 1. Clinical presentation of the condition in: (a) the male patient; and (b and c) the female patient. (a) Erythematous, mottled, telangiectatic macules extensively involving the extremities. (b) Diffuse telangiectasias on the lower limbs coalescent into purple-blue patches. (c) Dermoscopic appearance of the forearm telangiectasia: straight and serpentine vessels following a tree-like branched pattern (x10).
Fig. 2. Histological changes in the biopsy specimens obtained from: (a) the male patient; and (b) the female patient. Dilated thickened small blood vessels in the superficial dermal plexus (Periodic acid-Schiff, ×200). (b) Similar histological changes as in (a), using a different staining method (trichrome, ×200).
Acta Derm Venereol 2018; XX: XX–XX.
Diagnosis: Cutaneous collagenous vasculopathy
Cutaneous collagenous vasculopathy (CCV) is a recently described rare entity characterized by idiopathic acquired disseminated telangiectasias. CCV was first described in the literature in 2000 by Salama & Rosenthal (1). To date, fewer than 40 cases of this idiopathic microangiopathy of the superficial dermal blood vessels have been published (2). CCV is more common among middle-aged women, with a median age of diagnosis of 63.5 years. Some authors emphasize that this entity is highly under-recognized; the slow progression of skin lesions and no additional symptoms may contribute to late diagnosis. As calculated by Bondier et al., the median time delay from onset to diagnosis of CCV is 7 years (2).
The aetiology of CCV is unknown, although there is some speculation concerning the genetic defects that alter the production of collagen and certain environmental factors, such as skin trauma (2). Despite genetic factors being taken into consideration in pathogenesis of CCV, neither a familial history nor an autosomal dominant pattern of inheritance has been observed (3). Based on histology results, it has been hypothesized that intravascular obstruction resulting from local thrombosis might be a primary event in CCV (3). As the most common comorbidities of patients with CCV are arterial hypertension (reported in more than 40% of patients with CCV) and diabetes mellitus (found in almost 30% of patients with CCV), it is possible that microangio-pathy related to those conditions might also contribute to the origin of CCV (2, 4, 5).
The clinical picture of CCV is characterized by dilated capillary blood vessels arranged in branch-like shapes. CCV spreads progressively from distal parts of the lower limbs towards the trunk and upper limbs. In most cases, skin lesions spare the face, mucous membranes and nails. No additional symptoms accompany the abnormal cutaneous findings. Moreover, no systemic abnormalities are connected with this disorder. The diagnosis is based on histological testing. Typically, it shows dilated superficial cutaneous vessels with marked collagen deposition of PAS-positive material (6).
The most important disorders clinically presenting as generalized telangiectasia, that in many cases morphologically do not significantly differ from CCV, are generalized essential telangiectasia (GET), hereditary haemorrhagic telangiectasia (HHT) and hereditary benign telangiectasia. GET is clinically almost indistinguishable from CCV and these 2 entities can only be differentiated by histology. In GET, in contrary to CCV, the dilated superficial skin capillaries have normal wall thickness. Moreover, immunohistochemistry with type IV collagen antibody, showing the material deposited around the blood vessel basement membrane, is helpful in differentiating CCV from other disorders that involve the development of idiopathic telangiectasias (7). Patients with HHT are easily distinguishable from those with CCV, as they manifest severe systemic symptoms resulting from arteriovenous malformations that lead to bleeding from the lungs, liver or gastrointestinal tract (8). CCV is commonly mistaken for generalized essential telangiectasia or pigmented purpuric dermatosis. In addition, CCV is likely to be misdiagnosed as other unrelated entities, e.g. connective tissue diseases with vascular component, cutaneous mastocytosis or ataxia-telangiectasia.
CCV is currently considered a rare, yet under-recognized and underreported, cause of generalized telangiectasias. Physicians should therefore obtain biopsies in such patients to ensure adequate diagnosis and proper prognosis. In most of the described cases no treatment for CCV was introduced, as the course of the disease is usually benign, with telangiectasias being asymptomatic and confined to the skin. As with other telangiectatic diseases, pulsed dye laser (PDL) has been incorporated successfully in the treatment of CCV (9). However, the extent of the disease makes complete lesion clearance virtually impossible in the majority of cases.


 Click to show fullsize
Click to show fullsize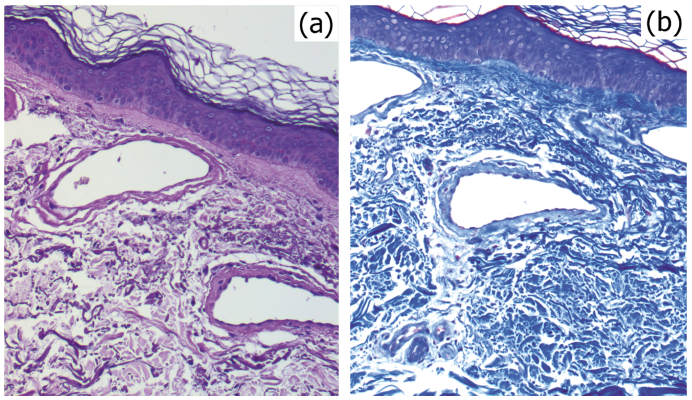 Click to show fullsize
Click to show fullsize