


1University of Texas McGovern Medical School at Houston, 2ADG Pathology, 2525 West Bellfort, Suite 194, 3Departments of Dermatology and Head & Neck Surgery, MD Anderson Cancer Center, and 4Department of Dermatology, University of Texas McGovern Medical School at Houston, 6655 Travis St, Ste 980, Houston 77030, TX, USA. *E-mail: Sirunya.Silapunt@uth.tmc.edu
Accepted May 29, 2018; Epub ahead of print Jun 1, 2018
Nodular hidradenomas (NH) are benign tumors that arise from eccrine adnexal structures. NH are commonly located on the head, neck, and anterior trunk, with lower extremities being an atypical site (1, 2). NH exacerbation in pregnancy is rare and raises possibility of cytological changes occurring secondary to hormonal fluctuations.
A 36-year-old Hispanic woman, gravida 6 para 6, at 31 weeks gestation of pregnancy presented with a tender nodule on her right lower leg that was stable for 2 years but enlarged during pregnancy. There was no significant past medical history or trauma to the area.
Physical examination of the right medial lower leg revealed a well demarcated, dome-shaped light brown nodule measuring 10 × 15 mm (Fig. 1). There was no regional lymphadenopathy and systemic examination was unremarkable. We considered a wide differential diagnosis, including arteriovenous malformation, connective tissue neoplasms, adnexal tumors, skin cancers, and cutaneous metastatic tumors.
Fig. 1. A well-demarcated border, dome-shaped, light brown nodule measuring 10 x 15 mm on the right lower leg.
A punch biopsy was performed. Histopathologic evaluation showed a well-circumscribed solid-cystic dermal tumor consisting of a solid sheet-like arrangement of eosinophilic, polyhedral and clear cells. The tubular and cystic structures are filled with homogeneous eosinophilic material. Atypia, invasion, necrosis, and mitoses are not observed (Figs. 2–3). Immunohistochemical studies showed tumor cells positive for cytokeratin 7 (CK7) and epithelial membrane antigen (EMA), and negative for renal cell carcinoma marker (RCC), paired box gene 8 (PAX8), carcino-embryonic antigen (CEA), and CD10. Tumor cells were also diffusely positive by periodic acid schiff (PAS) stain. These findings were consistent with nodular hidradenoma.
Fig. 2. The well-circumscribed dermal tumor consists of a solid sheet-like arrangement, containing eosinophilic, polygonal or fusiform cells, cystic spaces, and some cellular differentiation (Hematoxylin and eosin, 4x).
Fig. 3. The hidradenoma cells are large and polyhedral with distinct cell borders, containing round to ovoid nuclei, evenly distributed nuclear chromatin, and pale to eosinophilic cytoplasm. Tubular lamina formed by cuboidal cells are present. Hidradenoma produces mucin, which stains red with PAS stain, 20x.
Due to its benign nature, surgical removal was postponed until after delivery when the tumor was excised with a 3 mm margin.
NH are benign tumors that arise from eccrine adnexal structures. NH was first described by Liu in 1949 as clear cell papillary carcinoma of the skin, and has been termed clear cell hidradenoma, eccrine acrospiroma, and solid-cystic hidradenoma (3).
NH has a female predominance (1.7:1) with a mean age of 37.2 years (4). NH presents as a single, small, slow-growing, well-demarcated, intra-dermal tumor that varies in size from 5–30 mm. The overlying skin varies in color, with a smooth, thickened, atrophic, or ulcerated surface (1). It is common on the head, neck, and anterior trunk, and infrequent in the lower extremities (1, 2).
Our case involved an atypical location on the leg. In a 10-year review of 89 NH cases, 4 were located on the legs (4.49%) (4). The unusual location and exacerbation during pregnancy prompted our report of this case. Pregnancy is known to increase eccrine activity with exception of at the palms. This may lead to miliaria, hyperhidrosis, and dyshidrotic eczema (5). Our case suggests that pregnancy can contribute to the growth of eccrine sweat apparatus tumors, but this relationship has not been elucidated.
NH may be asymptomatic or may present with pain, or bleeding, and rarely can show malignant transformation (6). Diagnosis is made by histopathology. NH presents as a well-circumscribed dermal nodule surrounded by a collagenous pseudocapsule, occasionally extending into subcutaneous tissue (1, 7). The tumor is comprised of multiple lobulated masses of epithelial cells and tubular lamina (1, 7). Several different cell types are seen, including large polyhedral eosinophilic cells and fusiform cells, as well as columnar, cuboidal, squamous, and intermediate cells. Duct-like structures and cystic cavities are commonly found as is collagenous, hyalinized, and mucinous stroma (1). Dermoscopy shows a nodule of amorphous, white-pink areas, red lacuna-like areas, eccentric ulceration, as well as hairpin, dotted, and linear irregular vessels (8). Due to the variation in different cell types, histopathologic differential diagnosis is extensive, including apocrine mixed tumor, eccrine poroma, thyroid carcinoma, renal cell carcinoma, metastatic tumor, neuroendocrine carcinoma, hidradenocarcinoma, and glomus tumor.
Due to high recurrence rate, biopsy and surgical excision are warranted with follow-up to monitor for recurrence as malignant transformation has been known to occur (1). Our patient had an uncomplicated post-operative course with no evidence of recurrence at 12 months follow-up.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize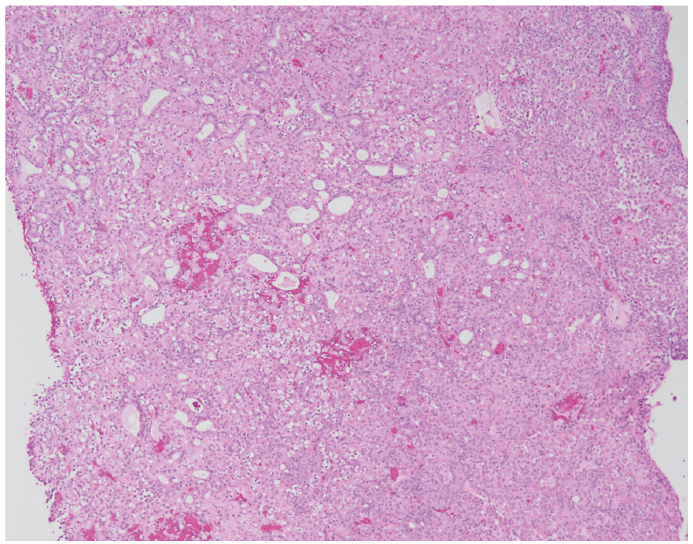 Click to show fullsize
Click to show fullsize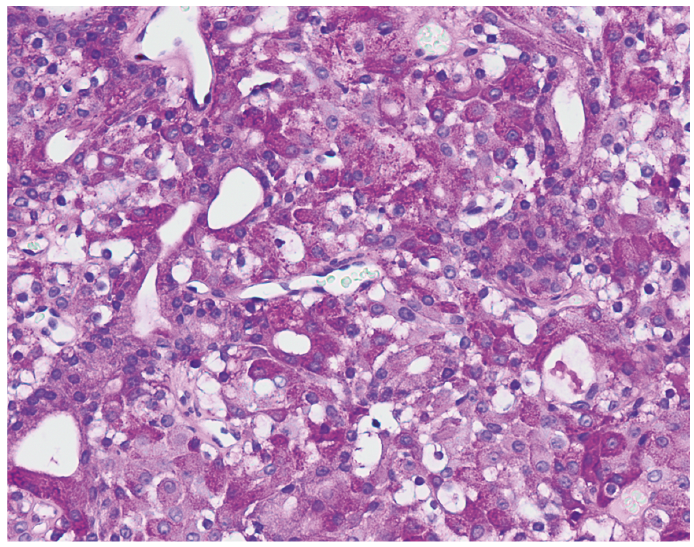 Click to show fullsize
Click to show fullsize