


1Section of Dermatology, Department of Medical Science and Public Health, 2Department of Life and Environmental Sciences, and 3Section of Pathology, Department of Surgery, University of Cagliari, IT-09124, Italy. *E-mail: ramonazanniello@gmail.com
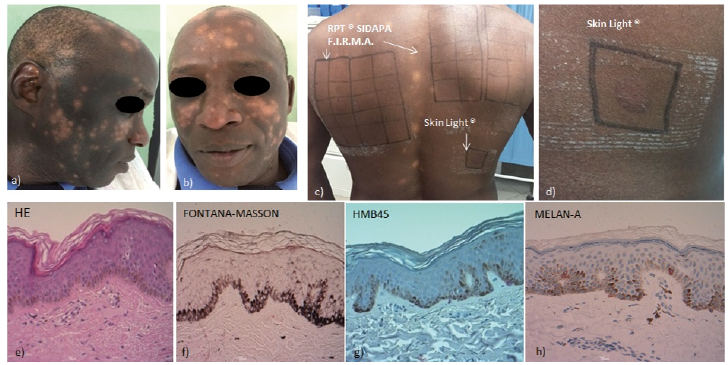
A 47-year-old African man was referred to our clinic for multiple, rapidly progressive, hypopigmented lesions, which first occurred on his face and later on his scalp and trunk. Dermatological examination showed whitish patches, either isolated in a confetti-like pattern, or confluent in larger hypopigmented areas with ill-defined margins (Fig. 1a, b). Examination under Wood’s lamp and direct microscopy for possible fungal infection were both negative. Otherwise healthy, the patient had no personal or family history of vitiligo and autoimmune diseases. Three days prior to onset of the hypopigmentation, he had begun application to his face of a “carrot extract and vitamin E cream”, a bleaching cream, named Skin Light® (RODIS, Abidjan, Ivory Coast), which he had bought in an ethnic shop in Italy, It was the first-time the patient had used this specific product, but he had used other bleaching creams previously, with no complaints or skin reaction. The patient was precise about the name and composition of these cosmetics. He also reported a mild itching sensation and redness during first application of Skin Light®, but only the appearance of the pigmentation disorder led him to seek a dermatological consultation. In order to determine the composition of the cream, we conducted chemical and physical analysis in our university laboratory, including liquid chromatography and mass spectrometry. A biopsy was taken from the patient’s neck in order to investigate the type of pigmentation disorder. Patch tests were performed with the baseline series recommended by the Società Italiana Dermatologia Allergologica Professionale ed Ambientale (SIDAPA) using Rapid Patch Test (RPT®, F.I.R.M.A. SpA, Florence, Italy) and the commercial cream “as it is”, with an additional reading on day 4. A positive patch-test reaction developed exclusively to the cream (Fig. 1c, d). Vitiligo was excluded by histological examination, showing non-specific findings: mild orthohyperkeratosis (Fig. 1e), normally pigmented epidermal basal keratinocytes with Fontana-Masson stain (Fig. 1f), and uniform distribution of melanocytes on immunohistochemistry (HMB-45; Melan-A) (Fig. 1g, h).
What is your diagnosis? See next page for answer.
Fig. 1. (a, b) Hypopigmented patches on the face and scalp (c, d) Patch test on day 4 with reaction only to the cream, (e) Histopathological imaging of a punch biopsy from the hypopigmented skin of the neck showed mild orthohyperkeratosis (×20 haematoxylin and eosin; H&E), (f) basal pigmented keratinocytes in the epidermis (×20 Fontana-Masson stain). (g, h) Immunohistochemical studies for HMB-45 and Melan-A demonstrated melanocytes distributed in a uniform pattern. Written permission to publish these photographs has been provided by the patient.
Acta Derm Venereol 2018; XX: XX–XX.
Diagnosis: Hydroquinone confetti-like depigmentation
The diagnosis of hydroquinone confetti-like depigmentation was supported by chemical analysis of the cream, which revealed the presence of 3% hydroquinone, excluding other toxic chemicals, such as mercury. The skin-lightening product was stopped immediately, but at 2-month follow-up no consistent repigmentation had occurred. Topical tacrolimus 0.1% ointment twice daily was started with poor improvement, as well as oral supplementation with antioxidants, melanin precursors and vitamin D, which was found deficient (25.2 ng/ml; normal range 40–100 ng/ml). A second biopsy was performed with superimposable results. After one year the lesions persist almost unchanged. The practice of skin bleaching has aesthetic, sociological, political and economic motivations, especially for people from Asian and African countries (1). Light skin tone is associated with beauty, elegance and higher social rank (1, 2). Hydroquinone is one of the most popular skin-lightening agents, banned from the market by the European Union (EU) Cosmetic Regulation 1223/2009 (3), because of severe local and systemic side-effects (2). Our patient developed spotting depigmentation, extending to sites quite distant from the location of application of the cosmetic cream. Fisher firstly described 4 cases of acquired disfiguring leukoderma following application of a 2% hydroquinone cream (4), and an allergic contact dermatitis was reported to cause leukomelanoderma in subjects professionally exposed to hydroquinone derivate (5). Positive patch-test reaction for the cream supported contact dermatitis with eventual post-inflammatory hypopigmentation. In addition, the timing of the cream application in our case is very short, and suggests possible previous exposure to hydroquinone. The patient reported having used other creams previously and having had a mild local reaction during application of the culprit cream. The histological findings were disappointing, excluding signs of contact dermatitis, and demonstrating the presence of melanocytes in basal layers with special stains. A second biopsy was performed, including areas of hypopigmentation. No information was available on the functional state of melanocytes, but post-inflammatory hypopigmentation or functional injury to the melanocytes damaged by the cream should have recovered after discontinuation of application of the cream and neo-melanin genesis oral supplementation. Mechanisms of hydroquinone toxicity on melanocytes remain unclear, as do treatment recommendations. The atypical presentation in our patient, whose pathogenic mechanisms remain unclear, supports the need for careful monitoring and eventual new biopsy to check that no other diagnosis becomes evident. Marketing of illegal agents not declared in the labelling, manufactured in developing countries, such as Ivory Coast, is a global issue, and vigilance measures need to be increased. In order to understand the pathogenesis and find suitable therapeutic agents, it is necessary to alert the medical community and promote patient education about the risks of artificial depigmentation.


 Click to show fullsize
Click to show fullsize