


Departments of 1Dermatology and 2Cellular Pathology, Norfolk and Norwich University Hospital, Colney Lane, Norwich NR4 7UY, 3Public Health England National Cancer Registration and Analysis Service, Fulbourn, Cambridge, UK, and 4Department of Medicine, University of Malaya, Faculty of Medicine, Unit of Dermatology, Kuala Lumpur, West Malaysia. E-mail: peter.goon@nhs.net
Accepted Jun 26, 2018 Epub ahead of print Jun 29, 2018
Eccrine porocarcinoma (EPC) was first described by Pinkus & Mehregan in 1963 (1) as “epidermotropic eccrine carcinoma” and is the malignant counterpart of eccrine poroma. It is a rare tumour (0.005–0.01% (2, 3) of cutaneous tumours), thought to arise from the acrosyringium of the sweat gland of the skin. The term “porocarcinoma” was first used by Mishima & Morioka in 1969 (4). Although initial case series suggested that this was a highly aggressive tumour, with approximately 60% of cases reported to have local recurrence, metastases or death, later larger case series of 18, 24 and 27 patients, respectively, did not support such an aggressive natural history (3, 5, 6)
The largest case series to date (69 cases) in 2001 (7), reported EPC as a less aggressive tumour, with 17% local recurrence, 19% lymph node metastasis and 11% distant metastases or death.
This study analysed the age-standardised incidence rates for the population of the East of England (East Norfolk and Waveney), and estimated the numbers of cases likely to be found here and in the UK for 2020, 2025 and 2030. This cohort (n = 152) is the largest reported so far and there are long-term follow-up data for recurrences, metastases and survival/death, thus helping to clarify the natural history of this tumour.
Electronic databases from the pathology department at the Norfolk and Norwich University Hospital (NNUH) from East Norfolk and Waveney (ENW): (Breckland, Broadland, Great Yarmouth, North Norfolk, Norwich, South Norfolk and Waveney community districts) in the Eastern Region of the UK (population: 794,043 in 2004 increasing to 870,100 in 2013) (8–11), were analysed and collected from the 1st of January, 2004 to 31st December 2013 for this retrospective cohort analyses.
Skin cancer histology results from each hospital in the region are coded and recorded monthly by the International Classification of Diseases categories ICD10/ICDO-2.
There have been no changes in catchment area for the pathology laboratory or change in practice protocols or routines for the pa-thologists and laboratory involved for the period of study. There have been no changes in physician patterns of referral of lesions over the study period. Standard immunohistochemical stains for markers known to be helpful in diagnosis of EPC such as epithelial membrane antigen (EMA), carcino-embryonic antigen (CEA), CD117 (KIT), etc, have been used as required or as available. Specialist dermatopathologists in the NNUH led the routine analyses of skin specimens. All porocarcinoma in situ samples were excluded from analyses. Only patients with verified survival and recurrence data were included in the study.
Statistical analyses were performed using statistics package GraphPad™ Prism 7 (2016).
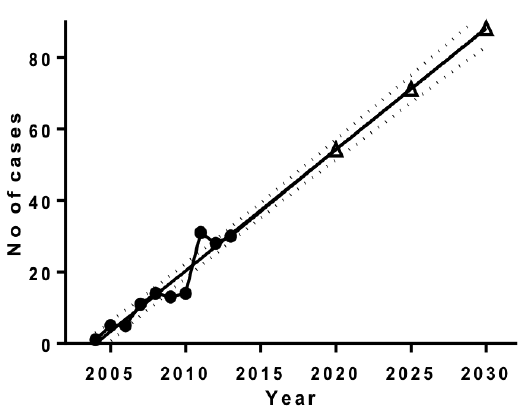
Over the 10-year study period stated above, the population of ENW increased by approximately 10.4% at a steady rate (8–11). Our recorded data for the numbers of EPC from the study period are shown in Fig. 1. Based on these data, linear regression analyses estimate numbers of cases for the years 2,020 (n = 54), 2,025 (n = 71) and 2,030 (n = 88).
The East of England has a higher number of the elderly (> 65 years of age), Caucasians (White) and more sunshine per annum by comparison with the UK mean. The technique of approximation to the means (8–10) controlled for these risk factors and extrapolated regional ENW data to UK levels, this allowed estimation of the national incidence in future years.
The predicted total number of cases of EPC for the whole of the UK was 2,979 in 2020, 3,873 in 2025 and 4,746 in 2030. [These figures are calculated estimates only, and the risk of error increases the further away the estimate is made (see Fig. 1)].
Fig. 1. Number of cases of eccrine porocarcinoma diagnosed in East Norfolk and Waveney, with predicted cases in 2020, 2025 and 2030. Total no. of cases per year were 1, 5, 5, 11, 14, 13, 14, 31, 28, 30 for the data points shown below from 2004–2013.
The Age-Standardised Incidence (ASI) Rates for EPC in males, females and the total population of the East of England was calculated using the European Standard Population 2013 (Table SI). This allowed comparison of these incidence rates with that of other published data so far. The ASI for males was 2.414 per 100,000, the ASI for females was 1.344 per 100,000 and the Total ASI was 1.866 per 100,000. These data showed that the incidence of diagnosed EPC in the East of England has increased rapidly over the 10-year study period. The rates of EPC are very high at the end of the study period, > 30-fold higher than that published for skin adnexal tumours as a whole in Holland (12), or nearly 10-fold higher than for Minnesota in the US (13).
Long-term follow-up data for these patients showed that the rates for metastases and recurrences are 16.45% and disease-specific deaths (DSD) were 7.89% (males: 6, and females: 6). Combined rates for total metastases/recurrences (males: 16, females: 9) and DSD would be 17.11%. These rates are not dissimilar to those reported by Robson et al. 2001 (7).
EPC is a rare malignancy originating from the acrosyringium of the sweat gland. Early studies reported that the tumour was highly aggressive with 60% rates of recurrences, metastases or death. This study presents possibly the largest cohort of patients with EPC (n = 152) over a 10-year period, and therefore might show slightly more accurate analyses of natural history.
These data show that although EPC appears to be a more aggressive tumour than squamous cell carcinoma (SCC) of the skin (mortality ~1%) on a per case basis, the mortality rate of nearly 8% is not as high as that initially reported by smaller case series.
We have previously shown that there has been a rapid rise in the UK incidence of non-melanoma skin cancers such as basal cell carcinomas, SCCs, and Merkel cell carcinoma (8–10). These data demonstrate that EPC incidence is also rising rapidly. The data show that EPC is a cancer of the elderly, with a median age of 82 in males, 86.5 in females, a male to female ratio of 1.7:1 and the highest ASIs are in the over 85s in both sexes.
The reasons for the rapid rise in incidence rates are unclear. It is likely that contributory factors include an increased efficiency and accuracy in histological diagnosis with better histological discrimination of EPC from poorly defined SCC of skin. The use of specific immunostains reported to be useful in the diagnosis of EPC such as CEA, EMA, PAS staining for glycogen, and CD117 may also be a contributory factor. Historical less efficient registration practices may also play a part. This study identified a much higher incidence rate at the end of the study period than available US or European data. In addition to diagnostic factors, genetic factors and the rise in sun-seeking holidays taken by the largely pale skinned UK population over the last 30–40 years may also be contributory.
In conclusion, we show that (i) EPC diagnosis, al-though rare, has been rising in the East of England, and has risen rapidly over the last 10 years, possibly due to histological diagnostic factors, and more precise registration together with a possible real increase in incidence; (ii) The EPC ASIs are much higher than the scanty data available from other Western countries, and it is likely that the incidence is also high in the rest of the UK; (iii) EPC is a more aggressive tumour compared to SCC of the skin but the metastases and mortality rates are not as high as early reports suggested.


 Click to show fullsize
Click to show fullsize