


1Department of Dermatology, and 2Department of Clinical Laboratory Medicine, Kyoto University Graduate School of Medicine, 54 Shogoin-Kawahara, Sakyo, Kyoto 606-8507, Japan. *E-mail: kaba@kuhp.kyoto-u.ac.jp
Accepted Jul 5, 2018; Epub ahead of print Jul 6, 2018
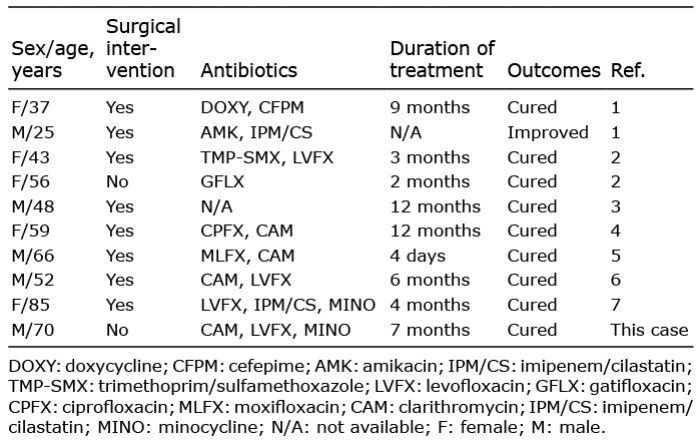
Mycobacterium mageritense is a recently identified rapidly growing uncommon mycobacteria (RGM) (1). Only 9 cases of skin and soft-tissue infection with M. mageritense have been reported to date (1–7) (Table I). Although accurate identification of the pathogenic bacteria is mandatory for efficient treatment, using conventional methods for the identification of M. mageritense is complex and time-consuming. We report here a case of subcutaneous infection with M. mageritense that was treated successfully with antibiotics, in which matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS) (8) enabled rapid identification of the species.
Table I. Summary of 9 cases of skin and soft tissue infection with M. mageritense reported
A 70-year-old Japanese man developed subcutaneous abscesses in the periumbilical region within 2 weeks after a laparoscopic cholecystectomy. After unsuccessful treatments with antibiotics (cefamezin and vancomycin) and immunosuppressive agents (prednisolone and azathioprine) for 1 year, he was referred to our hospital. On examination, a total of 80 reddish nodules intermittently excreting pus were observed on the abdomen (Fig. 1a). Histopathologically, the dermis and subcutaneous adipose tissue were prominently infiltrated with neutrophils (Fig. 1b, c). An acid-fast bacillus culture grown from the excreted pus at 37°C for 3 days revealed a Mycobacterium species. It was identified as M. mageritense using MALDI TOF-MS system (Microflex LT and MALDI Biotyper, Bruker Daltonics GmbH) with a score value of 2.26 according to the MycoEx extraction protocol (v.3.0) and Mycobacteria Library 4.0. In addition, full-length sequencing of the 16S rRNA gene confirmed this finding. Based on these results, the patient was given a diagnosis of subcutaneous infection with M. mageritense.
Fig. 1. Clinical pictures and histopathology. (a) A clinical picture before the treatment, showing reddish nodules on the abdomen. Arrow: scar from the laparoscopic cholecystectomy contiguous to the umbilicus. Histopathology: (b) low-magnification view showing a prominent infiltration of neutrophils in the deep dermis and subcutaneous adipose tissue. (c) High-magnification view of the rectangle in (b). (d) A clinical picture after treatment with antibiotics, showing post-inflammatory pigmentation.
In advance of the species identification and drug-susceptibility tests, we empirically administered clarithromycin (800 mg/day), levofloxacin (500 mg/day) and minocycline (200 mg/day). After initiation of these antibiotics, no new lesions emerged and the pre-existing eruptions began to subside. Following the species identification, clarithromycin was stopped because M. mageritense is known for its resistance to macrolides (1). Consistently, drug-susceptibility tests later revealed that the isolate was sensitive to levofloxacin and minocycline and resistant to clarithromycin. Within 9 months after the initiation of the antibiotics, all of the subcutaneous indurations had diminished, leaving post-inflammatory pigmentation (Fig. 1d). After antibiotics were stopped, no recurrence was observed in 9 months of follow-up.
The standard treatment for non-tuberculous mycobacterial infections is a combination of antibiotics (9). The selection of antibiotics is usually based on drug susceptibility tests, yet the correlation between in vitro drug susceptibilities and in vivo treatment outcomes can be ambiguous for RGM infections (10). M. mageritense is known for its resistance to macrolides, which are often used for RGM infections; thus, an accurate identification of the bacterial species is mandatory for effective treatment of infections (1).
In general, the species within Mycobacteria are identified using PCR-based and/or DNA-DNA hybridization-based methods in a clinical laboratory (11). However, M. mageritense is not identifiable using commercially available kits; and the more robust identification methods (PCR restriction enzyme analysis, 16S rRNA gene sequencing, and high-performance liquid chromatography) are complicated and time-consuming, delaying the selection and administration of appropriate antibiotics. Recently, MALDI-TOF MS has been widely used for species identification, in which a colony is picked from a culture plate and is directly submitted to the analysis chamber after drying (8). Since the analysis processes of MALDI-TOF MS itself takes only a few seconds, MALDI-TOF MS enabled us to identify M. mageritense in a day from the initiation of the examination, providing a theoretical basis for the selection and long-term administration of antibiotics. This patient’s broadly distributed lesions were successfully treated using only antibiotics, although a surgical resection of remaining lesions is often required for the treatment of skin or subcutaneous tissue infections with M. mageritense (Table I). In addition, because of the paucity of evidence for the identification of the minor NTM, M. mageritense, by MALDI-TOF MS, we corroborated the result by the most robust method of full-length sequencing of the 16S rRNA. Further accumulation of data might certificate MALDI-TOF MS as a stand-alone method for the identification of M. mageritense.
This report describes the clinical course of a case of subcutaneous infection with M. mageritense showing a broad distribution of abscesses. MALDI-TOF MS enabled the efficient identification of M. mageritense and thus its effective treatment with a combination of antibiotics.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize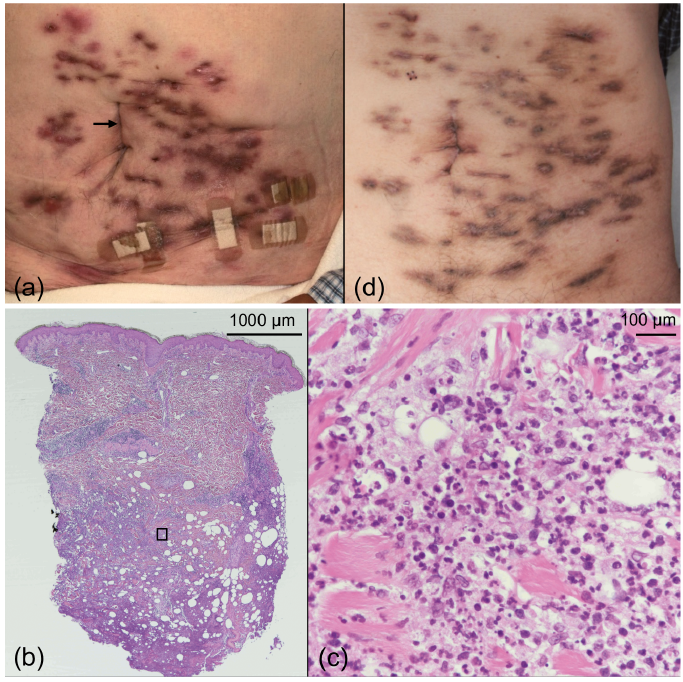 Click to show fullsize
Click to show fullsize