


1Department of Dermatology, 2Unit of Infectious Diseases, and 3Pulmonary Institute, Rabin Medical Center – Beilinson Hospital, Petach Tikva 4941492, and 4Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel. *E-mail: levp@clalit.org.il
Accepted Jul 27, 2018; Epub ahead of print Aug 7, 2018
Biologic therapies pose a risk of opportunistic infection, especially of reactivating latent tuberculosis infection (LTBI). Therefore, screening for LTBI is mandatory prior to commencing biologic treatment (1). Traditionally, the tuberculin skin test (TST) is used for LTBI screening, but its specificity is low, leading to unnecessary antibiotic treatment (2). Since 2001, researchers have developed ex vivo assays measuring interferon-gamma (IFN-γ) production by T cells exposed to specific mycobacterial antigens: T-SPOT.TB, QuantiFERON TB Gold (QFT) and QFT in tube. As IFN-γ-releasing assays (IGRAs) have high specificity, they are recommended as the screening method of choice by the British Association of Dermatologists (3). Nonetheless, because of their high cost, IGRAs are frequently used only as confirmatory tests in patients with an initial positive TST result (4). However, the agreement between these tests is poor, and the question of the need for chemoprophylaxis in patients with discordant results remains unresolved (4, 5).
This real-life study aimed to determine the prevalence of TST positivity in patients with psoriasis prior to the initiation of biologic therapy, and the safety of biologics without chemoprophylaxis in patients with discordant results.
This study was approved by the ethics committee of Rabin Medical Center. A retrospective cohort study design was used. The database of a tertiary dermatology department was searched for all consecutive patients treated with biologics for moderate-severe psoriasis since 2005. Prior to treatment, patients were screened for LTBI with chest X-ray (CXR) and TST, with or without the QFT. Patients paid for the QFT out-of-pocket until 2016, when the health insurance funds categorized it as reimbursable if TST was positive. TST was considered positive if the induration measured ≥ 5 mm at 48–72 h. QFT was considered positive when the IFN-γ response was ≥ 0.35 IU/ml (manufacturer’s instructions). Patients were evaluated every 2–3 months until follow-up ended and for successive TST screening annually. Chemoprophylaxis with isoniazid (300 mg daily; 9 months) or rifampicin (600 mg daily; 4 months) was administered under the following conditions: (i) TST ≥ 5 mm and unavailable QFT; (ii) positive QFT; or (iii) abnormal CXR. The www.bcgatlas.gov website was used to assign BCG status in each patient’s country of origin (6). Countries with an annual incidence > 40 per 100,000 population were defined as endemic.
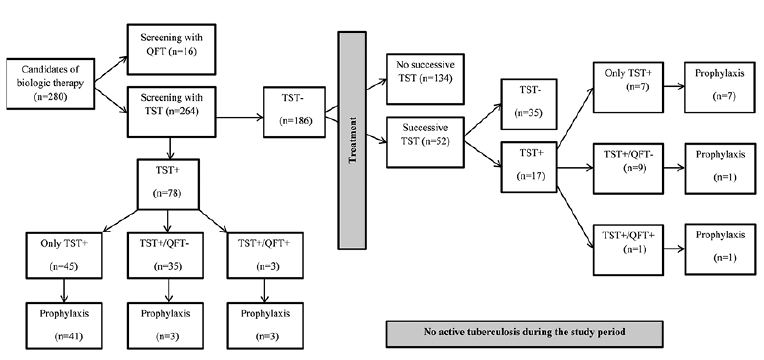
Of the 280 patients, 264 (94%) were screened with the TST. In 95 patients (36%), TST was positive either before or during treatment (Fig. 1). Table SI summarizes the clinical characteristics of the TST-positive patients. During a mean follow-up of 51 ± 40 months, none of the patients acquired active tuberculosis. The TST-positive patients included 53 men and 42 women of mean age 52 ± 14 years. Forty-eight patients (51%) were born when BCG vaccination was indicated at birth, and 35 (37%) were immigrants from endemic countries. None had a history of tuberculosis. A similar rate (50%) of BCG vaccination was found among the 169 TST-negative patients.
Fig. 1. Flow chart showing the distribution of tuberculin skin test (TST) results, QuantiFERON TB Gold (QFT) results, and chemoprophylaxis during the study period.
Screening data. Mean TST induration size was 12 ± 5 mm. TST was positive at baseline in 78/264 patients (30%) and negative in 186. Fifty-two patients with a negative TST result (28%) underwent successive screening during treatment; 17 (33%) experienced TST conversion. Of the total 95 TST-positive patients, 43 (45%) underwent confirmatory screening with the QFT (including 10 who underwent conversion) and 39 (90%) had a discordant result (TST+/QFT–). Four of them (10%) received chemoprophylaxis for the following reasons: TST induration of 18 and 30 mm (n = 2); equivocal CXR findings (n = 1); unclear indication (n = 1). The other 35 (81% of QFT-tested group) were safely treated with biologics without chemoprophylaxis (Table SII). For the remaining 52 TST-positive patients, QFT results were unavailable. Chemoprophylaxis was administered to 48, including all 8 patients (8% of the total cohort) with an abnormal CXR. The remaining 4 did not receive chemoprophylaxis because of an intermediate TST result (5 mm).
Biologic therapies. Etanercept was the most frequently used agent (83% of patients), followed by adalimumab (66%), ustekinumab (45%), secukinumab (15%), infliximab (11%), golimumab (2%), efalizumab (2%) and alefacept (1%). Patients received a mean ± SD of 2.3 ± 1.1 agents. The mean duration of treatment was 45 ± 31 months for the whole subgroup of TST-positive patients and 37 ± 30 months for the 35 patients with discordant tests who did not receive chemoprophylaxis.
This study was conducted in a population with a low tuberculosis burden. Although one-third of subjects had TST positivity before onset of biologic treatment, in most cases, a confirmatory QFT allowed for the safe administration of treatment without chemoprophylaxis.
Studies report a highly heterogeneous TST positivity rate in patients with psoriasis, ranging between 4.5% and 99% (7, 8). The present study was conducted in Israel, where the tuberculosis burden is low (4:100,000) (6). Nonetheless, a high rate of 30% of TST positivity was observed among 264 patients prior to initiation of biologic therapy. In addition, during the study period, TST converted to positive in 17/52 patients (33%) with an initial negative result who underwent successive TST screening. Previous studies have concluded that TST conversion is suggestive of reactivation (9). However, all 17 patients remained asymptomatic and had a normal CXR.
The major finding of our study is that, of the 43 TST-positive patients who were screened with confirmatory QFT (including 10 in whom TST converted), 35 (81%) had negative result and could be safely treated with biologics (over a mean of 37 months) without chemoprophylaxis. Importantly, most of these patients were considered to be at low risk of true LTBI on the basis of a normal CXR, no past active tuberculosis, and long-term residence in a country with a low tuberculosis burden. Nevertheless, approximately one-third were immigrants from endemic countries.
Similarly, Laffitte et al. (5), reported that screening with T-SPOT.TB (another IGRA), spared 10/12 patients with a TST-based diagnosis of LTBI from chemoprophylaxis. These findings suggest that low-risk patients with discordant results (TST+/IGRA–) might be safely treated with biologics without chemoprophylaxis. Possible reasons for the discrepancy between the TST and QFT include variability in performance and interpretation of the TST, reduced specificity of the TST following BCG vaccination, and exposure to non-tuberculosis mycobacteria and the Koebner phenomenon (2).
An important consideration is the rate of progression from LTBI to active tuberculosis during biologic therapy. A recent meta-analysis reported 0.57% incidence rate of active tuberculosis in patients receiving TNF-α antagonist, but the follow-up period in most of the studies was ≤ 30 weeks (10). In contrast, studies focusing specifically on patients with psoriasis who had positive LTBI screening reported reactivation rates of up to 3% (8). As most of these patients received chemoprophylaxis, the true reactivation rate without chemoprophylaxis may be much higher.
The current study was limited by the relatively small sample size. Large-scale studies are needed to consolidate our findings. Secondly, because of changing policies of QFT funding, only half of the TST-positive patients had available QFT. Finally, although successive screening was scheduled annually, patient compliance was low and screening intervals varied.
In conclusion, the present study suggests that even in populations with a low incidence of TB, a high proportion of psoriasis patients may be TST-positive at presentation or may convert to positive over time. Confirmatory screening with the QFT may allow for the safe administration of biologic therapy without chemoprophylaxis in those who are at low risk of tuberculosis.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize