


Departments of Dermatology, 1Aichi Medical University, 1-1 Yazako, Karimata, Nagakute, Aichi, 480-1195, 2Nagoya University Graduate School of Medicine, Aichi, and 3Graduate School of Medicine, Hokkaido University, Hokkaido, Japan. E-mails: yh_jp_hirot@yahoo.co.jp and makiyama@med.nagoya-u.ac.jp
Accepted Jul 27, 2018; Epub ahead of print Aug 7, 2018
Bullous pemphigoid (BP) is the most common autoimmune blistering disease that affects the skin and mucosae. Many cases of BP associated with oral intake of dipeptidyl peptidase-4 inhibitors (DPP4Is) have been reported recently (1–5). We report here a case of a woman with BP associated with DPP4Is. Interestingly, epitope spreading of anti-BP180 antibodies was observed when her disease recurred.
An 86-year-old woman visited our hospital with a complaint of general itching. She had been prescribed linagliptin, a DPP4I, for diabetes at a clinic. Blisters appeared on her lower limbs 6 weeks after initiation of oral linagliptin treatment, and the number of blisters gradually increased. At first, her attending physician suspected an allergic reaction to linagliptin. He changed the patient’s treatment from linagliptin to anagliptin, another DPP4I, but the blister formation continued. At the patient’s first visit to our hospital (defined as day 0), multiple blisters were seen scattered on both legs (Fig. 1a). A biopsy specimen from a bullous eruption on her right thigh showed a subepidermal blister with eosinophil infiltration (Fig. 1b). Direct immunofluorescence revealed linear deposition of IgG and complement component C3 at the dermoepidermal junction (Fig. 1c). In analyses of the patient’s serum, enzyme-linked immunosorbent assay (ELISA) for the non-collagenous 16A (NC16A) domain of BP180 was negative, but ELISA for full-length (FL) BP180 was positive. DPP4I-associated BP was suspected, and oral anagliptin was discontinued on day 10. After cessation of anagliptin, blister formation gradually diminished, and the patient’s anti-FL-BP180 antibody titres decreased immediately. On day 150, blister formation had stopped completely. Although itching and erythematous plaques on the extremities were seen intermittently, the symptoms were controlled with topical clobetasol propionate.
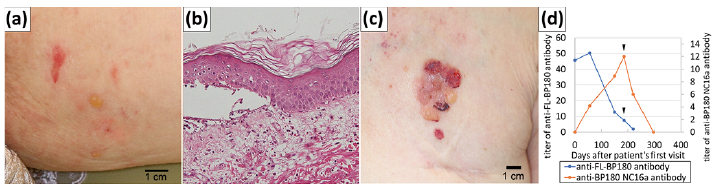
Fig. 1. Clinical and histopathological features and chronological changes in anti-BP180 antibody titres. (a) A clinical feature on the right thigh during the patient’s first visit to our hospital. Tense blisters and erosions were observed. (b) A biopsy specimen from the exanthema on the patient’s lower leg showed a subepidermal blister with eosinophil infiltration (haematoxylin-eosin, original magnification ×200). (c) Recurrent exanthema with blisters and erosions on the left chest. (d) Chronological changes in titres of anti-BP180 NC16A antibodies and anti-FL-BP180 antibodies in the patient’s serum. When BP recurred (black arrowheads), anti-BP180 NC16A antibodies became positive, and anti-FL-BP180 antibodies continued decreasing (day 185, 25 weeks after discontinuing DPP4I treatment).
On day 185, blisters relapsed bilaterally on the patient’s lower legs and trunk, although she had not taken any additional DPP4Is and continued using topical clobetasol propionate. At this time, ELISA for the NC16A domain of BP180 using the patient’s serum became positive, whereas the titres of her anti-FL-BP180 antibodies continued decreasing (Fig. 1d, Table I). Because the patient had hyperglycaemia, we prescribed oral low-dose prednisolone (7.5 mg/day) and minocycline. Blister formation stopped within one week, but itching and erythematous plaques on the extremities remained. We substituted mizoribine in place of minocycline, and her symptoms were gradually relieved. She became negative for anti-BP180 NC16A antibodies on day 220. She stopped treatment of her own volition on day 297. Her symptoms did not recur, and ELISA results for her serum have remained negative for both the NC16A domain of BP180 and FL BP180.
Table I. Titres of anti-BP180 antibodies in the patient’s serum during the disease course
In 2017, Benzaquen et al. (6) confirmed for the first time in a case-control study that DPP4Is are associated with an increased risk of developing BP in diabetic patients (adjusted odds ratio (OR) 2.64; 95% confidence interval (CI): 1.19–5.85; p = 0.02). Izumi et al. (7) also reported autoantibody profiles of patients with DPP4I-associated BP. They suggested that DPP4I-associated BP involves autoantibodies targeting the mid-portion of BP180, but not the NC16A domain. DPP4 is a cell-surface plasminogen receptor that is able to activate plasminogen to plasmin. Plasmin is a major serine protease that is known to cleave BP180 within the juxtamembranous extracellular non-collagenous 16A domain. Hence, the inhibition of plasmin production by DPP4I may change the proper cleavage of BP180, resulting in altered antigenicity and function of BP180.
The noteworthy aspect of the present case is that the epitope for the patient’s anti-BP180 antibodies spread from a region (or regions) outside the NC16A domain to the NC16A domain after the cessation of DPP4Is. After anagliptin was discontinued, the patient’s skin symptoms improved, and her titres of anti-FL-BP180 antibodies decreased immediately. Later, the disease recurred, and the patient’s serum became positive for anti-BP180 NC16A antibodies, but her titres of anti-FL-BP180 antibodies continued to decrease. We used a topical, high-potency steroid as the first-line treatment of BP in this case according to the latest recommendations (8, 9). However, the patient’s symptom was resistant to the treatment, and treatment with oral, low-dose prednisolone and mizoribine was necessary.
We speculated that the inflammatory reaction targeting the BP180 protein during the patient’s preceding DPP4I-associated BP induced the production of anti-BP180 NC16A antibodies, which are typically detected in the serum of patients with conventional BP (6). As mentioned above, the inhibition of plasmin production by DPP4I may change the proper cleavage of BP180. Thus, the cessation of oral DPP4I may lead to normalized cleavage of BP180 within the NC16A domain, and the NC16A domain may be exposed as an epitope for autoantibodies, as in patients with conventional BP. In the present case, we presumed that the co-existence of non-cleaved BP180 and cleaved BP180, together with the remaining antigen-antibody reaction to the mid-portion of BP180, induced alteration of the main epitopes from the mid-portion of BP180 to the NC16A domain of BP180 in the course of BP180 cleavage normalization after cessation of DPP4I.
To our knowledge, this article is the first case report to highlight the recurrence of DPP4I-associated BP accompanied by epitope spreading of anti-BP180 antibodies after the cessation of treatment with DPP4Is. In patients with DPP4I-associated BP, epitope spreading from domain(s) outside the NC16A domain to the NC16A domain of BP180 may occur even after cessation of the causative DPP4Is. Thus, routine monitoring of serum antibody titres is necessary for early detection of epitope spreading and disease recurrence.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize