


1Department of Dermatology and 7Pathology, Assistance Publique–Hôpitaux de Paris (APHP), Cochin Hospital, 2Paris Descartes University, 3Department of Head and Neck Surgery, 4Unité INSERM U932 and 8Department of Pathology, Institut Curie, 5PSL University, Paris, 6Department of Dermatology, CHU Reims, Robert Debré Hospital, Reims, 9Institut Cochin, Inserm U1016, 10Inserm UMRS938, Paris, 11EA 7319, and 12Reims Champagne-Ardennes University, Reims, France. *E-mail: sarah.guegan.bart@gmail.com
Accepted Aug 31, 2018; Epub ahead of print Sep 3, 2018
Melanoma treatment has improved considerably following the approval of immune checkpoint inhibitors and targeted therapy against BRAF and MEK (1, 2). In the melanoma tumour microenvironment, activated T cells can be functionally inactivated by engagement of the programmed-cell-death-receptor 1 (PD-1) with its ligands PD-L1 and PD-L2 expressed on tumour cells (3). Two monoclonal antibodies directed against PD-1 (nivolumab and pembrolizumab) have shown clinical efficacy in advanced melanoma (2, 4–7). Phase 3 trials have also demonstrated nivolumab and pembrolizumab superiority as adjuvant treatment in fully resected stage IIIB/C-IV melanoma (8, 9). But all trials centered on metastatic or locally advanced melanoma, and the efficacy of anti-PD-1 in non-metastatic primary melanoma has not been evaluated. We report herein 3 cases of patients with unresectable primary melanoma who achieved complete response after anti-PD-1 treatment.
Case 1. A 60-year-old man was diagnosed with an unresectable primary mucosal melanoma of the oral cavity invading mouth, soft palate, uvula, cavum (Fig. 1a). The tumour did not display any BRAF, NRAS, or CKIT mutation. PD-L1 expression was negative on tumour cells and intermediate on immune cells (Fig. S1a-c). Anti-PD-1 therapy was quickly initiated. After 4 pembrolizumab infusions, partial clinical response was noted with the pigmented area extending only to the soft palate and uvula. A punch biopsy of this persisting lesion (Fig. 1b) performed after 10 infusions of anti-PD-1 revealed an infiltrate of melanophages surrounded by lymphocytes with no tumour cells (Fig. S1d). The patient tolerated the medication well, but presented with asymptomatic hyperthyroidism (anti-thyroid antibodies were all negative). Pembrolizumab was discontinued 6 months after this histologically confirmed remission, and no relapse occurred (12 months of follow-up).
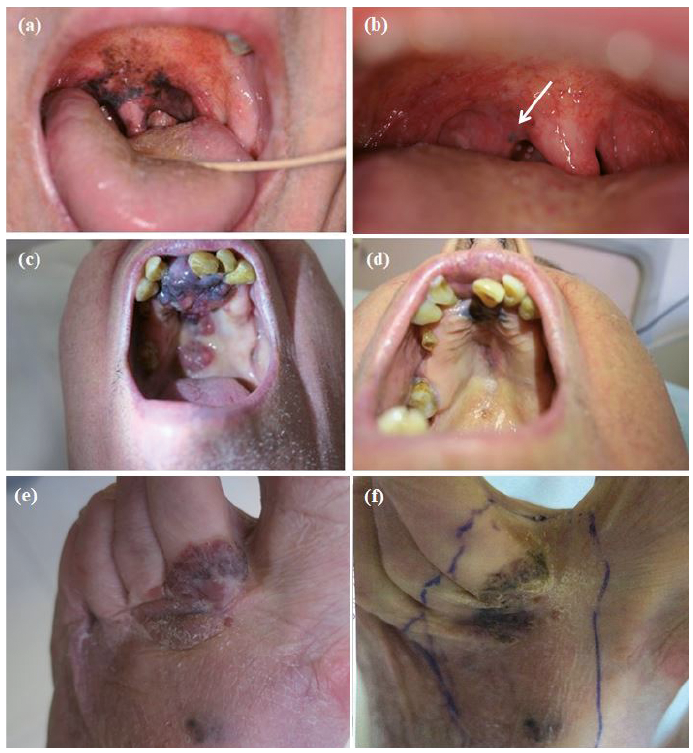
Fig. 1. Clinical features of melanoma before and after anti-programmed-cell-death-receptor 1 treatment. Patient 1: mucosal melanoma (a) before and (b) after 10 infusions of pembrolizumab. White arrow indicates a residual pigmented macule. Patient 2: mucosal melanoma (c) before and (d) after 12 infusions of pembrolizumab. Patient 3: superficial spreading melanoma (e) before and (f) after 3 infusions of nivolumab.
Case 2. An 89-year-old man was referred for a painful expanding lesion of the hard and soft palates (Fig. 1c), corresponding to a CKIT mutated mucosal melanoma (Fig. S1e), without metastatic disease on staging computing tomography (CT) scan and PET-scan. PD-L1 was highly expressed on tumour and immune cells (Fig S1f-g). Because of the limited efficacy of imatinib in CKIT mutated melanoma (10), anti-PD-1 therapy was initiated. After the third pembrolizumab course, the patient developed grade 2 polymyalgia rheumatica which quickly subsided with 0.5 mg/kg of oral corticotherapy. A significant reduction in tumour size was noted after the fourth pembrolizumab infusion. After the twelfth pembrolizumab infusion, 2 biopsies were performed on 2 residual lesions (Fig. 1d), and pathological analysis revealed a feature of complete regression with only melanophages and no tumour cells (Fig. S1h). Pembrolizumab was stopped after 13 anti-PD1 administrations. No relapse occurred (18 months of follow-up).
Case 3. An 85-year-old woman was diagnosed with an NRAS mutated superficial spreading melanoma (SSM) of the foot (Fig. 1e), with 3 peripheral pigmented cutaneous metastases on the foot dorsum and no distant metastasis. Wide amputation was refused by the patient. No PD-L1 marker was expressed on tumour cells or on immune cells (Fig. S1j, k). Nivolumab was initiated: the goal was to obtain a sufficient response to allow surgical resection without amputation. After 3 nivolumab infusions, the patient presented with rhabdomyolysis secondary to autoimmune related myositis. Nivolumab was discontinued, despite an early partial response of the foot melanoma. Two months after nivolumab discontinuation, the tumour size was significantly reduced (Fig. 1f); surgical resection of the 2 persisting pigmented areas with 10mm peripheral margins revealed a complete regression of the melanoma without residual tumour cell (Fig. S1l). Patient 3 died of rapid cerebral relapse 7 months after surgery. Total body CT scan had not revealed any other metastatic lesion.
This is the first case series of 3 patients with unresectable non-metastatic primary melanoma, including 2 mucosal melanomas, which responded to anti-PD-1 monotherapy with clinical as well as histologically proven remission. Of note, patient 3 underwent complete excision of the residual lesion, which confirmed complete regression of the primary melanoma. However, she developed cerebral metastases 7 months later. Indeed, in melanoma, complete regression and cure of the primary tumour does not always prevent visceral metastatic relapse.
Mucosal melanoma is usually resistant to traditional therapies (11). The anatomical location often precludes complete surgical resection because negative margins are difficult to achieve. Patients with mucosal melanoma infrequently harbor BRAF mutations, but mutations in the receptor tyrosine kinase KIT are common. Anti-tumour activity with KIT inhibitor has been observed, but was typically of short duration (10). Only 2 cases of metastatic mucosal melanoma with response to anti-PD-1 were reported (12, 13). Recently, a pooled analysis studying nivolumab alone or in combination with ipilimumab in metastatic mucosal or cutaneous melanoma, described lower median progression-free survival (PFS) in patients treated for mucosal melanoma (14). But there is no information about the efficacy of these treatments in unresectable non-metastatic primary melanoma.
Despite negative PD-L1 expression, patients 1 and 3 achieved complete remission after anti-PD-1 treatment. The use of PD-L1 biomarker in the therapeutic strategy for metastatic melanoma is controversial. In Larkin et al. (5), only patients with PD-L1 negative tumours had a significant improvement of PFS after treatment with nivolumab and ipilimumab versus nivolumab alone. But in a recent study including 430 different cancers and 8 melanomas, 25% of the melanomas expressed PD-L1, and PD-L1 expression did not affect the overall survival (15). This underlines the need for new biomarkers to elaborate an anti-PD-1 treatment strategy.
Anti-PD-1 monotherapy seems to be a good therapeutic option in unresectable non-metastatic primary melanomas, even in mucosal melanomas that are typically more resistant to this therapy, regardless of PD-L1 status. Adequate follow-up is mandatory, as visceral metastases may nevertheless occur in the course of evolution.
Conflicts of interest: CL: national congress attendance supported by BMS; NK: expert for Roche and BMS; NF: national and international congress attendance supported by Roche and BMS; SA: Boards for BMS; Florent Grange: Expert for MSD; SG: national and international congress attendance supported by Roche and BMS. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize