


1Department of Dermatology, Hospital del Mar-Parc de Salut Mar, Universitat Autònoma de Barcelona, 2Department of Statistics, Institut Hospital del Mar d’Investigacions Mèdiques (IMIM), Barcelona, Spain
Pink flat skin lesions on the legs in elderly people represent a diagnostic challenge due to the paucity of clinical and dermoscopic evidence. A prospective study of 114 pink flat lesions on the legs of 85 elderly patients was performed to describe the utility of reflectance confocal microscopy in this clinical context. Evaluation of clinical, dermoscopic and confocal parameters and calculation of diagnostic accuracy/sensitivity/specificity for non-melanoma skin cancer diagnosis of each technique were carried out. Thirty-four benign and 80 malignant neoplasms were analysed. A correct clinical diagnosis was establish-ed in 49.1% of cases (sensitivity 68.7%, specificity 73.5%). Dermoscopy achieved 59.6% correct diagnosis (sensitivity 85%, specificity 67.6%) and confocal microscopy evaluation after clinical and dermoscopic evaluation rendered a correct diagnosis in 85.1% of cases (sensitivity 97.5%, specificity 88.2%). Confocal microscopy may improve diagnostic accuracy, sensitivity and specificity as a secondary evaluation after dermoscopy. A diagnostic confocal algorithm for pink flat lesions on the legs is proposed.
Key words: dermoscopy; reflectance confocal microscopy; histopathology; basal cell carcinoma; Bowen’s disease; venous stasis dermatitis.
Accepted Aug 31, 2018; Epub ahead of print Sep 3, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Ignacio Gómez-Martín, Department of Dermatology, Hospital del Mar-Parc de Salut Mar. Universitat Autònoma de Barcelona, Passeig Marítim 25–29, ES-08003, Barcelona, Spain. E-mail: nachgm@gmail.com
Pink flat skin lesions on the legs represent a diagnostic challenge due to the paucity of specific clinical and dermo-scopic features. A prospective study of a series of 114 pink flat skin lesions on the legs in elderly people was performed to describe the utility of reflectance confocal micro-scopy (RCM) in this clinical context. RCM resulted in 85.1% diagnostic accuracy, 97.5% sensitivity and 88.2% specificity for non-melanoma skin cancer diagnosis. A diagnostic RCM algorithm for pink flat lesions on the legs is proposed. RCM, as a secondary evaluation after dermoscopy, may improve diagnostic accuracy, sensitivity and specificity and may avoid the need for invasive biopsies.
Pink flat skin lesions on the legs of elderly people exhibit a broad differential diagnosis (1, 2). They represent a diagnostic challenge due to the paucity of clinical and dermoscopic morphological clues, and the existence of varying degrees of associated xerosis, sun damage and venous stasis dermatitis. Pink flat skin lesions often present with non-specific overlapping clinical and dermoscopic features (3–11).
Furthermore, on dermoscopy, pink lesions on the lower limbs usually exhibit prominent, but non-specific, vasculature due to orthostatic blood pressure.
Differential diagnosis includes tumoural lesions (Bowen’s disease (BD), actinic keratosis (AK), invasive squamous cell carcinoma (SCC), basal cell carcinoma (BCC), amelanotic/hypomelanotic melanoma, seborrhoeic keratosis (SK), clear cell acanthoma, melanocytic naevus, angiomas, dermatofibroma, neurofibroma), inflammatory lesions (venous stasis dermatitis (VSD), lichen planus (LP), lichen planus-like keratosis (LPLK), porokeratosis, psoriasis, lichen aureus, lichen simplex chronicus) or infectious diseases (flat wart).
Dermoscopic algorithms used routinely for pigmented lesions are often not very helpful in the diagnosis of pink lesions. Several years ago, Giacomel & Zalaudek (12) suggested an algorithm for hypopigmented lesions based on vessel morphology, vascular architectural arrangement and additional criteria, and soon afterwards Zalaudek et al. (13) proposed including an initial clinical assessment and search for specific patterns. Rosendahl et al. (14) also described an algorithm for non-pigmented skin malignancies based on pattern analysis: first, looking for ulceration; secondly, for white clues; and thirdly, vessel analysis. However, these algorithms have not been tested in prospective studies for sensitivity, specificity or diagnostic accuracy.
In this particular clinical context, in which only scarce dermoscopic criteria are specific, reflectance confocal microscopy (RCM) may offer specific diagnostic criteria. RCM might achieve a confidence close to histopathology (gold standard) and may permit a decrease in the number of required biopsies, reducing costs and potential complications (pain, cellulitis and chronic ulcers).
The aim of the current study was to describe the utility of RCM in pink flat skin lesions on the legs in photodamaged skin, to characterize the dermoscopic and RCM criteria of the different skin conditions that present as pink lesions on the legs, and to correlate the RCM findings with the corresponding histopathological features.
Pink flat skin lesions on the legs in patients attending a referral unit in the Department of Dermatology, Hospital del Mar-Parc de Salut Marwere included prospectively between 1 January 2012 and 31 December 2016. The inclusion criteria used to recruit lesions to this study were: solitary pink flat lesions on the legs detected by clinical naked-eye examination with absent or less than 10% of pigmentation on dermoscopic evaluation. Only lesions for which skin cancer was suspected in the differential diagnosis were included in the study. Nodular lesions were excluded.
All patients gave written informed consent to be included in the study, which was approved by the ethics committee of our hospital.
Clinical and dermoscopic images of all lesions were obtained using a camera (PowerShot G10; Canon, Tokyo, Japan) attached to a contact polarized light dermoscopy device (DermLite Foto; 3Gen, San Juan Capistrano, CA, USA). No pressure was applied when taking image lesions, in order to preserve vessel morphology and ensure their better visualization. Dermoscopic images were evaluated blinded to histopathological diagnosis by one contributing author with > 10 years of experience in the field (S.M.). A total of 49 dermoscopic criteria described in the literature were analysed during the evaluation.
RCM examination was performed in all lesions (VivaScope 1500; Caliber I.D., Rochester, NY, USA). Sequential images were recorded in horizontal 4×4 to 8×8 mm mosaics (VivaBlock; Caliber I.D.) at 3 levels of the skin (epidermis, dermal-epidermal junction and dermis) and vertical sequential images (VivaStack; Caliber I.D.) in the more representative areas of the lesion. RCM images were later evaluated by 2 authors (I.G.M, S.S.) with 5 and 12 years of experience, respectively, blinded to dermoscopic images and histopathological diagnosis. A total of 45 RCM criteria were investigated during the evaluation.
Dermoscopic and RCM criteria included in the evaluation process were selected based on the data available in the literature and in our preliminary observations. Each evaluator for both the dermoscopic and the confocal study was asked to assess the presence or absence of pre-defined dermoscopic and RCM structures and to provide a final diagnosis.
Diagnostic accuracy, sensitivity (number of malignant lesions correctly identified as such) and specificity (number of benign lesions correctly identified as such) were calculated after the independent assessment of clinical, dermoscopic and RCM images. In a second analysis such parameters were determined for RCM considering clinical, dermoscopic and RCM information in a real clinical setting.
One or more 4-mm punch biopsies were obtained from all lesions at the most suspicious areas after clinical, dermoscopic and RCM evaluation. Histopathological features were systematically evaluated by 3 dermatopathologists (IGM, RMP, SS). Thirty-six histopathological criteria were evaluated. Discrepant cases were consulted to an external pathologist. All histopathological evaluators were blinded to the clinical information and histopathological diagnosis.
In bivariate analysis dichotomous variables were evaluated by χ2 test. In multivariate analysis of dermoscopic and RCM features a binary logistic regression was performed to differenciate between benign and malignant lesions. For the confocal, dermoscopic, and histopathological correlations, the Cohen kappa coefficient was calculated for each descriptor. Statistical evaluation was performed using SPSS statistical software for Windows, version 15.0 (SPSS Inc.).
A total of 114 pink flat skin lesions on the legs in 85 patients were included (57 women; 28 men), with a mean ± standard deviation (SD) age of 73.18 ± 11.96 years. Ten lesions were located on the thighs and 104 on the lower legs. A total of 80 malignant lesions (50 BCC, 17 BD, 9 AK, 4 SCC) were analysed and 34 benign lesions (16 VSD, 5 SK, 3 psoriasis, 2 LPLK, 2 porokeratosis, 1 LP, 1 lichen simplex chronicus, 1 flat wart, 1 dermatofibroma, 1 neurofibroma, 1 hypertrophic scar).
Clinical evaluation. A correct clinical diagnosis was established in 49.1% of cases (56/114) and 70.2% (80/114) considering exclusively the diagnosis of benignity or malignancy. The sensitivity for malignant lesions was 68.7% (55/80) and the specificity for benign lesions was 73.5% (25/34).
Dermoscopy. Dermoscopy following clinical assessment achieved 59.6% (68/114) correct diagnosis and 79.8% (91/114) correct diagnoses when differentiating between benign or malignant. The sensitivity for malignant lesions was 85% (68/80) and the specificity for benign lesions was 67.6% (23/34).
Reflectance confocal microscopy. RCM evaluation blinded to clinical and dermoscopic images rendered a correct diagnosis in 71.9% of cases (82/114), and 85.1% (97/114) if only benignity or malignancy were considered. The sensitivity of RCM was 90% (72/80) and the specificity was 73.5% (25/34).
RCM evaluation after clinical and dermoscopic evaluation rendered a correct diagnosis in 85.1% of cases (97/114), and 94.7% (108/114) correct diagnoses when discriminating between benignity and malignancy. The sensitivity of RCM improved to 97.5% (78/80) and the specificity to 88.2% (30/34).
Table I. Diagnostic accuracy, sensitivity and specificity of each technique
The most common criteria observed in BCC were the superficial scale, erosion/ulceration, white shiny structures, linear irregular vessels and clustered vessels (Table II). On the bivariate analysis multiple criteria, such as white shiny structures, erosion/ulceration, atypical vessels, arborizing vessels/telangiectasia, short fine telangiectasia, linear irregular vessels, polymorphous vessels, multiple blue-grey globules, leaf-like structures, blue-grey ovoid nests, buck-shot scatter dots (in-focus dots) and spoke wheel-like structures/concentric structures were statistically significant.
Table II. Frequencies of dermoscopic and reflectance confocal microscopy (RCM) parameters
On the multivariate analysis white shiny structures (p = 0.027), erosion/ulceration (p = 0.000) and short fine telangiectasias (p = 0.005) were statistically significant.
The most common dermoscopic features in the BD/SCC group were the superficial scale, glomerular vessels, dotted vessels and localized vessels (Table II). Dermoscopy of BD/SCC group exhibited 2 statistically significant criteria that were glomerular vessels and pink-brownish eccentric structureless areas. On the multivariate analysis pink-brownish eccentric structureless areas (p = 0.001), dotted vessels (p = 0.021) and glomerular vessels (p = 0.017) were statistically significant.
The most common dermoscopic features of the inflammatory group were the superficial scale, white shiny structures, glomerular, dotted, homogeneous and generalized vessels (Table II). Three criteria were statistically significant on the bivariate analysis: homogeneous vessels, generalized vessels and cornoid lamella. On the multivariate analysis only erosion/ulcer was a statistically significant protector criteria (p = 0.031).
The most frequent dermoscopic criteria in VSD were superficial scale (68.75%, 11/16), glomerular vessels (62.5%, 10/16), dotted and homogeneous vessels (56.25%, 9/16), generalized vessels (50%, 8/16) and white shiny structures (50%, 8/16). Generalized vessels (p = 0.026) and homogeneous vessels (p = 0.002) were statistically significant in multivariate analysis.
RCM criteria more frequently observed in BCC (Fig. 1) were ulceration/crust, streaming, non-visible papilla, basal cords/nodules, visible vessels, polymorphic vessels, convoluted glomerular vessels, melanophages and thickened collagen bundles (Table II). On bivariate analysis regular honeycomb, streaming (polarized honeycomb), non-visible papilla, basal cords/nodules, telangiectasias, branched vessels, curved vessels, straight vessels, polymorphic vessels, thickened collagened bundles and melanophages were statistically significant. Basal cords/nodules (p = 0.000), streaming (p = 0.001) and non-visible papilla (p = 0.03) reached statistical significance on multivariate analysis.
Fig. 1. Basal cell carcinoma. (a) Pink plaque on the right leg in a man in his 60s. (b) Dermoscopic image showed a superficial scale, pink-white areas, white shiny structures, generalized, atypical, polymorphous vessels (linear irregular vessels, short fine arborizing vessels, glomerular vessels). (c) Reflectance confocal microscopy (RCM) mosaic (1.5×1.5 mm) at the dermal-epidermal junction (DEJ) showing multiple clefted basaloid nodules, polymorphic vessels and thickened collagen bundles. (d) RCM image (0.5×0.5 mm). Detail of basaloid nodules and polymorphic vessels (branching vessels and convoluted glomerular vessels). (e) RCM image (0.5×0.5 mm). Polarized honeycomb on suprabasal layers. (f) Biopsy specimen revealed a nodular basal cell carcinoma. Haematoxylin-eosin, original magnification ×100.
Hyperkeratosis, parakeratosis, ulceration/crust, epidermal disarray, visible vessels and round to S-shaped blood vessels were the criteria most often observed in BD/SCC group (Table II, Fig. 2). Statistically significant RCM criteria on the bivariate analysis in BD/SCC group were parakeratosis, hyperkeratosis, targetoid cells, epidermal disarray and visible vessels. On multivariate analysis hyperkeratosis (p = 0.005), targetoid cells (p = 0.044) and epidermal disarray (p = 0.012) were statistically significant.
In the inflammatory group, the RCM criteria most frequently observed were hyperkeratosis, parakeratosis, visible vessels, round to S-shaped and convoluted glomerular vessels (Table II). RCM criteria on the inflammatory group that were statistically significant on the bivariate analysis were parakeratosis, hyperkeratosis, non-edged papilla, papillomatosis and dermal inflammatory cells. On multivariate analysis the presence of dermal inflammatory cells (p = 0.034) was statistically significant.
Fig. 2. Bowen’s disease. (a) Pink plaque on the left thigh of a man in his 70s. (b) Dermoscopic image revealed superficial scale, pink-brownish eccentric structureless area and localized, homogeneous, dotted and glomerular vessels. (c) RCM mosaic (1×1 mm) at suprabasal layers exhibiting epidermal dissarray and parakeratosis. (d) RCM image (0.5×0.5 mm). Detail of an atypical honeycomb pattern with targetoid cells and multinucleated cells in granular/spinous layer of epidermis. (e) RCM image (0.5×0.5 mm) at superficial papillary dermis showing round to S-shaped and convoluted glomerular vessels. (f) Biopsy specimen revealed hyperkeratosis, parakeratosis, acanthosis and full-thickness dysplasia of epidermis. Haematoxylin-eosin (H&E), original magnification ×100. Inset: detail of epidermal dysplasia with keratinocye atypia, atypical mitosis, multinucleated cells and dyskeratotic cells (H&E, original magnification ×200).
The most common criteria in VSD were visible vessels, round to S-shaped and convoluted glomerular vessels (Fig. 3). Statistically significant RCM criteria of VSD on bivariate analysis were parakeratosis (p = 0.045), spongiosis (p = 0.019), convoluted glomerular vessels (p = 0.012), dermal inflammatory cells (p = 0.037) and huddles of collagen (p = 0.048). No criterion was statistically significant on multivariate analysis.
Fig. 3. Venous stasis dermatitis. (a) Pink plaque on the right leg of a woman in her 70s. (b) Dermoscopic image exhibited superficial scales, white shiny structures, multiple rosette signs, white circles and generalized and homogeneous dotted vessels. (c) Reflectance confocal microscopy (RCM) mosaic (1×1 mm) at the dermal-epidermal junction revealing exocitosis, dermal inflammatory cells and melanophages. (d) RCM image (0.5×0.5 mm). Detail of the inflammatory cells and exocitosis. (e) RCM image (0.5×0.5mm). Round to S-shaped blood vessels in the centre of dermal papilla. (f) Biopsy specimen revealed hyperkeratosis, parakeratosis and acanthosis of the epidermis, and a dense, predominantly lymphocytic inflammatory infiltrate and dilated capillaries on the papillary dermis. Haematoxylin-eosin, original magnification ×100.
Dermoscopy – reflectance confocal microscopy. Classical criteria of pigmented BCC (blue-grey ovoid nests, leaf-like structures, spoke wheel/concentric structures and buck-shot scatter dots) correlated with moderate agreement with basal cords/nodules on RCM (k = 0.426, p = 0.000). Short fine telangiectasias correlated well with branched vessels on RCM (k = 0.442, p = 0.000), whereas ulceration/erosion on dermoscopy correlated with ulceration/crust on RCM (k=0.470, p < 0.001).
Reflectance confocal microscopy – histopathology. Among the RCM criteria, basaloid cords/nodules correlated well with basaloid nests on histopathology (k = 0.631, p = 0.000) and clefting on RCM with clefting on histopathology (k = 0.607, p = 0.000). Targetoid cells seen in BD by RCM had a good correlation with atypical mitosis on histopathology (k = 0.455, p = 0.045). Thickened collagen bundles on RCM correlated well with desmoplasia on histopathology with moderate agreement (k = 0.439, p = 0.000).
Some RCM criteria had poor correlation with their counterparts on histopathological examination: parakeratosis (k = 0.335, p = 0.000), hyperkeratosis (k = 0.362, p = 0.000), epidermal atypia (epidermal disarray on RCM) (k = 0.380, p = 0.000), or intratumoral melanin in basal cords/nodules (k = 0.359, p = 0.001).
Dermal structures, such as inflammation, vascularization and melanophages, presented very poor correlation between RCM and histopathology.
Pink flat lesions on the legs of elderly people are frequently seen in dermatologist consultations. Such lesions comprise a heterogeneous group of entities with different clinical significance and management, varying from inflammatory conditions to skin cancer. Clinical and dermoscopic diagnosis may be difficult due to lack of specific criteria. In order to establish a definite diagnosis, biopsies are frequently required, which is a procedure that in this clinical setting is not devoid of potential complications (ulceration or infection).
In recent years, multiple authors have described dermoscopic patterns of hypopigmented lesions, mainly based on vascularization (1–14).
We have observed, in agreement with patterns described in the literature, that BD is typically characterized by superficial scales and glomerular/dotted vessels arranged in clusters, superficial BCC by short fine telangiectasias, shiny pink-white areas and multiple small erosions, and VSD is defined by a scaly surface and homogeneous glomerular/dotted vessels in a generalized distribution.
However, important dermoscopic criteria (especially vascular criteria, such as glomerular/dotted vessels or scaly surface) overlap among different entities representing a decrease in dermoscopic specificity and diagnostic accuracy in the lower limbs.
RCM is a non-invasive real-time technique that has been useful in the diagnosis of skin cancer and inflammatory skin diseases. Recently, multiple hypopigmented lesions have been described by means of RCM (15–28) trying to help clinicians to decide confidently whether a pink lesion should be biopsied. Thus, techniques such as RCM may avoid unnecessary biopsies and allow monitoring of the response to non-invasive treatments, such as photodynamic therapy, topical imiquimod, ingenol mebutate gel, topical diclofenac or topical 5-fluorouracil (29–34).
In a prospective blinded design we observed that clinical and dermoscopic evaluation have an elevated rate of misdiagnosis in pink flat lesions on the legs, whereas RCM improves diagnostic accuracy. In clinical evaluation, we observed a tendency to underestimate malignant pink lesions; whereas in dermoscopic evaluation, due to high presence of vascularity in pink lesions on the legs, we tended to overestimate malignancy. Dermoscopy presented low diagnostic accuracy (59.6%), moderately good sensitivity (85%), but low specificity (67.6%), even lower than clinical examination. In our study, blinded RCM has demonstrated higher levels of sensitivity (90%), specificity (73.5%) and diagnostic accuracy (71.9%). In a more realistic model, in which RCM assessment was performed after clinical and dermoscopic evaluation, diagnostic values increased to 97.5%, 88.2% and 85.1%, respectively. These results highlight dermo-scopy and RCM as complementary/synergistic techniques for diagnosing pink flat lesions on the legs.
In concordance with the literature, our study showed through multivariate analysis the following significant RCM criteria in BCC: basal cords/nodules, streaming and non-visible papilla (15, 16). Basal cords/nodules had a good correlation with classical dermoscopic criteria of pigmented BCC and with the presence of basaloid nests in histopathology. The BD/SCC group showed, as previously reported: hyperkeratosis, targetoid cells and epidermal disarray (17, 21, 23, 24). Interestingly, targetoid cells had a good correlation with atypical mitosis. Finally, the inflammatory group showed the presence of dermal inflammatory cells, as in previous reports (26). However, the agreement with histopathological inflammation was poor, probably because it is difficult to assess dermal features by RCM.
Other criteria, such as spongiosis, parakeratosis and round to S-shaped blood vessels, did not show significant association with the inflammatory group due to the small number of cases and the presence of these criteria in some cases in the BD/SCC group.
Surprisingly, multivariate analysis did not show significance of any kind of vessels; perhaps due to a higher prevalence of vascularity in the lower limbs, frequent overlapping of vascular patterns among different entities, and technical difficulties when evaluating dermal features in hyperkeratotic lesions.
In view of these results, we propose a RCM algorithm (Fig. 4) to improve the diagnosis of pink flat skin lesions on the legs, in which the main criteria are obtained from the results of multivariate analysis. An initial step has been added to this algorithm to rule out a melanocytic lesion, in accordance with other RCM algorithms (18) proposed in solitary pink lesions, since the screening of malignant melanoma is essential when evaluating a cutaneous pink lesion.
Fig. 4. Reflectance confocal microscopy (RCM) algorithm. *Junctional nests/thickenings, dermal nests, widespread atypical cells at dermal-epidermal junction. BCC: basal cell carcinoma; AK: actinic keratosis; SCC: squamous cell carcinoma.
No case of amelanotic/hypomelanotic melanoma could be included in our series because of the low prevalence (2–8%) of this subtype of malignant melanoma (10).
Definite diagnosis was established according to a 4-mm punch evaluation chosen by RCM findings in all cases, which may have caused confocal false negatives according to histopathology if the sample was not perfectly representative of the lesion.
Thick hyperkeratosis, ulceration and crusts represented a technical limitation in the dermoscopic-RCM-histopa-thology correlation, because they may have hampered the quality of RCM imaging or not allowed sufficient penetration of RCM light to reliably assess dermal features.
Larger series with different pink tumours (especially melanoma) and inflammatory/infectious conditions should be studied to confirm our results.
This study demonstrated that, in this clinical setting, where clinical evaluation and dermoscopy do not possess high specificity, RCM might be a useful tool, since, importantly, it may improve diagnostic accuracy, sensitivity and specificity for non-melanoma skin cancer diagnosis, thus reducing the number of biopsies and their consequences (pain, costs, scars, infections and chronic ulcers).
Additional contributions: Carlos Barranco, MD (Department of Pathology, Hospital del Mar-Parc de Salut Mar, Univesitat Autònoma de Barcelona, Spain) helped with histopathological examination in discrepant cases. There was no financial compensation other than salary.
Additional information: This work was conducted within the framework of the PhD in medicine for Dr Gómez-Martín from the Universitat Autònoma de Barcelona. Biological samples were obtained from Parc de Salut MAR Biobank, Barcelona.
Funding source: This work was supported by grants RD09/0076/00036 and PT13/0010/0005 from Instituto de Salud Carlos III/FEDER and the Xarxa de Bancs de tumors, sponsored by Pla Director d’Oncologia de Catalunya.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize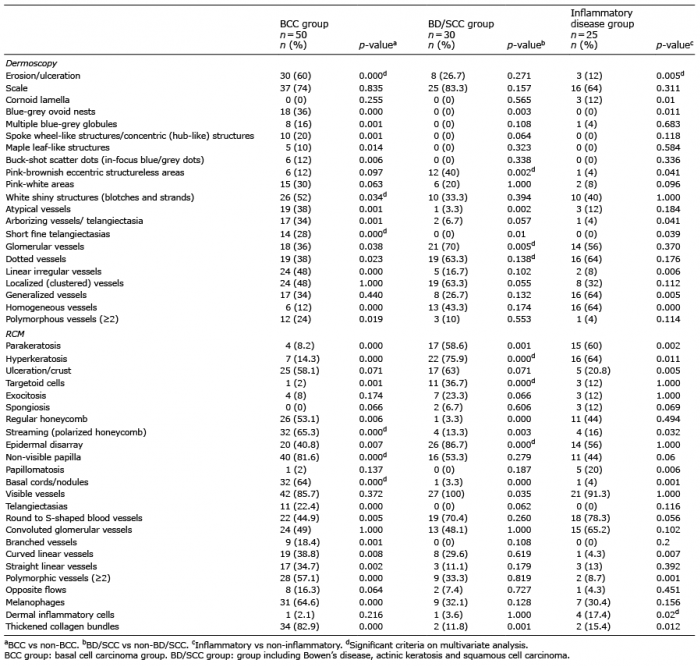 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize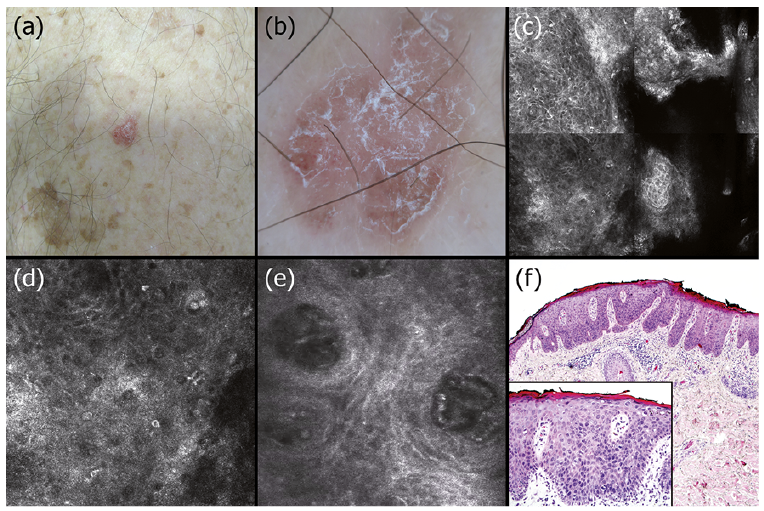 Click to show fullsize
Click to show fullsize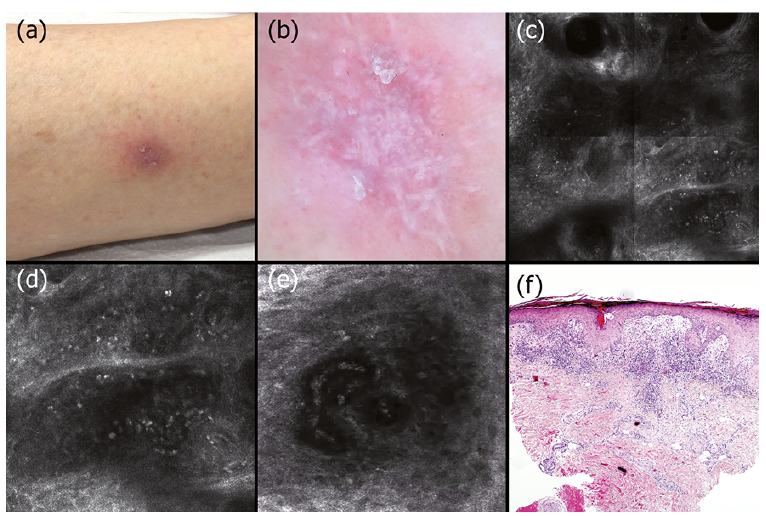 Click to show fullsize
Click to show fullsize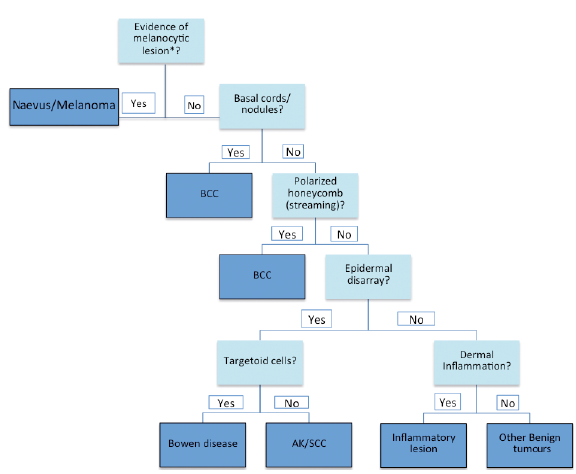 Click to show fullsize
Click to show fullsize