


1Dermatology Clinic, and 2Institute of Interdisciplinary Research in Molecular Biology, Biostatistics Department, Université libre de Bruxelles, ULB, Brussels, Belgium
Papulopustular rosacea and demodicosis are characterized by non-specific symptoms, which can make clinical diagnosis difficult. This retrospective study of 844 patients assessed the diagnostic importance of clinical signs and symptoms that are poorly recognized as being associated with these conditions. In addition to well-known signs (vascular signs (present in 80% of patients), papules (39%), pustules (22%) and ocular involvement (21%)), other signs and symptoms (discreet follicular scales (93%), scalp symptoms (pruritus, dandruff or folliculitis; 38%) and pruritus (15%)) may also suggest a diagnosis not only of demodicosis, but also of papulopustular rosacea. Facial Demodex densities (measured by 2 consecutive standardized skin biopsies) were higher when ocular or scalp involvement was present, suggesting more advanced disease, but further investigations are needed to confirm this hypothesis. Recognition of these clinical signs and symptoms should encourage dermatologists to perform a Demodex density test, thus enabling appropriate diagnosis to be made.
Key words: Demodex; rosacea; demodicosis; scalp; dandruff; pruritus.
Accepted Sep 18, 2018; Epub ahead of print Sep 18, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Fabienne Forton, Dermatology Clinic, rue Frans Binjé, 8, BE-1030 Brussels, Belgium. E-mail: fabienne.forton@skynet.be
Papulopustular rosacea and demodicosis are common facial skin conditions that can be difficult to diagnose clinically. In addition to well-known clinical signs, such as vascular signs and papules, in our study of patients with known papulopustular rosacea or demodicosis, we showed that other clinical signs (discreet facial follicular scales, dandruff, folliculitis on the scalp, facial or scalp pruritus) are also frequently present. Presence of these signs and symptoms should therefore encourage dermatologists to perform further diagnostic tests (e.g., the recently described test based on the high density of Demodex mites observed in these conditions), to ensure accurate diagnosis.
Papulopustular rosacea (PPR) and demodicosis are common skin conditions with non-specific signs and symptoms (1–3). PPR is characterized mainly by central face distribution of persistent erythema and papulopustules (1, 2) (Fig. 1). Most cases of demodicosis are pityriasis folliculorum (Fig. 2) or rosacea-like demodicosis (3–7), this being considered by some authors as the same disease as PPR (8–11). Less frequently, demodicosis can manifest as folliculitis or abscesses (3, 12–15), hyperpigmentation (3, 5, 16), follicular eczematids (defined as erythema, dilated pores, granular skin, some papules and non-follicular scales) (3), isolated inflammatory papules (3, 17), and ocular demodicosis (5, 16, 18–29).
Fig. 1. A 25-year old man with papulopustular rosacea and extensive demodicosis involving the entire head. (A, C) Papulopustular rosacea on the face; (B) typical cylindrical dandruff at the base of the eyelashes (black arrows); (B, D) visible pityriasis folliculorum (blue arrows) on the upper left eyelid and on the pre-auricular zone; (D) papulopustular rosacea involving the left ear lobe. He also had dandruff on the scalp. SSSB1+SSSB2 values are indicated on the figure. Patient permission was obtained. This patient, seen recently, was not included in the study.
Fig. 2. A 70-year old woman with demodicosis of the whole head. (A, B) The facial skin shows pityriasis folliculorum and associated seborrhoeic dermatitis (Malassezia furfur +). SSSB1+SSSB2 values are indicated on the figure; (C) 7 of her Demodex mites free in immersion oil (×100). (D) The eyelids show cylindrical dandruff and blepharitis with 2.8 mites/eyelash; (E) ± 6 mites around one of her eyelashes (×100). (F) The scalp shows dandruff, which could also be related to her seborrhoeic dermatitis. Nevertheless, numerous mites were found on epilated hairs; (G) ± 8 mites on her epilated hairs (×40). Patient permission was obtained.
The diagnosis of PPR and demodicosis from clinical signs alone can be difficult, but can be confirmed using a new diagnostic test (30) based on the high skin Demodex density (Dd) in these patients (30–36). In addition to well-known clinical signs, many patients with PPR or demodicosis have other signs that are less frequently recognized as being associated with these conditions. Recognition of the possible role of these more discreet clinical signs could encourage dermatologists to assess the Dd, and thus improve diagnosis and treatment.
The present study therefore assessed the diagnostic importance of clinical signs and symptoms that are poorly recognized as being associated with PPR or demodicosis: follicular scales, scalp symptoms and pruritus. We hypothesized that these less obvious features may be useful diagnostic indicators not only of demodicosis, in which they are known to occur, but also of rosacea. This study also investigated the relationship of ocular involvement and scalp symptoms with Dds measured by 2 consecutive standardized skin surface biopsies (SSSBs).
This retrospective study is an analysis of data obtained from 844 patients (254 patients with symptoms suggestive of PPR (i.e. rosacea with centro-facial papulopustules) (1) and 590 patients with demodicosis) who were included in a study to assess a new diagnostic test for rosacea and demodicosis (Table SI) (30). The 254 PPR-suggestive patients included 215 patients with PPR with persistent erythema (i.e., typical PPR according to the consensus of the National Rosacea Society (NRS) (1)), 27 with rosacea without persistent erythema, 7 with granulomatous rosacea and 5 with steroid-induced rosacea (30). The study was approved by the Erasme Hospital ethics committee.
For each patient, the date of consultation, age, sex, clinical diagnosis, symptoms, ocular involvement (cylindrical dandruff, blepharitis, conjunctivitis, chalazion), other potentially associated facial dermatoses (such as seborrhoeic dermatitis) and recent treatment for the facial condition were recorded. At the start of the data collection in 2002, the importance of scalp involvement (pruritus, folliculitis of the scalp or dandruff), especially in rosacea, was not realized and was not looked for specifically in these patients. From August 2005, however, we started to systematically look for scalp involvement and therefore analysed these patients separately (subgroup A, n = 488). In addition, to limit the effect of confounding factors that could potentially influence the cutaneous facial symptoms, we also studied these symptoms in a group of 490 patients (subgroup B) who had received no treatment during the 3 months prior to their consultation and had no other associated facial dermatoses (Fig. 3).
Fig. 3. Two subgroups were analysed separately. Subgroup A comprised patients included from August 2005 (n = 488), the time-point at which we started looking specifically for possible scalp involvement in our patients. The prevalence of pruritus and scalp symptoms is likely better reflected in this group. Subgroup B comprised patients with no recent treatment and without an associated facial dermatosis (n = 490). The aim of this subgroup was to study the signs and symptoms while avoiding these potential confounding factors. The 2 subgroups were not mutually exclusive; 267 patients were present in both groups.
In all patients, 2 consecutive SSSBs were performed at the same place, collecting the 2 first layers of 1 cm2 of the horny layer of the skin and of the follicular content. Full details of the method, including an online video, are available in an earlier publication (30).
The number of epilated lashes and the number of Demodex mites visualized on the lashes were also collected for patients with clinical ocular involvement (Fig. S1).
Continuous variables are summarized by means ± standard error of the mean (SEM) and qualitative variables by n (%).
Differences in continuous variables among groups were compared using analyses of covariance (ANCOVA), including age and sex as covariates, followed by Sidak tests for multiple comparisons if required. Differences in qualitative variables were compared among groups using Pearson exact χ2 tests.
Statistical significance was considered when p < 0.05. All statistical tests were performed using IBM-SPSS (version 23.0 to 24.0) software (IBM Corp, Armonk, NY, USA).
The demographic data for the 844 patients have been reported previously (30).
The initial complaint was localized to the face in 805 patients (95%), the scalp in 22 (3%) and the eyes in 17 (2%). When the initial complaint was elsewhere than the face, clinical examination nevertheless generally revealed facial demodicosis (n = 37/39); the facial skin appeared healthy in only 2 patients. In 6 patients (0.7%), the initial complaint was subjective: feeling of dry skin (n = 2), sensitive skin (n = 2), cosmetic intolerance (n = 1), burning facial sensation (n = 1).
The prevalences of the signs and symptoms were similar in subgroups A and B to those in the whole cohort, except for pruritus, scalp symptoms and ocular involvement (Table SII).
Follicular scales were observed more frequently than vascular symptoms in the total cohort (782/844 (93%) vs. 677/844 (80%), p < 0.001) and in the 2 subgroups (Table SII).
In the total cohort of 844 patients, the presence of follicular scales was related to the presence of persistent erythema (p = 0.020), but not to the presence of flushes (p = 0.497). Concordance for the presence of follicular scales and vascular symptoms was 70% (565/844 had both signs, and 26/844 had neither).
In subgroup B (n = 490), the presence of follicular scales was not related to the presence of flushes (p = 0.283) nor to the presence of persistent erythema (p = 0.060). Concordance for the presence of follicular scales and vascular symptoms was 71% (336/490 had both signs and 13/490 had neither). The proportions of patients with follicular scales and with vascular symptoms differed according to the clinical diagnosis: vascular symptoms were more frequent in the PPR-suggestive group than in the demodicosis group; there was no significant difference in the frequency of follicular scales in these 2 groups or between the PPR-suggestive with and without persistent erythema groups (Table SIII).
In the total cohort, 130 (15%) patients had pruritus and 5 had excoriated facial prurigo (Fig. S2). Most of the patients with pruritus (117/130 (90%)) were observed among the 488 patients included from August 2005, giving a prevalence of 24% in this subgroup (Table I and Table SII): the pruritus was localized to the scalp in 106 patients (22%), to the face in 15 patients (3%) and to the eyes in 2 patients (0.4%); more than one site was affected in 5 patients.
Table I. Prevalence of follicular scales, pruritus, scalp symptoms and ocular involvement in subgroup A (patients included from August 2005)
In the total cohort, 321 (38%) patients had scalp symptoms, most of whom (n = 244) were in subgroup A, giving a prevalence of 50% in this subgroup (Table I and Table SII).
In this subgroup, the mean Dd in the facial skin tended to be higher when the patients had scalp symptoms than when they did not, but this difference was not statistically significant (Table SIV). For 2 patients with scalp symptoms, Dd samples were taken from the scalp: for 1, 9 Demodex mites were observed on epilated hair (Fig. 2), for the other, the SSSB1 and SSSB2 were 24 and 25 D/cm2, respectively, on the vertex.
In this subgroup, the presence of scalp symptoms and presence of an associated facial seborrhoeic dermatitis were related (p < 0.001). The total concordance was 58% (65/488 had both signs and 219/488 had neither).
In the total cohort, 180 (21%) patients had clinical ocular involvement (Table SII, Fig. 2). The prevalence of ocular involvement was significantly higher in PPR-suggestive than in demodicosis patients (70/254 (28%) vs. 110/590 (19%), p = 0.004), but not significantly different in patients with PPR with and without persistent erythema (64/215 (30%) vs. 4/27 (15%), p = 0.117). Two of the 7 patients with granulomatous rosacea had ocular involvement.
The patients with ocular involvement had higher mean facial Dds than those without (Table SV). The eyelashes were analysed in 161 of the 180 patients with clinical ocular involvement and Demodex mites were found in the eyelashes in 147 patients (91%), giving an overall mean of 1.6 ± 0.1 Demodex mites/lash. There were no significant differences in the numbers of mites on the eyelashes according to age (p = 0.337) or sex (p = 0.128). There were no statistically significant differences in the mean number of mites/eyelash or in the facial skin Dds in the different subgroups of clinical ocular involvement (cylindrical dandruff, blepharitis, conjunctivitis, chalazion) (Tables SVI and SVII).
In subgroup A, 140 of the 488 patients (29%) had clinical ocular involvement (Table I) and these patients had a higher mean facial Dd than those without ocular involvement (Table SIV). In this subgroup A, ocular involvement and scalp symptoms were related (p = 0.012). The concordance was 55% (83/488 of the patients had both signs and 187/488 had neither).
Follicular scales were the most frequent sign observed in our patients, occurring significantly more frequently than vascular symptoms. Scalp symptoms and pruritus were present, respectively, in 50% and 24% of the patients included from August 2005, when we started to systematically look for these symptoms (subgroup A). Follicular scales, scalp symptoms and pruritus were observed with the same frequency in demodicosis and rosacea, and in rosacea with or without persistent erythema. The mean Dd in the skin was higher when the eyelids or scalp were involved (although the latter finding was not statistically significant) and these 2 signs were often present together.
The high frequency of follicular scales in patients with PPR and with demodicosis is not surprising because they correspond to Demodex opisthosomas protruding at the follicular orifice (Fig. 4) and these patients are known to have very high Dds in their skin (30–36). Nevertheless, follicular scales have not been considered as a sign to suggest the diagnosis of rosacea. We showed that the presence of follicular scales was statistically related to the presence of persistent erythema, which is a diagnostic criterion for rosacea, supporting the use of follicular scales as a diagnostic indicator of this condition. Importantly, follicular scales can be very discreet and may need close examination to be detected (Fig. 4): they can resemble extruded comedones, trichostasis, follicular hyperkeratosis and ulerythema ophryogenes so 2 consecutive SSSBs should be performed at the same site to confirm the clinical diagnosis (30).
Fig. 4. Follicular scales: detection and significance. (A) Pityriasis folliculorum on the right cheek of a 55-year-old man consulting recently (not included in the study) for symmetrical hyperpigmentation of the beard present for 2 years (blue arrow). (B) Close examination revealed thin whitish follicular scales at the base of the hair, giving a frosted appearance and a rough texture. Each follicular scale corresponds to the most superficial part of numerous opisthosomas agglutinated in the follicle (blue box on B, C, D, E). (C) The scales are more visible when the skin was cleaned with ether and using tangential illumination. (D) Schematic representation of numerous Demodex mites, agglutinated at different levels (arrows) inside the follicle. (E) Microscopic view (×100) of 10 D. folliculorum agglutinated in a single follicle on a standardized skin surface biopsy (SSSB). In this patient, the 2 successive SSSBs revealed 160 and 340 D/cm2 respectively. The final diagnosis was demodicosis: pityriasis folliculorum with secondary post-inflammatory pigmentation on phototype V. Patient permission was obtained.
As expected, vascular symptoms were more frequent in the PPR-suggestive group than in patients with demodicosis, because, by definition, all patients with typical PPR have persistent erythema. However, most of the patients with pityriasis folliculorum (83%), the most frequent demodicosis, also had vascular symptoms: these patients are usually diagnosed as having simple erythematotelangiectatic rosacea (ETR) or flushes because these vascular symptoms are easily visible, whereas follicular scales are more discreet. Interestingly, however, 17% of patients with pityriasis folliculorum had no vascular symptoms and 10% had only flushing (Table SIII), thus a diagnosis of pityriasis folliculorum should also be considered when no vascular symptoms are present.
The high prevalence of scalp involvement was an unexpected finding of this study. Because scalp involvement has rarely been reported in demodicosis (37–42), and even more rarely in rosacea (43–46), its presence was not specifically looked for when the study started, which explains why most of the patients with scalp involvement were identified in the later phase of the study.
Because scalp SSSB is painful, diagnosis of scalp involvement was not confirmed by parasitological examination (except in 2 patients). To confirm that these scalp symptoms correspond to true scalp involvement by Demodex mites, future studies are needed that systematically assess the Dd on the scalp, using techniques other than SSSB, such as confocal laser microscopy. Dermoscopy has a much lower resolution than confocal laser microscopy and, to our knowledge, cannot differentiate Demodex mites from other conditions (e.g. follicular hyperkeratosis, extruded comedones, trichostasis) nor measure their density. The presence of seborrhoeic dermatitis may also be associated with dandruff or pruritus of the scalp. Indeed, the presence of scalp symptoms was statistically related to the presence of facial seborrhoeic dermatitis. Nevertheless, in our experience, scalp symptoms are generally the first clinical symptoms to disappear with acaricidal treatment, indirectly confirming abnormal proliferation of Demodex on the scalp. Application of an acaricidal treatment, not only to the face, but also systematically to the scalp, may therefore be useful in patients with demodicosis and those with rosacea to normalize the Dds on the whole head. This approach may influence treatment efficacy and reduce potential relapses, but this hypothesis needs to be confirmed by prospective studies.
Pruritus, traditionally associated more with demodicosis (14, 15, 28, 29), was observed with the same frequency in demodicosis and rosacea. As pruritus was most frequently localized to the scalp, the occurrence of pruritus in subgroup A (24%) probably better reflects the real prevalence compared with that reported in the entire group of 844 patients. Nevertheless, this percentage is less than that reported by Akilov and colleagues, who observed pruritus in all their patients with demodicosis (28). The reasons for this difference are unclear.
The proportion of patients with ocular involvement (21%), although comparable to that reported in other studies (28, 47), was less than that reported in patients with rosacea recruited from an ophthalmological consultation (48, 49). In patients with clinical evidence of ocular involvement, Demodex mites were generally found on the eyelashes (91%), with a mean of 1.6 ± 0.1 Demodex mites/lash, confirming data from Gao et al. (18).
The mean Dds in the skin were greater when the eyes were involved and when the scalp was involved, although the latter finding was not statistically significant; moreover, eye and scalp involvement were often observed together. These observations suggest that ocular and scalp involvement probably represent a more advanced stage of the disease, as has already been reported (47, 50). Bae et al. (50) observed a significant association between the severity of ETR and ocular rosacea. Tan et al. (47) observed that ocular signs developed after the establishment of cutaneous signs, and that PPR tended to occur after ETR; moreover, they observed ocular involvement in 42% of patients with the PPR subtype and 33% of those with the ETR subtype.
Although ocular involvement and vascular symptoms were more frequent in PPR-suggestive patients than in those with demodicosis, and in PPR with than without persistent erythema, other signs (follicular scales, scalp involvement and pruritus) were encountered with a similar prevalence in these different groups. As these subgroups also have similar Dds (11, 30), our observations are compatible with the hypothesis that these diagnostic groups (PPR-suggestive, demodicosis, PPR with and without persistent erythema) may all be phenotypes of the same disease (10, 11).
In conclusion, this study highlights the high frequency of discreet follicular scales in patients with rosacea and demodicosis, stressing their value in diagnosis and the utility of close clinical examination to detect them, especially when the clinical diagnosis is difficult. Our results also suggest that these diagnoses should be considered in patients with pruritus or symptoms localized to the scalp (dandruff, pruritus, folliculitis), which are frequently associated with ocular involvement and are likely to correspond to an advanced stage of disease.
The study was approved by our local IRB (Erasme Hospital, P 2014/117).
Conflicts of interest: FMNF occasionally works as a consultant for Galderma, VDM has no conflicts of interest to declare.
 Table SI Figure S1 Figure S2 Table SII Table SIII Table SIV Table SV Table SVI Table SVII
Table SI Figure S1 Figure S2 Table SII Table SIII Table SIV Table SV Table SVI Table SVII

 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize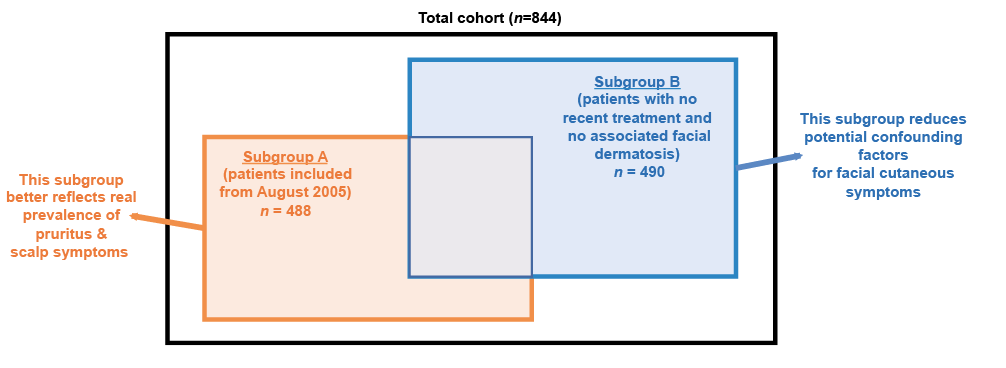 Click to show fullsize
Click to show fullsize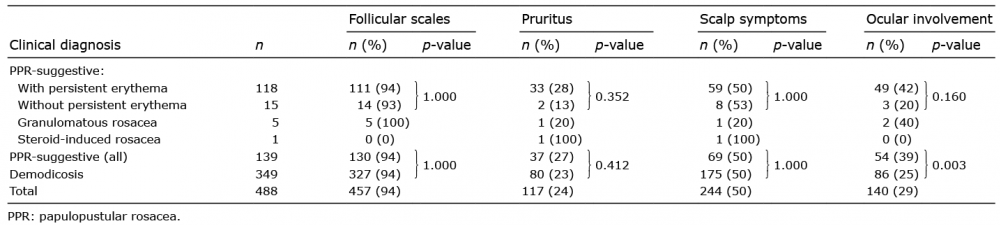 Click to show fullsize
Click to show fullsize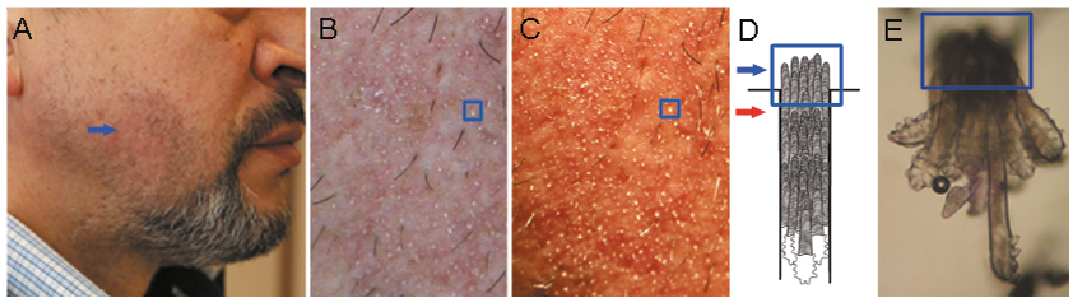 Click to show fullsize
Click to show fullsize