


Department of Dermatology, Kansai Medical University Medical Center, 10–15 Fumizono-cho, Moriguchi, Osaka 570-8507, Japan. E-mail: kiyohart@takii.kmu.ac.jp
Accepted Sep 18, 2018; E-published Sep 18, 2018
Progressive nodular histiocytosis (PNH) is a rare normolipaemic macrophage disorder first reported by Taunton et al. in 1978 (1). PNH belongs to a subgroup of unifying non-Langerhans cell histiocytoses (NLCHs), or the xanthogranuloma (XG) family (2). It displays a progressive clinical course with no signs of spontaneous resolution, and is characterized by the histological finding of a nodular infiltrate of spindle cells in a storiform arrangement intermingled with foamy cells and Touton giant cells (3, 4).
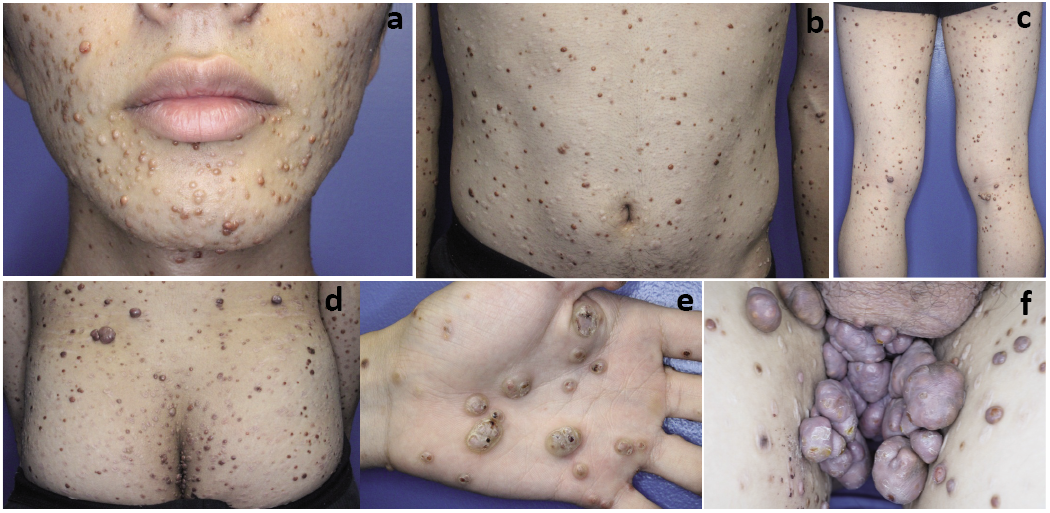
An 11-year-old boy presented with multiple painless nodules on his trunk and extremities that started at the age of 9 years as yellow to brown papular lesions. Although spontaneous regression was expected on the basis of the histopathological diagnosis of juvenile XG, new lesions continued to appear over time. At the age of 17 years, the boy had large nodules on his face, trunk, and upper and lower limbs (Fig. 1a–c), most of which were 1–2 cm in diameter, smooth-surfaced, and yellow to brown. The number of lesions was over 200. These nodules tended to be larger on the buttocks, knees, palms and soles (Fig. 1d, e). In particular, several nodules had coalesced, leading to a size of over 20 cm in largest diameter on the perineum to bilateral inguen (Fig. 1f). A biopsy specimen from a forearm lesion at 11 years demonstrated a dermal nodule containing foamy cells and multinucleated Touton giant cells (Fig. 2a). Histological examination at 17 years revealed a dermal nodular infiltrate of spindle cells in a storiform arrangement beneath a thinned epidermis (Fig. 2bc), reminiscent of dermatofibroma or spindle cell XG. Foamy cells, Touton giant cells, and foreign body giant cells were scattered throughout and aggregated in the periphery (Fig. 2d). Immunohistochemical examination demonstrated strong positivity for CD68 in most cells (Fig. 3a). A minority of spindle cells were positive for factor XIIIa (Fig. 3b). Cells were negative for S-100 protein, CD1a, α-smooth muscle actin, and factor VIII-related antigen. The Ki-67 proliferation index was ~10% (Fig. 3c). On the basis of the diagnosis of PNH, the bulky mass was resected surgically with satisfactory results.
Fig. 1. Clinical appearance, 17-year-old boy. Smooth-surfaced, yellow to brown nodules on (a) face, (b) trunk, (c) lower limbs, (d) buttocks, and (e) left palm. A bulky mass over 20 cm in largest diameter, composed of coalesced nodules on (f) the perineum to bilateral inguen.
Fig. 2. (a) Foamy cells and multinucleated Touton giant cells from a lesion on the patient at 11 years. (b) A dermal nodular infiltrate beneath a thinned epidermis composed of (c) spindle cells in a storiform arrangement, accompanied by (d) foamy cells, Touton giant cells, and foreign body giant cells in the periphery at 17 years. (Haematoxylin and eosin (HE), a: ×400, b: ×12.5, c: ×100, d: ×400).
Fig. 3. Immunohistochemistry. (a) Most cells were positive for CD68. (b) A minority of spindle cells were positive for factor XIIIa. (c) The Ki-67 proliferation index was ~10% (a: ×400, b: ×400, c: ×400).
The present case exhibited progressive disease activity without spontaneous regression, consistent with the clinical course of PNH, not multiple XG. Histological findings demonstrated a nodular infiltrate of spindle cells in a storiform arrangement intermingled with foamy cells and Touton giant cells. NLCHs, or members of the XG family, have the monocyte/dendritic cell lineage in common, and are classified according to the predominant mononuclear and/or multinucleate histiocytic cell types (2). These disorders often overlap and progress to other clinical forms, depending on the patient’s immune status and the triggers of macrophage proliferation (5). While overlapping cases of PNH and juvenile XG have been reported (4), the present case could be diagnosed as PNH because of the progression over time. Although the lesions in PNH are widely and randomly distributed on different sites of the body, the flexor areas and joints are usually spared, according to a review by Nofal et al. (3). In the present case, the nodules tended to be larger on the buttocks, knees, palms, soles, and perineum, in contrast with previous reports. We speculated an exacerbation by external stimuli. Furthermore, the previous reports included cases with over 100 nodules measuring up to 7 cm, as reported by Gonzalez Ruíz et al. (6), hundreds of nodules measuring up to the size of a plum, as reported by Hilker et al. (7), and 85 nodules up to 6 cm, as reported by Nofal et al. (3). The present patient had over 200 nodules and a bulky mass over 20 cm. The number of nodules may be insignificant, however, since it does not directly correlate with the aggressiveness of the disease. However, such a bulky mass as in the present case has not been reported previously. Because surgical resection of selected nodules is thought to be the only therapeutic option in PNH (8), this option was chosen for the bulky mass for cosmetic reasons.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize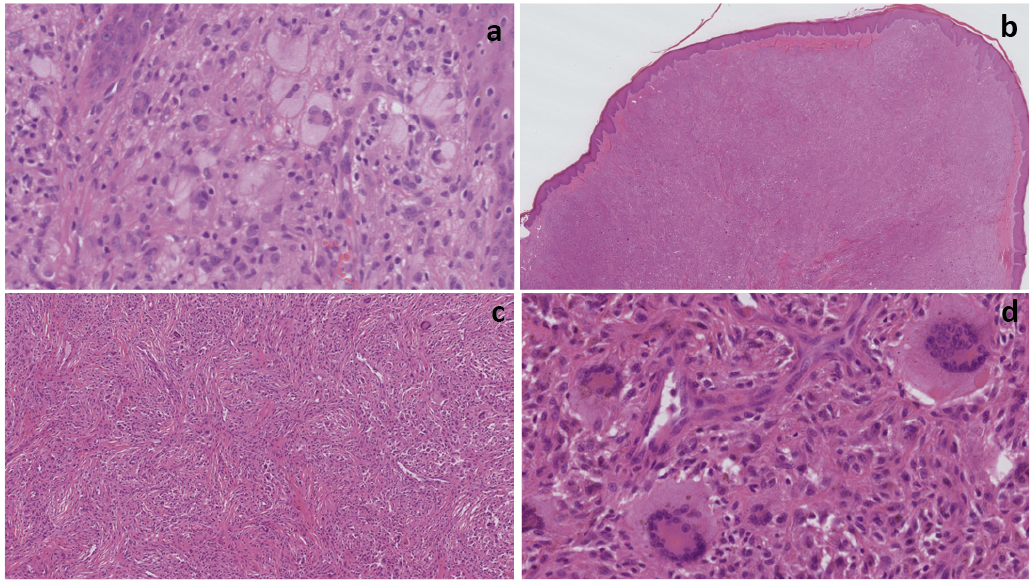 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize