


1Department of Dermatology, Bispebjerg Hospital, University of Copenhagen, Bispebjerg Bakke 23, DK-2400 Copenhagen NV, and 2Clinic of Dermatology, Karlslunde, Denmark. E-mail: stine.regin.wiegell@regionh.dk
Accepted Sep 23, 2018, Epub ahead of print Sep 24, 2018
The introduction of daylight-mediated photodynamic therapy (d-PDT) has resulted in pain-free field treatment of multiple actinic keratoses (AK) of the face and scalp (1). Erythema and crusting may be less pronounced after d-PDT compared with conventional PDT (c-PDT) using red light (2, 3). During PDT of multiple AK of the face and scalp, patients are affected by inflammation, which may cause absence from work or social activities. In a recent study we introduced the concept of pulse-PDT, in which methyl aminolevulinate (MAL) cream is applied for only 30 min under occlusion and then removed to ensure selective accumulation of the photosensitizer protoporphyrin IX (PpIX) in the mitochondria and cytosol of the diseased cells (4). The study showed that the use of pulse-PDT could reduce erythema after PDT of multiple AK on the face and scalp (4). The use of a super-potent corticosteroid before and just after pulse-PDT further reduced erythema.
The objective of this randomized study was to evaluate whether the combination of pulse-corticosteroid-daylight-PDT (PS-d-PDT) would result in less post-PDT erythema than d-PDT without affecting the efficacy of the treatment of multiple AK on the face and scalp. A further aim was to clarify whether the use of brimonidine tartrate (BT), a selective α2-adrenergic receptor agonist, could result in a further short-term reduction in PDT-induced erythema.
Twenty-five male patients with a total of 823 AK were included in the study. AK on the face or scalp were marked in 2 symmetrical squared areas and randomized to d-PDT or PS-d-PDT, respectively. After lesion counting and mapping, a sunscreen (Actinica® SPF 50+, Galderma, Uppsala, Sweden) was applied. Following lesion preparation with a curette, MAL cream (Metvix®, Galderma) was applied to both treatment areas without occlusion. After 30 min, the MAL cream was removed in the area randomized to PS-d-PDT and super-potent glucocorticosteroid (Dermovat®, GlaxoSmithKline, Broendby Denmark) was applied. The MAL was not removed from the d-PDT until after daylight exposure. Patients exposed themselves continuously to daylight for 2 h, after which they stayed indoors for the remainder of the day. Erythema was evaluated 24 h after PDT, at which time BT gel was applied in both treatment areas, and erythema was re-evaluated 30 min later. Erythema was measured using a skin reflectance meter (Optimize Scientific 558; Chromo-Light, Vedbaek, Denmark) (5) and evaluated visually by the investigator using a 4-point scale. Patients scored the pain using a numerical scale (0–10) in both areas every 30 min during daylight exposure.
The study was approved by the ethics committee of Region Hovedstaden (H-4-2011-151). Statistical analyses were performed with GraphPad Prism® (GraphPad Software Inc., USA). Wilcoxon matched-pairs signed rank test was used to compare paired data and for correlations Spearman R correlation was used. A p-value < 0.05 was considered significant.
No difference was found between the 2 treatment areas in baseline characteristics, such as lesion count and ery-thema. Ninety percent of the lesions were grade I AK. One patient was excluded from the BT part of the study due to treatment with MAO-inhibitors.
The visually evaluated erythema one day after treatment was less in areas treated with PS-d-PDT compared with d-PDT (p = 0.0032).
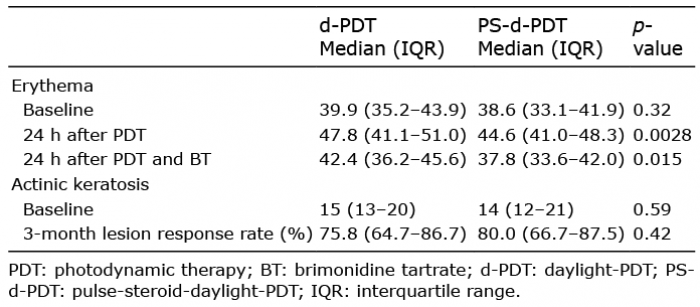
Measured erythema was significantly increased the day after both treatments compared with baseline (p < 0.0001). Median erythema was significantly higher in the d-PDT areas than in the PS-d-PDT areas the day after treatment (p = 0.028) (Table I).
The use of BT on the treated areas 1 day after treatment significantly reduced erythema (p < 0.0001) (Table I). BT removed PDT-induced erythema as no significant difference was found between erythema before PDT and after BT in either d-PDT or PS-d-PDT treated areas (p = 0.77 and p = 0.27, respectively). Both treatments were almost pain-free, with a median maximal pain score of 1 (p = 0.81). No significant difference in efficacy was found between the 2 treatment areas (p = 0.42) (Table I).
At 3-month follow-up a mean of 1.4 new AK had developed in the d-PDT-treated areas, compared with 2.6 new AK in the PS-d-PDT-treated areas (p = 0.012). Lesion response rate was not associated with increased erythema (p = 0.51 and p = 0.78).
Table I. Erythema and number of actinic keratosis before and after treatment in both areas
The use of PS-d-PDT resulted in only a minor reduction in erythema compared with d-PDT. In an earlier study PS-d-PDT more than halved the increase in erythema seen after c-PDT (4). As reported in other studies (2, 3), d-PDT induced much lower post-treatment erythema (21.2%), than c-PDT with red light (38.7%) (4), which makes it more difficult to achieve a significant reduction in erythema using the pulse-steroid approach. The use of pulse-steroid did not affect the efficacy of d-PDT or of c-PDT (4).
Super-potent corticosteroid was applied only once before exposure to daylight and not twice (before and after PDT) as in the former c-PDT studies (4, 6). Single application was used to ensure that corticosteroid was applied only to the PS-d-PDT area, but may explain some of the reduced effect on erythema in the present study. Further studies are needed to determine whether application of corticosteroid once daily after PDT would reduce erythema further.
The number of new AK in the treated areas 3 months after treatment was significantly higher in the PS-d-PDT-treated areas compared with d-PDT-treated areas. This difference was not found using conventional PDT (4, 6). The reason for more new AK lesion after PS-d-PDT is unknown, but may be caused by a less effective treat-ment of subclinical lesions, which could be evaluated using confocal microscopy. However, since no reduced efficacy of PS-d-PDT is found for visible AK this theory is not likely. The enhanced number of new lesions raises concern regarding the long-term efficacy of PS-d-PDT for AK.
We found that application of BT significantly reduced PDT-induced erythema 24 h after d-PDT. BT is a highly selective α2-adrenergic receptor agonist with potent vasoconstrictive activity, which is now approved for the treatment of facial erythema associated with rosacea (7). In 9 patients, BT gel reduced the erythema to a level below the redness before PDT. BT was only applied once 24 h after treatment, without affecting the efficacy of the treatment, since efficacy was comparable with other d-PDT studies (1, 8). It may therefore be safe for the patient to use a single application of BT before attending work-related and social activities. However, further research is needed to determine whether daily application of BT might affect the efficacy of PDT for AK due to vasoconstriction leading to less inflammation.
In conclusion, d-PDT induced less erythema than seen after conventional PDT. The use of PS-d-PDT resulted in a minor reduction in erythema compared with d-PDT. Application of BT significantly reduced post-treatment erythema and may be an easy way to make PDT in visible areas more acceptable and reduce downtime.


 Click to show fullsize
Click to show fullsize