


1Department of Dermatology, Tel Aviv Medical Center, 2Department of Human Molecular Genetics & Biochemistry, Sackler Faculty of Medicine, Tel Aviv University, and 3Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Conventional treatment of cutaneous leishmaniasis often leaves permanent scars with frequent psychosocial sequelae. The aim of this study was to compare the efficacy, safety, associated pain and final cosmetic outcome of fractional carbon dioxide (CO2) laser followed by topical application of sodium stibogluconate vs. sodium stibogluconate injections for the treatment of cutaneous leishmaniasis. A total of 181 lesions (20 patients) were randomly assigned to receive intralesional injections of sodium stibogluconate (control group) or fractional CO2 laser treatment followed by topical application of sodium stibogluconate (study group). The visual analogue scale (VAS) score of the control group was much higher than that of the study group (6.85 vs. 3.5, respectively, p < 0.001). Both the patients and 2 blinded dermatologists found the final cosmetic outcome to be superior for laser-treated lesions (p = 0.001 vs. p =0.008 for controls). Fractional CO2 laser treatment followed by topical application of sodium stibogluconate is less painful and leads to a better final cosmetic outcome compared with intralesional injections of sodium stibogluconate.
Key words: cutaneous leishmaniasis; carbon dioxide; ablative fractional laser; drug delivery.
Accepted Oct 3, 2018; Epub ahead of print Oct 3, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Ofir Artzi, Department of Dermatology, Tel Aviv Medical Center, 6 Weizman Street, Tel Aviv 6423906, Israel. E-mail: ofira@tlvmc.gov.il
Cutaneous leishmaniasis is a parasitic infection that affects millions of people every year (1). Although common treatments vary in safety and efficacy, none of them addresses the disfiguring atrophic hypo- or hyper-pigmented post-inflammatory scars. The current study shows that fractional carbon dioxide (CO2) laser treatment, followed by topical application of sodium stibogluconate, is an effective, safe treatment, which is less painful and results in better final cosmesis compared with the current gold standard, intralesional injections of sodium stibogluconate.
Leishmaniasis is a parasitic infection affecting million of patients every year (1) and may manifest with cutaneous, mucocutaneous, and visceral lesions, depending mostly on the Leishmania species and the individual’s immunity (2). Leishmania major and L. tropica are the main species of parasites responsible for cutaneous leishmaniasis (CL) in the Old World (Africa, Asia and Europe), including Israel (3). CL usually develops on exposed parts of the body within a few weeks to several months following the sandfly bite, presenting as an erythematous papule that gradually enlarges in size to become a nodule (1). Multiple lesions may develop. The lesion eventually becomes a crusted ulcer with raised indurated borders (1). Although it is a self-healing disease, the lesions may persist for months to years, often leaving disfiguring atrophic hypopigmented or hyperpigmented scars. These scars may entail mental and social problems (4), thus, many patients seek treatment to remove them or, at least, to improve their cosmesis.
Despite recent advances, optimal treatment of CL remains controversial and depends on the Leishmania species and its predicted drug susceptibility, the size, number and location of the lesions, the availability of appropriate drugs and equipment, and the skills and experience of medical personnel (5). Therapeutic options include topical drug therapies, such as paromomycin and imiquimod 5%. Although relatively easy to use and potentially inexpensive, those treatments are usually reserved for ulcerative lesions of CL, since penetration is limited by intact skin (6). Intralesional injection of pentavalent antimony overcomes this obstacle and, in many places, is considered as first-line therapy for CL (7). A few injections are usually required, but injection-related pain is considered substantial, and pain may decrease patient compliance if treatment is needed for numerous lesions (7). Moreover, sedation might be required if performed on children. Some authorities recommend avoiding intralesional injection of pentavalent antimony on the face and below the knee due to excess risk of complications (6). Oral systemic therapies, such as azoles, azithromycin, and zinc sulphate, have proven beneficial in several studies, but evidence for efficacy was inconclusive in others (8). Miltefosine is a relatively novel agent that was used mainly for visceral leishmaniasis and is now also used for CL, with proven efficacy in both New World and Old World CL (7). Side-effects include teratogenicity and gastrointestinal symptoms, such as vomiting and diarrhoea, which may be severe enough to prevent completion of therapy (6). Intravenous systemic drugs, such as pentavalent antimonial sodium stibogluconate (PASSG, Pentostam™) and liposomal amphotericin B, are also used in the treatment of CL. Since prolonged inpatient treatment may be needed for as long as 20 days, considerable expense is added to the cost of the drug itself (8). Side-effects may be severe, with reports of hepatotoxicity and renal toxicity in patients treated with amphotericin B and pancreatitis and cardiotoxicity in patients treated with pentavalent antimonials (8). Physical therapies, such as cryotherapy, localized controlled heat, photodynamic therapy, and CO2 laser, have shown various levels of effectiveness in different studies (7). Laser treatment for CL was described as an effective ablative therapy in the 1990’s, but scar formation was prominent (9, 10). Although treatments vary in safety and efficacy, none of them addresses the scarring that persists after the active leishmaniasis lesion heals.
Fractional ablative CO2 lasers had been recognized as being effective treatment for scars long before they were used for CL lesions (11). Fractional lasers create microscopic columns of tissue destruction, which result in a wound-healing response and ultimately in dermal remodelling. They are believed to increase the deposition of collagen through the upregulation of heat-shock proteins (12). In addition, the channels created by the ablative fractional CO2 laser allow deeper penetration and greater bioavailability of topically applied medications (13).
Fractional ablative CO2 laser is an effective treatment for cutaneous atrophic scars resulting from CL (14). Furthermore, the use of laser-assisted drug delivery for leishmaniasis was published in one case report treating recalcitrant active Leishmania lesion with fractional ablative CO2 laser followed by topical paromomycin with good clinical and aesthetic outcome (15).
The aim of this study was to assess the efficacy, associated pain, number of treatments required and final aesthetic outcome of a similar therapeutic approach consisting of fractional CO2 laser followed by immediate application of topical PASSG compared with intralesional injection of PASSG, a conventional first-line therapy, for active CL. Our aim was not only to cure the disease, but also to improve the patient’s skin texture and to achieve optimal resolution of the scar with minimum downtime and complications.
This open-label prospective, interventional, randomized controlled study was conducted at the Department of Dermatology, Tel Aviv Medical Center, between April 2014 and May 2017. The study was approved by our Institutional Research Ethics Board, and written informed consent was obtained from all patients.
The study enrolled 20 patients, older than 18 years and younger than 60 years, with a positive Leishmania PCR test, skin scraping with evidence of presence of parasites, or a skin biopsy diagnostic for CL. Patients were eligible if they were otherwise healthy and had several CL lesions. Patients were excluded if they had received treatment for CL, had undergone radiation therapy in the past, had a history of abnormal scarring, were immunodeficient, or if they were believed to have been infected outside of Israel.
All lesions were numbered. Odd-numbered lesions for each patient were assigned to the study group (fractional CO2 laser treatment followed by topical PASSG), and even-numbered lesions of each patient were assigned to the control group (intralesional injections of PASSG). Both the treatment and control lesions were first cleaned with 70% isopropyl alcohol. Each patient wore opaque glasses during laser treatment. The study group lesions were treated with fractional ablative CO2 laser (Ultrapulse; Lumenis, Santa Clara, CA, USA; Deep Fx handpiece) with fluence ranging from 15 to 100 mJ and density range 3–5%. Laser treatment was followed by the immediate topical application of PASSG. The control group lesions were injected intralesionally with PASSG. The injection continued until complete blanching of the lesion and its margins was observed. The procedure was repeated on each lesion once a month until complete healing (defined as complete re-epithelialization and flattening of induration) was achieved. The level of pain associated with the treatment of each lesion was recorded using the visual analogue scale (VAS) method (range 1–10). Following treatment, all patients were instructed to apply moisturizer and sunscreen 3 times a day and to avoid sun exposure.
Side-effects or drug-related complications were recorded at the monthly follow-up visits. Both the treated and control lesions were photographed with a digital camera (Canon EOD 70D) using a 100-mm macro objective and a flash (Canon Macro 100 mm) under identical lighting and patient positioning conditions at baseline during the follow-up visits and 6 months following the last treatment. The final cosmesis of the scars was scored by the patient and 2 dermatologists who were unaware of the treatment protocol. The final cosmesis score for each treatment modality was evaluated using a 1–5 Likert scale (1=worst aesthetic results, 5=best aesthetic results) based on colour (redness or hyperpigmentation), depth, texture and atrophy, and general appearance of the scar. In addition, an integrated physicians’ and patients’ score was calculated as the mean of the 4 parameters.
Differences between the 2 treatment groups were tested using the Wilcoxon paired test for all ordinal measurements and the Fisher’s exact test for categorical measurements. Mixed models were applied to enable adjustment for the variability in the number of lesions, their size and location, and the age and sex of the participants. These models were used to evaluate the differences in duration, pain and efficacy of treatment as evaluated by the 2 physicians and adjusted to the 4 selected parameters. Significance was defined at p = 0.05. Analyses were carried out using SPSS 24.01 software.
All infections were acquired in areas of Israel endemic for L. major. L. major species were confirmed by PCR. Nineteen out of 20 patients (9 males and 10 females) with a total of 178 lesions completed the study. One patient (with 6 lesions) was dropped from the study because both the study and control lesions failed to respond to treatment. The mean age of the patients was 27.3 ± 9.82 years (range 19–47 years). The majority of the lesions (68%) were on the upper limbs and the others were on the lower limbs (20.2%), head and torso (11.8%).
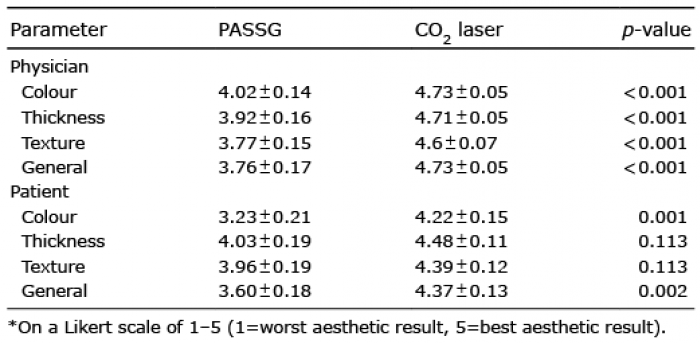
The integrated physicians’ and patients’ scores at 6 months following the last treatment were significantly higher for the lesions treated by laser followed by the topical application of PASSG compared with the intralesional injections of PASSG (4.7 ± 0.2 vs 3.9 ± 0.7, p = 0.001 and 4.4 ± 0.2 vs. 3.9 ± 0.8, p = 0.008, respectively). Comparison of the 4 selected parameters revealed that lesions treated by laser and topical application of PASSG received significantly higher scores compared with those treated with intralesional injections of PASSG according to both the physicians’ and patients’ evaluations (Table I, Figs 1 and 2).
Table I. Patients’ and physicians’ scoring* of the efficacy of injected pentavalent antimonial sodium stibogluconate injection (PASSG) vs. carbon dioxide (CO2) laser followed by topical PASSG
Fig. 1. Leishmaniasis scars, physicians’ and patients’ scores for lesions treated by laser followed by the topical application of pentavalent antimonial sodium stibogluconate (PASSG) compared with intralesional injections of PASSG at 6 months following the last treatment. IL: intralesional.
Fig. 2. Representative leishmaniasis scars (a, c, e) before, and (b, d, f) after treatment. Fractional ablative carbon dioxide (CO2) laser followed by application of pentavalent antimonial sodium stibogluconate (PASSG) (pairs: a, b and c, d) and intralesional PASSG injection (pair: e, f).
There was no significant difference in the number of sessions required until complete healing (3.1 ± 0.9 for the study group vs. 2.8 ± 0.9 for the control group, p = 0.272). Lesions > 1 cm required a significantly higher number of sessions compared with lesions < 1 cm (3.1 ± 0.8 vs. 2.4 ± 1.0, respectively, p = 0.002). In general, more pain was associated with the intralesional PASSG injections compared with the laser treatment and topical application of PASSG (VAS 6.8 ± 1.6 vs. 3.9 ± 0.7, respectively, p < 0.001). This difference was more pronounced in lesions > 1 cm (VAS 7.1 ± 1.5 vs. 3.9 ± 1.8) compared with lesions <1 cm (VAS 5.7 ± 1.7 vs. 4.2 ± 2.0).
A mixed model was used to assess the contribution of lesion size and location and patient age and sex to the final treatment cosmesis. Better cosmetic results were observed for lesions located on the head/abdomen/back areas, followed by those on the hands and then on the legs (4.8 ± 0.3, 4.4 ± 0.7, 4.1 ± 0.7, respectively (p = 0.037). Smaller lesions (< 1 cm) resulted in better aesthetic outcome compared with lesions >1 cm (an advantage of 0.6 ± 0.11, p < 0.001).
With the exception of the lesions of the single patient who was dropped from the study, the lesions of all the other study patients were completely healed following treatment. The number of required treatments was not significantly higher in the study group compared with the control group, suggesting that our proposed treatment protocol is effective. The treatment-associated pain was graded in the study group as being 43% less than in the control group (VAS: 6.8 ± 1.6 vs. 3.9 ± 0.7, respectively, p < 0.001). The difference increased to 54% when we compared only lesions > 1 cm. These data demonstrate the superiority of the study treatment over the control treatment. As mentioned earlier, intralesional PASSG is considered a powerful first-line therapy whose major drawback is significant pain. By having similar effectiveness with major reduction in associated pain, our proposed treatment will help increase adherence to treatment, lower patient pain levels and possibly provide an alternative and non-sedated trea-ment for the paediatric population. Last, but not least, the final cosmetic outcome of the study treatment was considered superior both subjectively by the patients and by the objective dermatological assessment. Leishmania lesions heals with scarring, and their occurrence on exposed skin areas together with the increasing incidence of the disease cause considerable burden on growing numbers of patients. This burden sometimes also has psychological implications. An alternative Leishmania treatment that minimizes scars will alleviate that element of the burden and should be offered to patients.
There was secondary infection of one lesion each in the study group and the control group. The patient who dropped out of the study had 6 lesions, 2 of which showed no evidence of healing by the fourth treatment. She was referred to alternative treatment, and her data were not included in the statistical analysis. An intention-to-treat analysis was performed to validate the results of this study. Because no final outcome assessment was carried out on the excluded patient, we re-did the statistical analysis, giving a score of 1 (worse) to her study lesions and score of 5 (best) to her control lesions in all parameters, and the level of significance for the entire cohort did not change (Table II).
Table II. Patients’ and physicians’ scoring*: intention-to-treat analysis
We speculate that fractional CO2 will have a triple effect when applied to the treatment of active CL: (i) its thermolysis effect might contribute to elimination of the parasites from the skin; (ii) the channels created might allow deeper penetration and greater bioavailability of the applied PASSG (referred to as laser-assisted drug delivery) (8); and (iii) the multiple columns of epidermal and dermal microscopic thermal wounds (micro-thermal zones) are likely to lead to dermal remodelling and thereby mediate an anti-scarring effect within a few months.
Regardless of the mechanisms of action of this new therapeutic modality, fractional CO2 laser followed by topical application of PASSG (Fig. 3) was found to be superior to intralesional injections of PASSG based on several parameters. Treatment-associated pain was less intense when laser was used prior to application of PASSG. Laser-assisted delivery of PASSG was even more beneficial when the results of treatment of lesions >1 cm size and lesions located in the centre of the body and upper limbs were compared.
Fig. 3. Active cutaneous leishmaniasis. Fractional ablative carbon dioxide (CO2) laser followed by pentavalent antimonial sodium stibogluconate (PASSG) application. (a) Before treatment, (b) after 2 treatments, (c) 6 months after last treatment.
The limitations of this study include the division of lesions into study and control groups. After the lesions were numbered, the odd-numbered ones were assigned to the study group and the even-numbered ones to the control group. This method might include selection bias by the treating investigator. In addition, the sample size is relatively small, and understanding of the mode of action of this new treatment modality is incomplete. Another important limitation is the systemic effect of the intralesional injections of PASSG. One patient had 26 lesions. The mean number of lesions per patient was 9.4. Each lesion assigned to the control group was injected with 1.2–3.1 ml (mean 1.8 ± 0.6 ml) PASSG per lesion depending on its size and until blanching. Our study used Pentostam™ 100 mg/ml. Systemic PASSG treatment is given at a dose of 20 mg/kg per treatment (8), meaning that a patient with multiple lesions might have had a systemic effect on both the studied and control lesions, introducing a bias on the study. This limitation, however, might cause the study group to be as effective as the control group, but cannot explain the superior results of the lesions in the study group.
In spite of these limitations, these results demonstrate the remarkable advantages of laser-assisted drug delivery for the treatment of CL.
Esther Eshkol is thanked for editorial assistance.
Reviewed and approved by IRB; approval #TLV-14-0371 NIH registry #NCT03009422.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize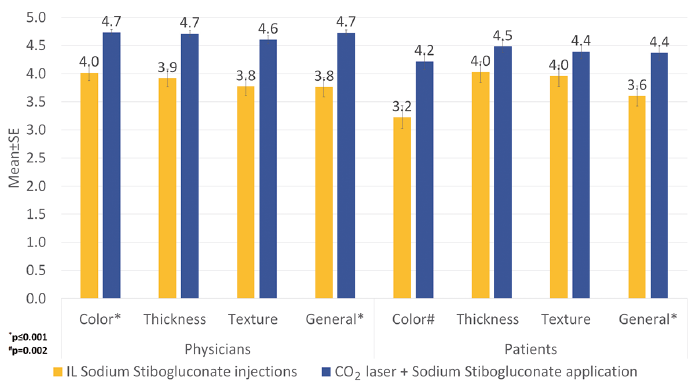 Click to show fullsize
Click to show fullsize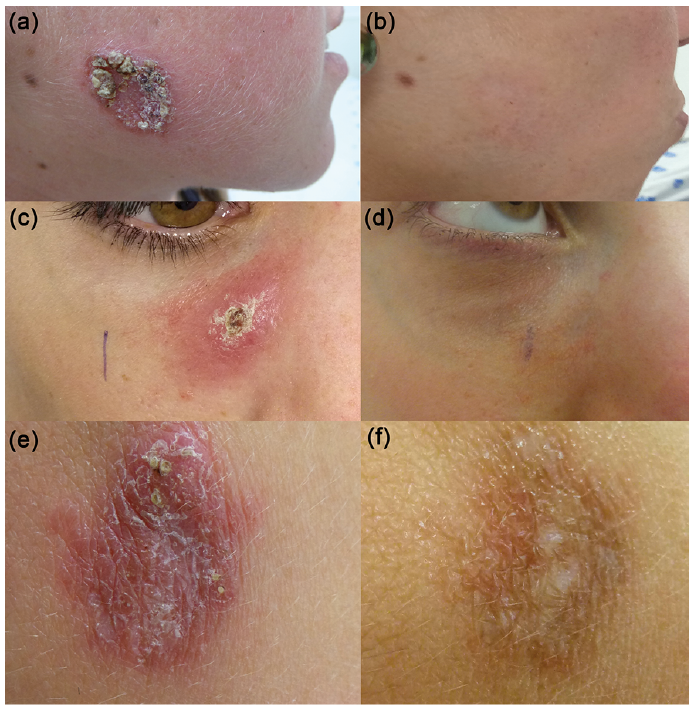 Click to show fullsize
Click to show fullsize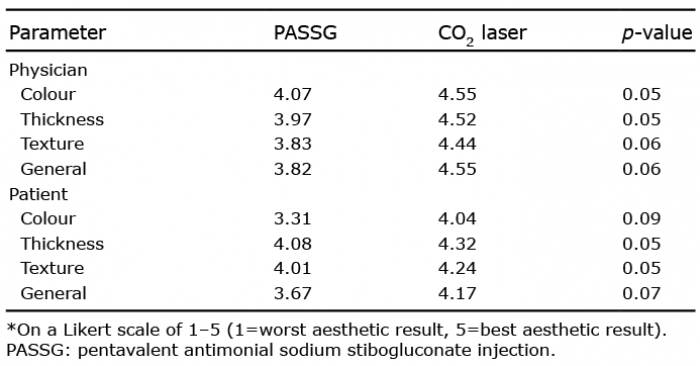 Click to show fullsize
Click to show fullsize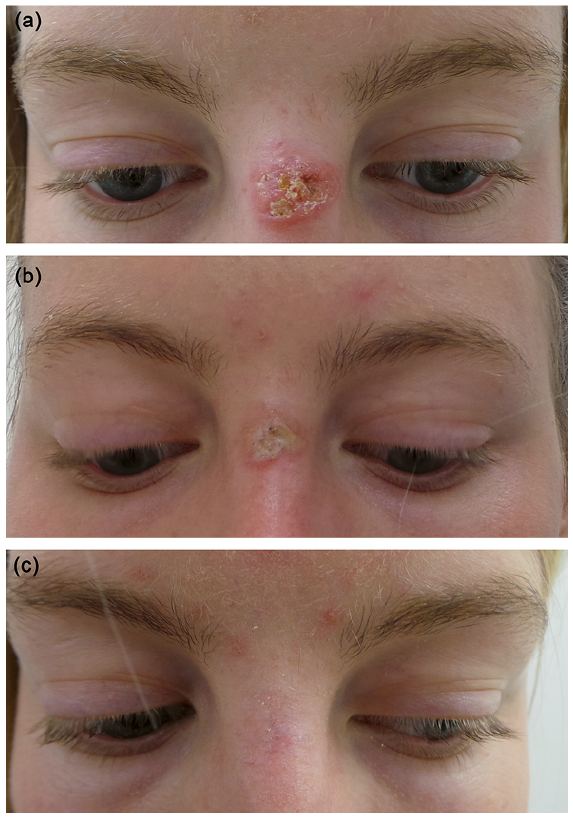 Click to show fullsize
Click to show fullsize