


Department of Dermatology, Ehime University Graduate School of Medicine, Toon, Ehime, Japan. E-mail: kshira@m.ehime-u.ac.jp
Accepted Oct 3, 2018; Epub ahead of print Oct 3, 2018
Vemurafenib, an oral BRAF kinase inhibitor, has been approved for the treatment of late-stage metastatic malignant melanoma. Although vemurafenib prolongs progression-free and overall survival, numerous cutaneous side-effects have been reported (1, 2). We present here a case of perforating folliculitis (PF) associated with vemurafenib. To the best of our knowledge, this is the first report of vemurafenib-associated PF.
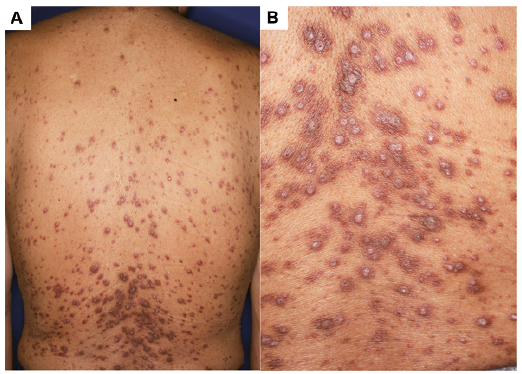
A 62-year-old man was treated with vemurafenib (960 mg twice daily) for metastatic malignant melanoma. Two months after initiating therapy, numerous disseminated keratotic follicular papules developed on his scalp, face, trunk and legs (Fig. 1A, 3A). Each papule contained a central, cone-shaped, keratotic plug (Fig. 1B). Differential diagnoses included a perforating disorder, suppurative folliculitis, hyperkeratotic folliculitis, and keratosis pilaris. Histopathological examination showed a dilated follicular infundibulum filled with a mixture of keratotic material, basophilic debris and inflammatory cells (Fig. 2A). The follicular epithelium showed a perforation through which degenerated collagen fibres entered into the follicular cavity (Fig. 2B). The follicles were surrounded by inflammatory infiltrate, mainly comprising lymphocytes. Elastic Masson and Azan staining revealed invasion or penetration of collagen fibres into the follicular epithelium (Fig. 2C, 2D). A diagnosis of PF was established. Because of the clinical efficacy against metastatic melanoma, vemurafenib was maintained at the same dosage. Combined treatment with topical corticosteroid ointments and antibiotic ointments (nadifloxacin) did not improve the folliculitis. We initiated minocycline at 100 mg/day, but the skin lesions did not disappear (Fig. 3B). After vemurafenib was discontinued and changed to nivolumab due to tumour recurrence, follicular papules rapidly began to improve. One month after stopping vemurafenib, the skin lesions disappeared with residual pigmentation (Fig. 3C). We concluded that PF was a cutaneous adverse drug reaction due to vemurafenib.
Fig. 1. (A) Numerous disseminated keratotic follicular papules on the trunk. (B) Each papule contained a central, cone-shaped, keratotic plug.
Fig. 2. (A) Dilated follicular infundibulum filled with a mixture of keratotic material, basophilic debris and inflammatory cells. Haematoxylin and eosin staining; original magnification ×40. (B) Degenerated collagen fibres enter the follicular cavity through the follicular epithelium. Haematoxylin and eosin staining; original magnification ×100. (C) Elastic Masson staining reveals invasion or penetration of collagen fibres (green); original magnification ×200. (D) Azan staining detects collagen fibres (blue) invading into the follicular cavity; original magnification ×200.
Fig. 3. Keratotic follicular papules on the face and buttocks (A) at 2 months and (B) 7 months after initiating vemurafenib treatment. (C) Skin lesions disappeared with residual pigmentation 1 month after stopping vemurafenib therapy.
Vemurafenib is a small molecule that belongs to the group of protein kinase inhibitors. The drug has been approved for the treatment of metastatic melanoma harbouring the BRAF mutation. Although vemurafenib prolongs progression-free and overall survival, numerous cutaneous side-effects, including photosensitivity, alopecia, xerosis, squamous cell carcinoma, keratoacanthomas, palmar-plantar keratoses, and keratosis pilaris-like eruptions, have been reported (1, 2).
Acquired perforating dermatosis is an uncommon cutaneous perforating disorder characterized by transepidermal elimination of dermal tissue materials, such as keratin, collagen and elastic fibres. PF is an acquired perforating dermatosis together with Kyrle disease, reactive perforating collagenosis and elastosis perforans serpiginosa (3). PF is characterized by asymptomatic to severe pruritic keratotic follicular papules with disruption of the infundibular follicular wall. These skin lesions appears more frequently in patients with severe renal insufficiency, poorly controlled diabetes mellitus or arterial hypertension, as well as in sclerosing cholangitis (4). Scratching and deficiency of bile acids or vitamin A have been considered as possible causes (5). In this case, asymptomatic lesions and absence of excoriations ruled out chronic scratching as a causal factor. During vemurafenib therapy, PF developed gradually (Fig. 3A, B) and did not disappear with any treatments, including corticosteroid ointments, antibiotic ointments, and minocycline. After discontinuing vemurafenib, the skin lesions improved rapidly (Fig. 3C). We therefore concluded that the PF skin lesions were a cutaneous adverse drug reaction to vemurafenib.
The pathogenesis of PF induced by vemurafenib remains unknown. Interestingly, some cases of PF associated with sorafenib, another Raf kinase inhibitor, have been reported (3, 5–7). Sorafenib inhibits not only Raf-1 kinase, but also vascular endothelial growth factor receptor (VEGFR) 2, VEGFR3, platelet derived growth factor (PDGF) receptor and c-kit (3, 7). Some authors suggest that the pathogenic mechanisms could be explained by a possible direct toxic effect on follicular cells due to the inhibition of Raf and other kinases, and an indirect effect due to c-kit inhibition (5, 8). Inhibition of the PDGF receptor by sorafenib could also play a role in the pathogenesis of PF (3). Furthermore, a previous report suggested that EGFR blockade increases expression of proinflammatory chemokines and p27kip, a negative growth regulator that enhances apoptosis and promotes keratinocyte differentiation. This may lead to a thin stratum corneum and inflammatory infiltration of the follicles, resulting in dilation and plugging by excessive keratin (9). Moreover, our patient had chronic renal insufficiency, diabetes mellitus and arterial hypertension. This background may also have supported or promoted the development of PF by vemurafenib.
In conclusion, we have described vemurafenib-associated PF for the first time. Alterations in keratinocyte differentiation and/or proliferation pathways induced by vemurafenib could induce PF. This observation is important for elucidating the pathogenesis of PF, which remains unknown. Further prospective studies are needed to clarify the precise mechanisms.


 Click to show fullsize
Click to show fullsize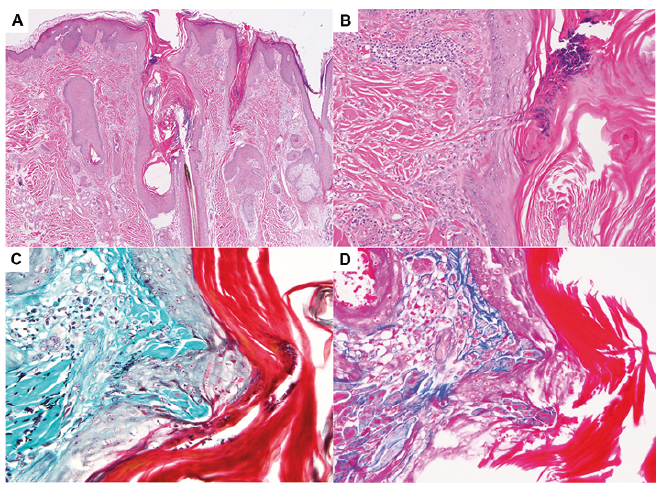 Click to show fullsize
Click to show fullsize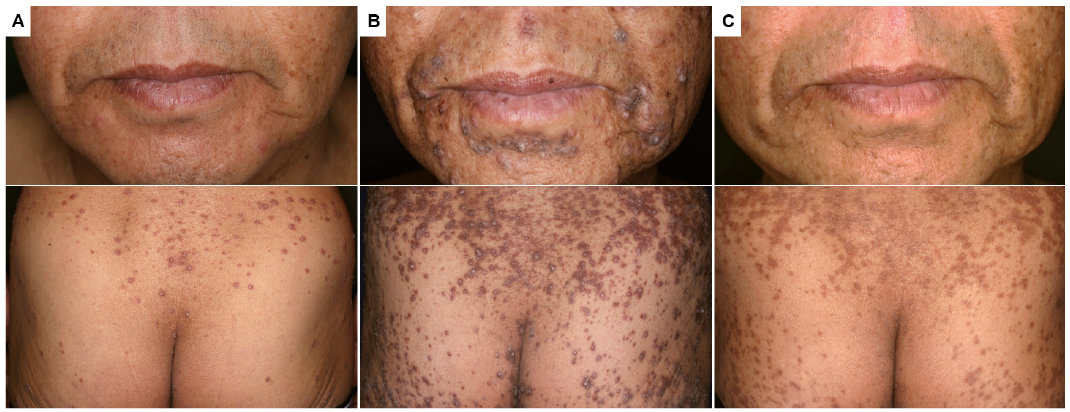 Click to show fullsize
Click to show fullsize