


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wrocław, Poland
Subjective symptoms accompanying atopic dermatitis and psoriasis can negatively influence patients’ well-being. This study assessed the impact of itch and pain on sleep quality among 100 patients with atopic dermatitis and 100 patients with psoriasis, compared with 50 controls. The Athens Insomnia Scale (AIS) and Pittsburgh Sleep Quality Index (PSQI) were used to evaluate a spectrum of sleep disturbances. Co-existence of insomnia was indicated in the majority of patients; atopic dermatitis; 82%, psoriasis; 62%. PSQI total scores for patients with atopic dermatitis (8.3 ± 4.2 points) and those with psoriasis (8.1 ± 4.8 points) qualified them, in 80% of cases, as poor sleepers and were significantly higher compared with controls (3.1 ± 1.9 points). However, subjects with atopic dermatitis experienced more problems with insomnia and sleep quality than did those with psoriasis. Atopic dermatitis and psoriasis-related itch, but not pain, has a substantial association with insomnia and sleep quality in these patients, and is a crucial subjective symptom in these chronic, inflammatory skin diseases.
Key words: atopic dermatitis; psoriasis; itch; pain; quality of life; sleep; visual analogue scale.
Accepted Oct 11, 2018; Epub ahead of print Oct 11, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Chałubińskiego 1, PL-50-368 Wrocław, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Atopic dermatitis and psoriasis are chronic, inflammatory and debilitating skin conditions. As skin conditions can affect sleep activity, it is possible that such dermatoses can disturb sleep quality. Moreover, atopic dermatitis- and psoriasis-related subjective symptoms may worsen sleep disturbances. In this study, we demonstrate that patients with atopic dermatitis experience far more problems with insomnia and sleep quality than those with psoriasis. We show that atopic dermatitis and psoriasis-related itch, but not pain, has a substantial association with insomnia and sleep quality, and is a crucial subjective symptom in these two chronic inflammatory diseases.
Atopic dermatitis (AD) and psoriasis (Ps) are chronic, inflammatory and debilitating skin diseases. Their pathogenesis, however distinct, is multifactorial and encompasses a hyperactive immune system, environmental factors and genetic predisposition (1). The mean prevalence of AD in the general population worldwide ranges from 2.1% to 4.9% (2). The disease is characterized by erythema, lichenified lesions and accompanied by severe itch, which is an essential symptom of AD. Itch is such a “crucial”, symptom that Romeo (3) described AD as “the itch that rashes”. It negatively influences different aspects of well-being in patients with AD (4). Skin lesions in Ps are typically scaly plaques that cover the scalp, elbows and knees, but nails and any other skin area can be also affected (5). The prevalence of psoriasis in adults worldwide ranges from 1% to 3% (6). Itch is a problem for approximately 60–90% of adults with psoriasis, and similarly to AD, is often characterized as the most burdensome symptom of the disease (7). Not only itch, but also pain in the lesioned skin, is a frequently reported accompanying symptom, resulting in profound burden due to the course of these diseases (8, 9).
Sleep is a fundamental, restorative, physiological, neurobiological state that engages approximately one-third of our lives. Sleep is carefully regulated by multiple processes, including homeostatic sleep drive and the circadian system (10, 11). Both itch and pain can significantly reduce the quality of life (QoL) and sleep of patients (12, 13). The aim of this study was to better characterize the influence of itch and pain on sleep in patients with AD and Ps.
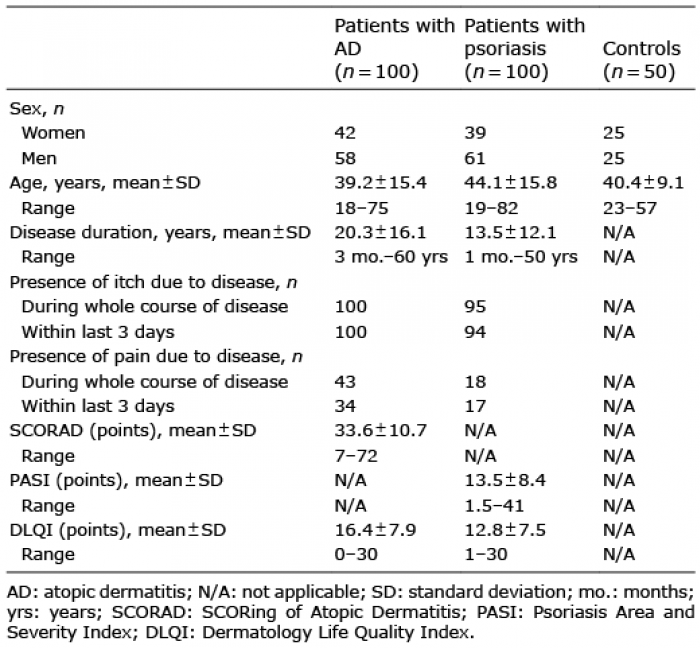
The study was conducted among Caucasians with AD (n = 100), with plaque Ps (n = 100) with no involvement of the joints, and 50 sex- and age-matched healthy controls (detailed characteristics are shown in Table I). AD diagnosis was made according to well-established Hanifin & Rajka criteria (14), while Ps diagnosis was based on clinical manifestation (in doubtful cases biopsies were taken). The mean duration of disease was assessed as 20.3 ± 16.1 years (range 3 months–60 years) and 13.5 ± 12.1 years (range 1 month–50 years) for AD and Ps, respectively. Disease severity was evaluated with SCORing of Atopic Dermatitis (SCORAD) for AD and Psoriasis Area and Severity Index (PASI) for patients with Ps (15, 16).
Table I. Characteristics of studied group
All patients and controls with any itchy/painful skin condition of any type or receiving any antipruritics, or pain-killers (e.g. antihistamines, immunomodulators/immunosuppressants, etc. (> 5 half-lives washout period)) were excluded. None of the patients or controls had a known primary psychological disorder or disease of any type that might have influenced sleep quality (e.g. obstructive sleep apnoea). Only over-the-counter (OTC) sleep drugs were allowed.
The intensity of itch and pain was evaluated with a VAS (visual analogue scale) as the mean symptom experienced within the last 3 days (VASmean) and at the time of examination (VASexam).
The VAS is a 10-cm long line, in our study oriented horizontally, on which patient assessed the intensity of subjective symptoms by marking the line vertically at the point corresponding to the severity of itch or pain. Scores ranged from 0 (no itch/pain) to 10 points (worst itch/pain imaginable). Itch VAS scoring was categorized as mild (> 0–< 3 points), moderate (≥ 3–< 7 points) and severe or very severe itch (≥ 7–10 points) (17). The respective cut-off points for pain (≤ 5; > 5–7; > 7–10) could be distinguished (18).
To assess a spectrum of sleep disturbances, all patients and controls were asked to complete the validated version of multiple self-assessment questionnaires, including the Athens Insomnia Scale (AIS) and Pittsburgh Sleep Quality Index (PSQI). Moreover, quality of life was evaluated with the Dermatology Life Quality Index (DLQI).
The AIS is a self-rated psychometric questionnaire quantifying sleep difficulty, based on International Classification of Diseases – 10th edition (ICD-10) criteria, over the previous month. AIS consists of 8-items: sleep induction, waking during the night, final awakening, total sleep duration, sleep quality, well-being, functioning capacity, and sleepiness during the day. The questionnaire uses 8 items, based on a 0–3 scale, in which “3” designates negative outcomes. Total AIS scores range from 0 to 24 points. A total score of ≥ 6 points reflects a diagnosis of insomnia (19, 20).
The PSQI is a self-rated questionnaire assessing sleep quality and disturbances over an interval of the 4 previous weeks. PSQI is an instrument evaluating 7 domains of sleep quality: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleeping medication, and daytime dysfunction. The questionnaire uses 14 questions, based on a 0–3 scale (where 3=negative outcome), and 4 open-ended questions. PSQI scores range from 0 to 21 points. A global score ≥ 5 reflects a specific and sensitive measure of poor sleep quality (21, 22).
The DLQI is a self-assessment psychometric instrument designed to estimate the impact of a skin disease on the patients’ life over the previous week. DLQI is using to assess the 6 particular aspects of the patients’ life, including symptoms and feelings, daily activities, leisure, work and school, and personal relationships. The questionnaire uses 10 questions based on a scale of 0 to 3. DLQI scores range from 0 to 30 points, with higher scores indicating worse QoL (23).
The study was approved by the ethics committee of Wroclaw Medical University (number KB – 455/2017). Informed written consent to participate in the study was obtained from all individuals studied.
All variables were assessed for normal or non-normal distribution, in order to apply corresponding parametric or non-parametric statistical tests. Pearson’s χ2 test was applied to sets of categorical data. Differences between groups were determined using the Mann–Whitney U test and Kruskal–Wallis test or Student’s t-test with reference to the distribution of evaluated variables (non-normal or normal, respectively). Correlations were determined using Spearman’s correlation analysis. The level of significance was set at α=0.05. The resulting p-values were considered significant if p < 0.05. Statistical analyses were performed using Statistica 12 software (StatSoft, Tulsa, OK, USA).
The sample size of the study cohort was determined by sample size calculation using the principle of the anticipated response distribution of 50%, with 95% confidence interval (CI) and 10% precision.
Itch was present permanently among every patient with AD. Itch intensity was assessed as 7.1 ± 2.7 points and 3.4 ± 2.7 points (for VASmean and VASexam, respectively). Pain severity was estimated as 5.3±2.9 points and 2.8 ± 2.9 points (for VASmean and VASexam, respectively). Moreover, according to the cut-offs for VASmean, 60% of patients with AD reported having severe-to-very severe itch (Fig. 1). In contrast to itch, AD-related pain was reported by “only” 43% and 34% of patients, during the whole course of disease and within the last 3 days, respectively. Moreover, pain was distributed equally, among patients reporting this symptom, in the terms of its intensity.
Fig. 1. Atopic dermatitis (AD) and psoriasis (Ps)-related itch and pain intensity rates. The diagrams were based on cut-off established for visual analogue scale (VASmean) values; (A) AD-linked itch intensity, (B) AD-linked pain intensity, (C) Ps-linked itch intensity, and (D) Ps-linked pain intensity.
The mean AIS score among patients with AD was assessed as 10.5 ± 5.5 points (range 0–23), whereas controls scored significantly lower (p < 0.0001) (Table II). Moreover, the results indicate the co-existence of insomnia in 82% of patients with AD (AIS ≥ 6). Furthermore, patients with AD significantly more commonly reported problems with falling asleep, waking during the night, sleep quality, well-being and functioning capacity, compared with the controls (Table III). However, no significant differences between patients with AD and controls were found according to final awakening, total sleep duration, and sleepiness during the day.
Table II. Athens Insomnia Scale (AIS) and Pittsburgh Sleep Quality Index (PSQI) total scores among atopic dermatitis (AD), psoriatic (Ps) patients and controls
Table III. Athens Insomnia Scale (AIS) items among atopic dermatitis (AD), psoriatic (Ps) patients and controls
The mean PSQI score among this group of patients was assessed as 8.3 ± 4.2 points (vs. controls, p < 0.0001). Eighty percent of patients with AD, but only 22% of controls were classified as poor sleepers (PSQI ≥ 5) (p < 0.0001). Patients with AD, on average, were more severely affected in all PSQI domains in comparison with controls (Table IV).
Table IV. Pittsburgh Sleep Quality Index (PSQI) domains among atopic dermatitis (AD), psoriatic (Ps) patients and controls
Severity of itch (VASmean) correlated significantly with the scores obtained by AIS (r=0.44, p < 0.0001), but not with PSQI (r=0.21, p = 0.09). Moreover, the pain intensity, its presence, disease duration or SCORAD scores did not correlate with the results obtained with AIS or PSQI. Nonetheless, both itch and pain intensity impacted independently on the DLQI results (r=0.45, p < 0.0001 and r=0.36, p = 0.026, respectively).
Itch and pain were experienced by most patients with Ps during the entire course of disease (95% and 18%, respectively). The respective symptoms were reported by 94% and 17% of subjects with Ps during the 3 days immediately before examination.
The mean itch and pain intensity (VASmean) were assessed, among patients reporting these symptoms, as 6.6 ± 2.6 points and 7.3 ± 2.8 points, respectively (VASexam, 2.8 ± 2.7 points for itch and 1.8 ± 2.3 points for pain). Moreover, according to the cut-offs for VASmean, the majority of patients with Ps reported itch of at least moderate intensity (87%). Pain, if any, was predominantly severe (11%) (Fig. 1).
The mean AIS score among patients with Ps was assessed as 7.4 ± 5.2 points (range 0–20) whereas controls scored 5.5 ± 3.4 points (range 0–14 points) (Table II). No statistical differences in AIS mean total scores received by patients with Ps and controls were revealed, but subjects with Ps significantly more commonly reported problems with final awakening (p = 0.04) compared with controls. The mean scores for PSQI were 8.1 ± 4.8 points (range 0–16) and 3.1 ± 1.9 points (range 0–7) for patients with Ps and control subjects, respectively (p < 0.0001). Eighty percent of patients with Ps were classified as poor sleepers (p < 0.0001). Patients with Ps, on average, had more severely affected sleep quality with regard to sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances and use of sleeping medications compared with controls (Table IV).
The severity of itch (VASmean) was significantly correlated with AIS and PSQI scores (r=0.34, p < 0.001 and r=0.59, p < 0.001, respectively). Pain intensity, PASI and disease duration had no influence on AIS and PSQI results. Moreover, in most patients, for the above-mentioned factors, i.e. itch and pain severity, the PASI scores correlated significantly with DLQI outcomes.
Direct comparison of patients with AD and those with Ps revealed no significant differences in intensity of itch (VASmean). Furthermore, patients with AD reported disease-related pain during the last 3 days twice as often as did patients with Ps, but Ps patients reported its intensity as significantly higher (p < 0.01). Moreover, significant differences were found between these 2 groups in terms of total AIS score and its specific items, but not in terms of PSQI. Patients with AD scored higher on all of the AIS items, except for final awakening and sleepiness during the day. With regard to the PSQI, patients with Ps scored significantly higher for sleep duration (i.e. shorter sleep), but patients with AD scored significantly higher for sleep disturbances (i.e. more trouble sleeping) (Tables III and IV).
Severity of itch (VASmean) correlated significantly with pain intensity (VASmean) among patients with AD and those with Ps (r = 0.45, p < 0.01 and r = 0.49, p =0 .04, respectively). It is notable that, in both diseases, AIS, PSQI, itch and pain scores were independent of the sex and age of the patients (detailed data not shown).
AD and Ps have a major impact on health-related QoL (4, 24). In concordance with previous studies, our data indicate that itch and pain of moderate-to-severe intensity are frequent among patients with these conditions (4, 7, 25, 26). These symptoms, but also other issues, including cognitive and somatic arousal, mood, depression and anxiety, have a potential impact on sleep quality (27, 28).
A negative influence of itch on sleep quality is seen in chronic inflammatory skin diseases such as AD and Ps (29–31). Moreover, pain, like itch, impacts negatively on sleep quality in psoriatic arthritis (PsA) (32).
The association with AD and Ps-related subjective symptoms is reflected in the results seen with AIS and PSQI. With reference to AIS scores, the co-existence of insomnia was suggested in the vast majority of patients with AD (82%) and those with Ps (62%). Furthermore, patients with AD more commonly reported problems with falling asleep, waking during the night, sleep quality, well-being and functioning capacity, compared with controls, but problems with final awakening were reported more frequently by subjects with Ps. To the best of our knowledge, the AIS has not been used previously in studies of dermatoses. Nonetheless, mean AIS scores found for individuals with AD and Ps (10.5 points and 7.4 points, respectively) were significantly higher than these for patients with hidradenitis suppurativa (HS) (5.4 points) (33).
In the current study, PSQI total score for patients with AD (8.3 points) and with Ps (8.1 points) was comparable to the results of other studies (27, 34–39), but significantly higher than controls, and higher than the general healthy German or Austrian normative populations (5.0 and 4.5 points, respectively) (40, 41). Moreover, PSQI total score was surprisingly higher among our subjects with AD and Ps than in the recently studied patients with HS (6.5 points) (33).
In available published data, AD significantly affected subjective sleep quality and daytime dysfunction compared with controls (34), but Ps, in addition to these effects, also impacted on habitual sleep efficiency (35, 42). In our study, the results for patients with AD indicated significant involvement of all domains of the PSQI. In subjects with Ps significant associations with sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances and use of sleeping medication were revealed, but, in contrast to the study by Malikoglu (35), there was no link with subjective sleep quality and daytime dysfunction domains.
Furthermore, since they are chronic skin conditions, AD and Ps could have a similar, or even a more major, effect on sleep quality than severe systemic conditions, including chronic obstructive pulmonary disease (COPD), Hodgkin’s (HL) and non-Hodgkin’s (NHL) lymphomas, or systemic lupus erythematosus (SLE). For instance, previous researchers have reported a total PSQI score of 6.0 points in patients with COPD (43). Moreover, in a large study from a population-based German regional cancer registry, involving 515 long-term survivors of HL and NHL, mean PSQI scores of 5.8 points and 6.4 points for HL and NHL, respectively, were reported (44). In addition, mean PSQI scores of 6.5 and 8.1 points were found among SLE patients without and with metabolic syndrome, respectively (45).
The current study revealed that itch, but not pain, had a substantial association with insomnia frequency and sleep quality. Itch intensity had a significant link with insomnia frequency in both AD and Ps, but also affected sleep quality among patients with Ps. Similar results were found by Jensen et al. (46) among psoriatic patients, where itch was significantly associated with all sleep-related outcomes. Such dependence was also found in the AD study, where pruritus score also significantly correlated with PSQI (38). In addition to itch acting as a crucial factor in insomnia and poor sleep quality, some authors also pointed out that disease severity (assessed with SCORAD or PASI) is also a factor. For instance, such dependence was revealed by Yano et al. (37), who demonstrated that global PSQI score was positively and significantly associated with SCORAD/DLQI scores. Significant association between PSQI domains (subjective sleep quality and sleep latency) and SCORAD in patients with AD was also shown by Kong et al. (38). Melikoglu (35) has found such correlation among patients with Ps, where global PSQI and PASI scores were significantly linked. Interestingly, we found significant correlations of itch and pain with SCORAD and PASI (data not shown), but in contrast to the data mentioned above, in our study there were no significant correlations between total AIS/PSQI scores and diseases severity, their duration or pain intensity. The lack of significant correlations with diseases severity could be due to the fact that SCORAD and PASI measure parameters that may not directly affect sleep quality (e.g. the extent of skin lesions). Moreover, SCORAD could be treated as a poor measure of the severity of AD in our study, since it contains a patient-reported outcome regarding sleep in the metric itself. This is a limitation of our study. The use of a different severity measure tool (e.g. Eczema Area and Severity Index) should be considered, in order to better assess probable dependences.
Finally, with regard to AIS, direct comparison of AD and Ps revealed that insomnia is more pronounced among patients with AD. “Final awakening” and “sleepiness during the day” were the only 2 items that differed between these groups. With reference to the PSQI, our results were in agreement with those of Zachariae et al. (47), indicating longer sleep duration among patients with AD, probably caused by more frequent sleep disturbances.
Our study has some other limitations. Firstly, the study was conducted at a single-centre, which limits generalization of the results to other populations or institutions with different resources. Multicentre studies are needed in order to fully understand the relationship between sleep quality and skin-related symptoms. Secondly, the sample size was too small (the desired margin of error should be 5%), which may also limit the generalization of our findings. Finally, there was a positive correlation between itch and pain. This does not allow us to completely rule out the possibility of confusion of the symptoms experienced by the patients, which may be responsible for bias in the results.
In general, AD seems to have a greater effect on sleep than does Ps. Moreover, itch related to AD or Ps has a substantial association with insomnia and sleep quality, and acts as a crucial subjective symptom in these chronic, inflammatory skin diseases. It was previously suggested that itch-related sleep impairment could be an important mediator of the association between itch severity and psychological and somatic symptoms (47). Intervention studies on itch management could therefore be useful for improving sleep quality and QoL among patients with these conditions. Further research into objective measurements of sleep quality, using questionnaire-based epidemiological surveys over a longer period of time, are warranted in order to elucidate the nature of poor sleep in these patients.
Funding sources Research grant by Wroclaw Medical University (grant No. STM.C260.16.030).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize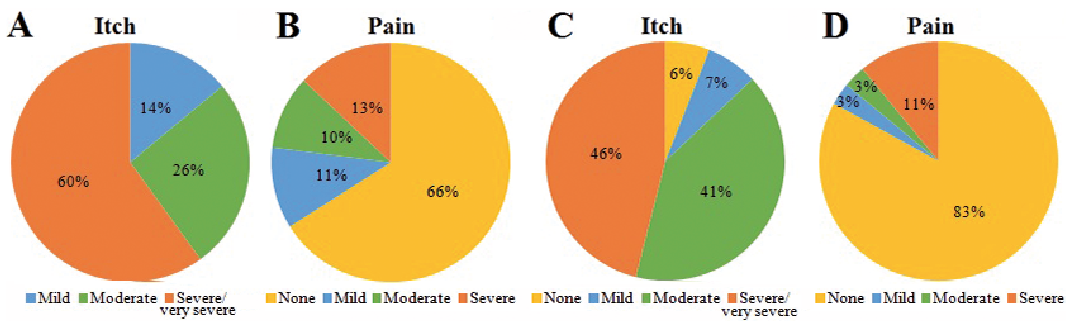 Click to show fullsize
Click to show fullsize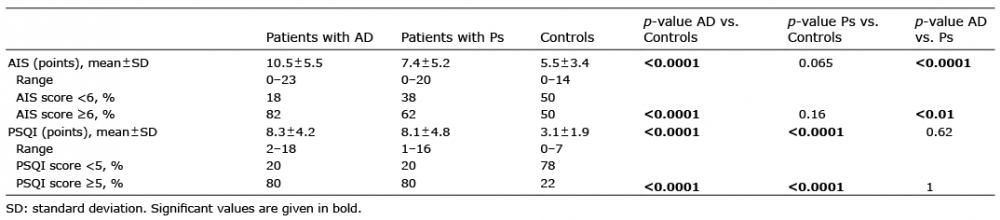 Click to show fullsize
Click to show fullsize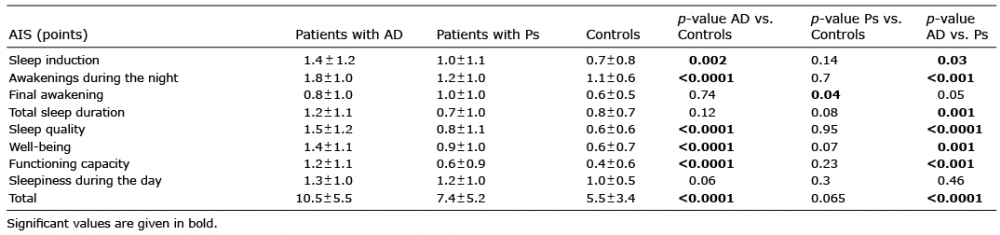 Click to show fullsize
Click to show fullsize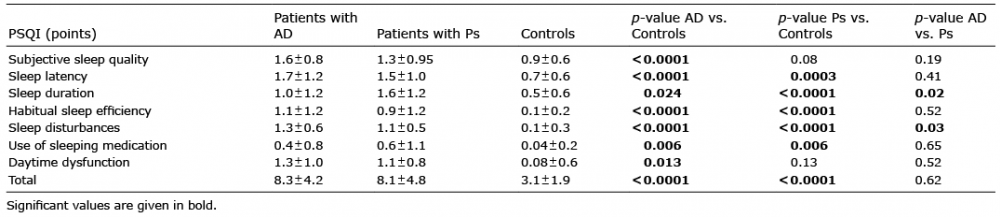 Click to show fullsize
Click to show fullsize