


1Department of Dermatology, and 2Department of Bacteriology, Hospital of Fréjus Saint Raphaël, Fréjus, France
Bacteraemias are life-threatening conditions that require rapid care and antibiotherapy. Dermatological signs might help in deciding the most relevant treatment. The aim of this study was to determine the prevalence and clinical characteristics of cutaneous manifestations in hospitalized patients with bacteraemia. A cross-sectional study was conducted over a period of 1 year. All consecutive patients with a bacteraemia (except contaminations) were included and examined by a dermatologist within 48 h after positive blood cultures. Clinical (skin manifestations, diagnosis, origin of the bacteraemia) and laboratory (bacteria) data were recorded. In total, 401 bacteraemias in 375 patients were included for the final analysis. Thirty-nine cutaneous manifestations in 34 patients were noted, corresponding to a prevalence of 9%; 69% (n = 27) were considered primary cutaneous manifestations, 18% (n = 7) as secondary ones, 10% (n = 4) as contiguous, and 3% (n = 1) as undetermined. Gram-positive cocci, specifically Staphylococcus aureus and Streptococcus species, were the most frequent bacteria (n = 27, 69%).
Key words: bacteraemia; Staphylococcus aureus; Streptococcus pyogenes; purpura fulminans; sepsis.
Accepted Oct 16, 2018; Epub ahead of print Oct 17, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Pascal del Giudice, Infectiology-Dermatology, Hospital of Fréjus Saint Raphaël, 240 Avenue de saint Lambert, FR-83600 Fréjus, France. E-mail: del-giudice-p@chi-fsr.fr
Bacteraemias are life-threatening conditions that require rapid antibiotherapy. Dermatological signs might help in deciding the most relevant treatment. The aim of this study was to determine the prevalence and clinical characteristics of cutaneous manifestations in hospitalized patients with bacteraemia. In this study 401 bacteraemias in 375 patients were included in the final analysis: 9% had cutaneous manifestations; 69% were primary cutaneous manifestations, 18% as secondary ones, and 10% contiguous. Gram-positive cocci, specifically Staphylococcus aureus and Streptococcus species, were the most frequent bacteria (69%). Thus, careful dermatological examination of septic patients provides important information to enable prescription of the most relevant probabilistic antibiotherapy.
Bacteraemias are defined as an invasion of the bloodstream by live bacteria. The diagnosis is based on positives blood cultures associated with clinical signs of infection. Recognized to be a major cause of morbidity and mortality globally, they remain a clinical and public health concern (1, 2). Rapid and appropriate antibio-therapies are required and associated with better outcomes (3). Skin lesions associated with bacteraemia have been reported in isolated case reports or short selected series (4). Those reports do not provide an overview of the characteristics of skin lesions in all causes of bloodstream infections. Furthermore, the prevalence of skin lesions in patients with bacteraemia is unknown. Better knowledge of these dermatological signs in bloodstream infections could help to initiate appropriate antibiotherapy.
The objective of this prospective, cross-sectional study was to assess the prevalence of cutaneous manifestations in patients with bacteraemia and to describe their clinical and microbiological characteristics.
This monocentric, prospective, cross-sectional study was conducted in a 500-bed general hospital covering an area of approximately 180,000 inhabitants, during a period of one year from 1 December 2013 to 30 November 2014. All patients with a bacteraemia were included. All episodes of bacteraemia for each patient were analysed. There was no age limit for inclusion in the study. Patients were excluded because of death or discharge before the dermatological examination. Contaminated blood cultures as defined afterwards were also excluded. The clinical, microbiological and epidemiological data were recorded on a standardized form. The study was approved by the local research ethics committee.
All definitions result from the Réseau d’Alerte, d’Investigation et de Surveillance des Infections Nosocomiales (RAISIN, nosocomial infection early warning, investigation and surveillance network) (5).
In the hospital, blood cultures are performed systematically for each patient presenting at least one of the following symptoms: fever > 38.0°C, hypothermia < 36°C, hypotension or chills.
A bacteraemia was defined by at least one positive blood culture. For patients presenting several bacteraemias, the different episodes were included as new episodes if the isolated microorganism was different from the previous episode or if the origin of the bacteraemia was different.
Contamination was defined as the isolation of contaminant bacteria in a single blood culture set, including the following species: Coagulase-negative staphylococci, Corynebacterium species, Bacillus species or Propionibacterium acnes. Bacter-aemias involving contaminant microorganisms were included if the contaminant bacterium was isolated from 2 or more separate blood culture sets or samples taken at different times. Bacter-aemias involving contaminant microorganisms were also included if the patient was carrying an intravascular catheter or a pros-thetic device and if an adapted antibiotherapy had been started.
Community-acquired bacteraemia was defined by positive blood culture taken within 48 h after hospital admission. Nosocomial bacteraemia was defined by positive blood culture taken 48 h after admission.
The BacT ALERT 3D system (bioMérieux Inc., Marcy L’étoile, France) for blood cultures was used with aerobic (FA), anaerobic (FN) and paediatric (PF) bottles. Blood culture bottles were placed in the routine blood culture system at any time of the day. Identification of the bacteria was performed using a phenotypic method (Vitek2 system, BioMérieux Inc.).
Each patient included was evaluated for the presence of any cutaneous manifestation. A detailed dermatological examination including mucosae, palms and soles was performed by a dermatologist from the author list (PDG, TH, HT). Each skin lesion was counted as a single episode. The dermatological examination was performed within 48 h after a positive blood culture. All included patients with skin lesions were subjected to clinical photography for medical files and gave oral consent. For analysis, we considered only the cutaneous manifestations, which were directly related to the bacteraemia. Hence, we excluded other prevalent dermatosis, such as eczema, vitiligo, carcinoma, psoriasis, etc.
Skin manifestations were classified into 4 different types, primary, secondary, by contiguity or undetermined, according to the likely origin of the bacteraemia. The classification was based on clinical findings and on chronological events. Hence, primary cutaneous manifestations were those corresponding to the starting point of the bloodstream infection and mainly comprised of skin cellulitis, lymphangitis, septic superficial thrombophlebitis, cutaneous abscess, and diabetic foot infections. Next, secondary cutaneous manifestations were those corresponding to secondary skin septic localization of the bacteraemia (such as septic emboli and erythematous nodules of the finger pad) and those corresponding to dermatological demonstration of septic shock (such as purpura fulminans, vascular purpura or livedo reticularis). Cutaneous manifestations by contiguity were defined as skin cellulitis associated with an underlying deep infection, such as arthritis, bursitis and visceral abscess. Finally, undetermined cutaneous manifestations were those for which the investigations failed to conclude on their characterization as primary or secondary manifestations.
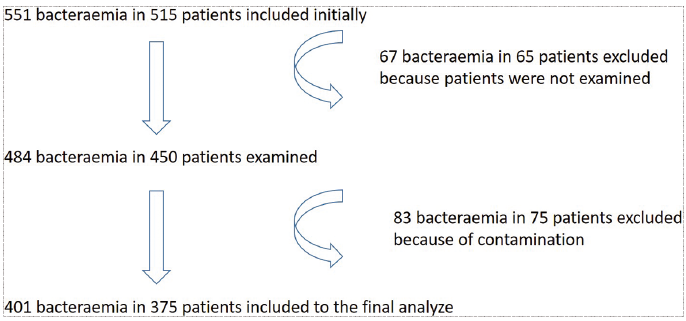
Over the year of study, 551 bacteraemias occurred in 515 patients. Due to contamination, 83 bacteraemias in 75 patients were excluded from the final analysis; 67 bacteraemias in 65 patients were also excluded because patients could not be examined (26 bacteraemias in patients who died and 41 bacteraemias in patients who were discharged from the hospital before the examination). Finally, 401 bacteraemias in 375 patients were included for the analysis: 209 males and 166 females (sex ratio = 1.26), mean ± standard deviation (SD) age 70 ± 19 years (Fig. 1); 406 infectious diagnoses were established (Table I). The most frequent diagnoses of the origin of the bacteraemia were urinary tract infections (n = 138, 34%), catheter infections (n = 100, 25%), infections of unknown origin (n = 50, 12%), angiocholitis (n = 17, 4%) and skin cellulitis (n = 9, 2%).
Fig. 1. Study flow chart. In our study a total of 551 bacteraemias in 515 patients were included. After exclusion of 83 bacteraemias in 75 patients due to contamination and 67 bacteraemias in 65 patients who could not be examined, 401 bacteraemias in 375 patients were selected for the final analysis.
Table I. Diagnosis associated with bacteraemia
From 401 bacteraemias in 375 patients, 431 bacteria were isolated (Table II), with 24 bacteraemias consisting of 2 different bacterial species and 3 consisting of 3. There were 220 (51%) Gram-negative bacilli (GNB), 201 (46.5%) Gram-positive cocci (GPC), 8 (2%) Gram-positive bacilli (GPB) and 2 (0.5%) Gram-negative cocci (GNC). There were 16 (4%) of anaerobes bacteria. The most frequently isolated bacteria were Escherichia coli (n = 137, 32%), S. aureus (n = 52, 12%), S. epidermidis (n = 41, 9.5%) and Enterococcus faecalis (n = 22, 5%).
Table II. Epidemiology of isolated bacteria
Thirty-nine cutaneous manifestations associated with bacteraemia in 34 patients corresponding to a prevalence of 9% were noted (Table III). Of these cases, there were 16 (41%) skin cellulitis, 5 (13%) lymphangitis, 5 (13%) septic superficial thrombophlebitis, 3 (8%) cutaneous abscess, 2 (5%) diabetic foot infections, 2 (5%) purpura fulminans, 2 (5%) vascular purpura, 1 (2.5%) septic emboli, 1 (2.5%) livedo reticularis, 1 (2.5%) acute paronychia and 1 (2.5) erythematous nodules of the finger pad. Two patients exhibited 2 different cutaneous manifestations: 1 presented with a Capnocytophaga canimorsus bacteraemia following a dog bite with cellulitis around the wound and purpura fulminans; the other presented with a Streptococcus milleri bacteraemia with cutaneous abscess and septic superficial thrombophlebitis. In addition, 1 patient with a Streptococcus pyogenes A bacteraemia exhibited 4 different cutaneous manifestations: septic emboli of the hands, erythematous nodules of the finger pad, cellulitis by contiguity with knee arthritis and elbow bursitis. All investigations failed to find the origin of this patient’s bacteraemia.
According to our classification, 27 (69%) primary cutaneous manifestations, 7 (18%) secondary ones, 4 (10%) cutaneous manifestation by contiguity and 1 undetermined cutaneous manifestation were noted. Descriptions of all the skin manifestations are shown in Table III.
Table III. Characteristics of cutaneous manifestations associated with bacteraemia
Thirty-five different types of bacteria were involved in these cutaneous manifestations (S. aureus and S. warnerii were isolated for 1 patient with a septic thrombophlebitis). There were 23 (65.5%) GPC, 10 (28.5%) GNB, 1 (3%) GNC and 1 (3%) GPB.
Of the bacteraemias due to GP bacteria (GPC and GPB), 12.9% were associated with cutaneous manifestations compared with 5.4% for GN bacteraemias (p < 0.001). More precisely, 12.9% of the bacteraemias due only to GPC, but 5.6% of the bacteraemias due to the other causes (GPB, GNB and GNC) were associated with cutaneous manifestations (p < 0.001).
In addition, among the primary cutaneous manifestations, 70.4% involved GP bacteria, whereas 29.6% involved GN bacteria.
Finally, of the secondary cutaneous manifestations, 57.1% involved GP bacteria, whereas 42.9% involved GN types.
Numerous dermatological manifestations have been reported in the literature associated with bacteraemias as isolated case reports, short series or specific pathologies. Indeed, a recent study showed that dermatological findings associated with infectious endocarditis included specific manifestations, such as necrotic lesions of the lower limb, purpura or splinter haemorrhages. However, bacteraemias include a wider spectrum of pathologies and, to our knowledge, the real prevalence and clinical spectrum of skin lesions in bacteraemic patients has not been evaluated. Our study reported a prevalence of 9%. We classified these cutaneous manifestations as primary (69%), secondary (18%), by contiguity (10%) and undetermined (3%) according to the starting point of the bloodstream infection. This classification was based on clinical findings, chronology of events and paraclinical results. As expected for primary cutaneous manifestations, the most reported types were skin cellulitis (41%), catheter infections causing primary cutaneous manifestations, such as lymphangitis (13%) and septic superficial thrombophlebitis (13%). Secondary cutaneous manifestations consisted of 2 cases of purpura fulminans (Capnocytophaga canimorsus, Neisseria meningitidis), 2 cases of vascular purpura in the context of infectious endocarditis and central catheter infection, one case of livedo associated with septic shock and one case of a patient presenting with septic emboli of the hands with erythaematous nodules of the finger pad. Moreover, we defined a third group of cutaneous manifestations by contiguity. This group included patients with primary underlying visceral or bone infections who later developed skin cellulitis.
Our microbiological and epidemiological findings pertaining to bacteraemias were similar to those reported in the literature, guaranteeing the reproducibility and the quality of our work. Indeed, as in previous studies, the most frequent diagnoses made were urinary infections (34%) and catheter infections (25%) (6). An origin of the bacteraemia was not found in 50 cases (12%), which is a rate similar to other studies (7). In terms of the microorganisms isolated, the most frequent were Escherichia coli (32%), S. aureus (n = 52, 12%), S. epidermidis (9.5%) and Enterococcus faecalis (5%), which was also comparable to the results of previous studies (6, 8, 9).
Furthermore, we reported certain correlations between skin manifestations and the bacteria involved. Hence, the most frequent bacteria implied in skin manifestations were GP types and, more precisely, GPC bacteria, such as S. aureus and Streptococci species. This was particularly true for primary cutaneous manifestations.
This study has several limitations. Not all of the patients with bacteraemias could be examined, and we had to exclude those who died or left the hospital before the dermatological examination. In addition, we could isolate only bacteria that are able to grow in standardized blood culture media. Indeed, some bacteria causing systemic infections, such as Rickettsia, Treponema, Borrelia, and Mycobacteria could not be taken into consideration due to the technical limitations of routine blood cultures. Moreover, H. cinaedi are detected from blood culture using an automatic blood culture system, such as the BACTEC or BacT/ALERT, but because H. cinaedi are slow-growing organisms, a relatively prolonged incubation time is generally required (4–10 days) (10).
Our study gives an overview of the rate of clinical skin manifestations associated with the usual cultivable bacteria isolated from bloodstream infections. Thus, a careful dermatological examination of septic patients may provide important information necessary to prescribe the most relevant probabilistic antibiotherapy.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize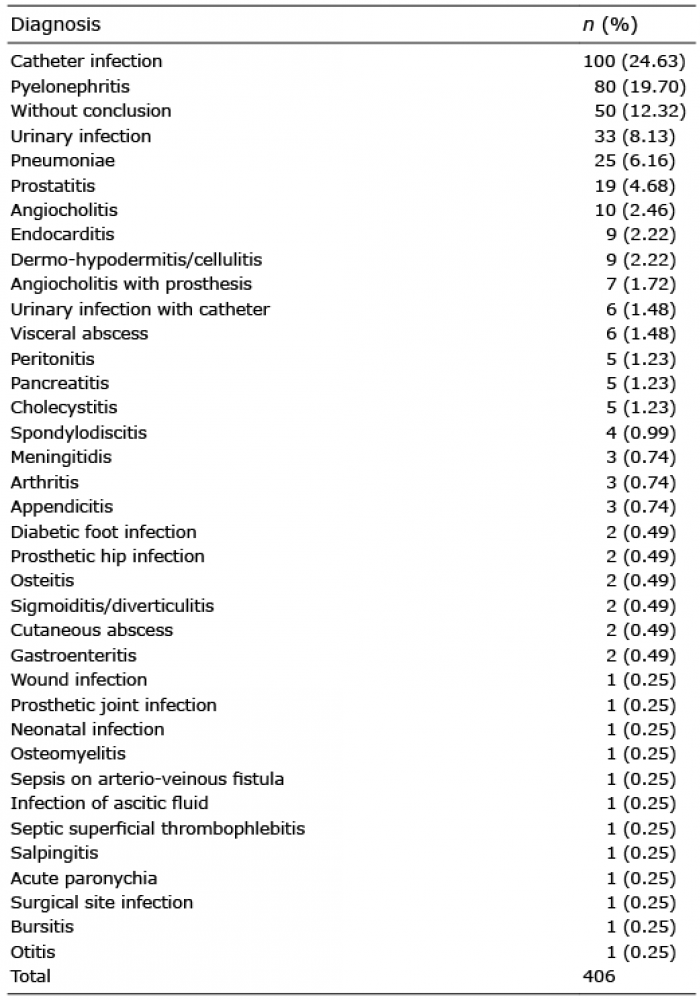 Click to show fullsize
Click to show fullsize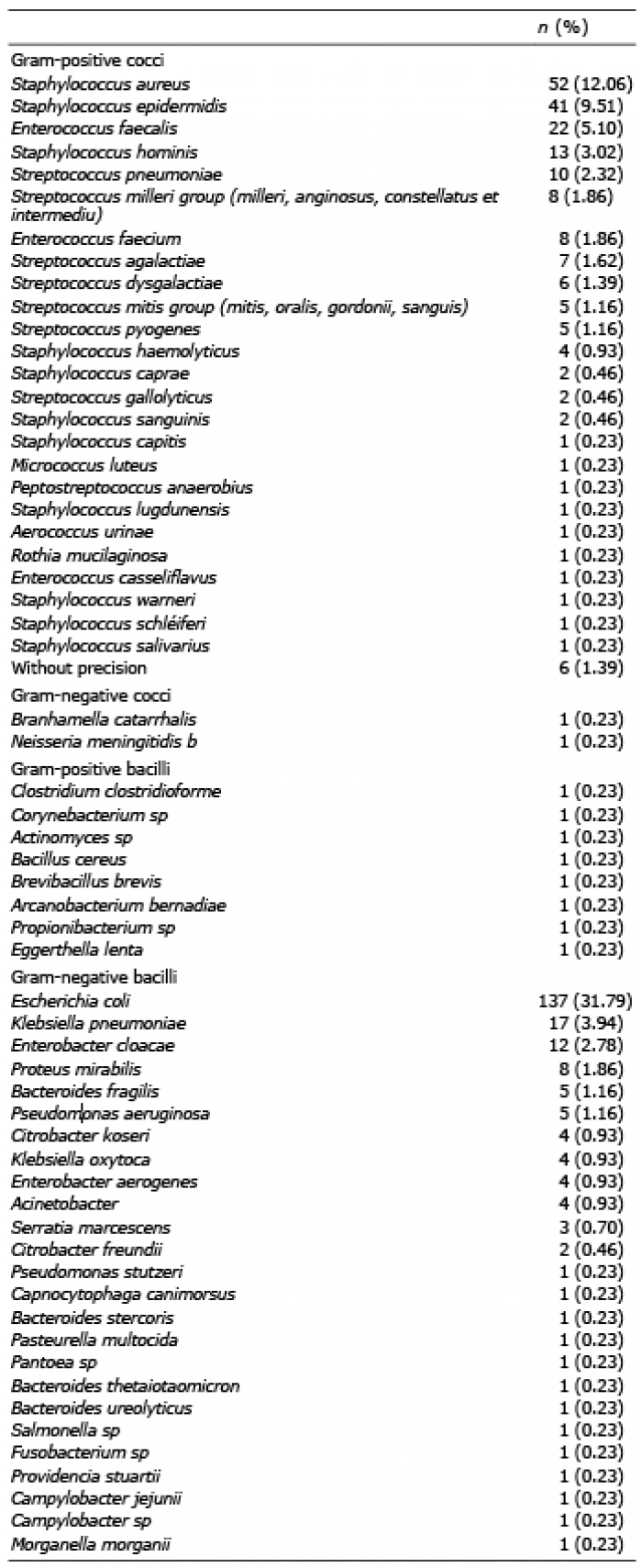 Click to show fullsize
Click to show fullsize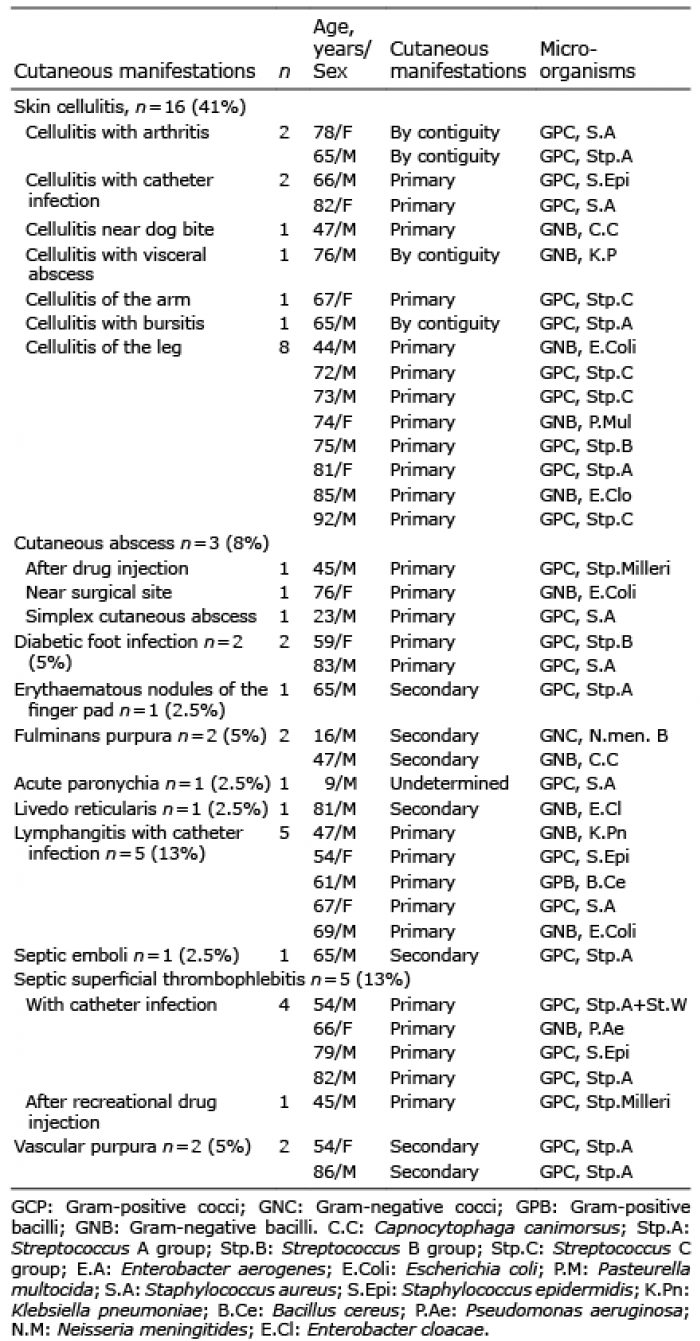 Click to show fullsize
Click to show fullsize