


1Department of Experimental and Clinical Medicine, Institute of Dermatology, University of Udine, Azienda Sanitaria Universitaria Integrata, Udine, Italy, and 2Dermatology Department and Skin Research Center, Saint Louis Hospital, Paris, France. E-mail: pinzca@gmail.com
Accepted Oct 16, 2018; Epub ahead of print Oct 17, 2018
Lichen planus pigmentosus (LPP) is a variant of lichen planus characterized by dark-brown macules usually distributed on sun-exposed areas or, rarely, on flexural folds. It is described more often in some ethnic groups from the Indian subcontinent, the Middle East, Far East, and Latin America, especially in people with darker phototypes (1). Blaschkolinear distribution of LPP, probably resulting from a genetic mosaicism, is rarely reported and called Blaschkolinear lichen planus pigmentosus (BLPP) (2). Skin chronic graft-versus-host disease (cGVHD) lesions after allogeneic hematopoietic stem cell transplantation (AHSCT) are characterized by a spectrum ranging from lichenoid to sclerodermoid manifestations (3).
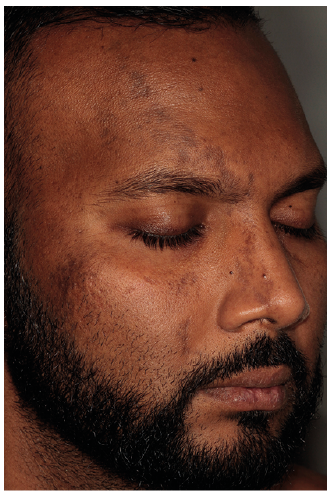
We report here a case of BLPP that occurred in a 34-year-old Mauritian man, who underwent an HLA-identical peripheral blood AHSCT for a stage IIA nodular-sclerosis classical Hodgkin lymphoma. Four months after AHSCT, the patient had cGVHD, namely a bronchiolitis obliterans, a diffuse interstitial pneumonia and a mouth/ocular sicca syndrome. Eight months later, a maculo-papular brownish linear eruption occurred following the Blaschko lines. These cutaneous lesions progressively involved the right leg, the right arm, and the right half-face (Fig. 1). Dermoscopic evaluation showed diffuse brown dots (peppering) over a brown background (Fig. 2), representing dermal pigmentary incontinence resulting from a lichenoid inflammation and dermal-epidermal interface damage (4). Histological analysis showed slight interface dermatitis with marked pigmentary incontinence (Fig. 3). On the basis of the clinical, dermoscopic, and histological presentation a diagnosis of extensive form of BLPP in the context of cGVHD was made. Four months of treatment with once-daily 0.05% betamethasone valerate cream on the body lesions and twice-daily 0.1% tacrolimus induced partial remission.
Fig. 1. Erythematous, maculo-papular brownish linear eruption following the Blaschko lines involving the right half-face. A written permission from the patient was given to publish this photo.
Fig. 2. Dermoscopic features of the lesion: diffuse brown dots (peppering) over a brown background.
Fig. 3. Histopathological features of the lesion (Hematoxylin Eosin Saffron, original magnification ×100). Basal layer vacuolization, pigmentary incontinence.
A case of a lichen striatus (LS) of the left arm as the only complication after AHSCT (for aplastic anaemia) has been reported previously (5), but to the best of our knowledge this is the first report of BLPP after AHSCT. Cases of LPP in the setting of cGVHD have been reported previously (6), but not with a distribution along the Blaschko lines. The aetiopathogenesis of BLPP is not completely understood, but is possible that interferon pathways could be involved (7). It has been postulated that cells of Blaschko lines, as part of skin mosaicism, become visible when stimulated by type 1 interferon (alpha and beta) chemokines (8). Upregulation of type 1 interferon-inducible genes has also been found in cGVHD monocytes (9).
In conclusion, BLPP should be considered in the wide spectrum of skin cGVHD symptoms. Physiopathological studies are warranted to understand the possible link between these 2 conditions.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize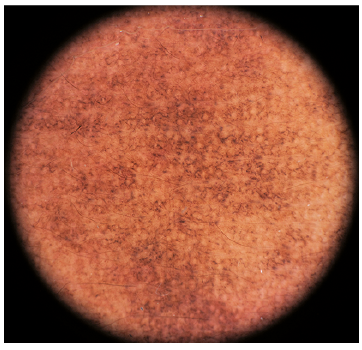 Click to show fullsize
Click to show fullsize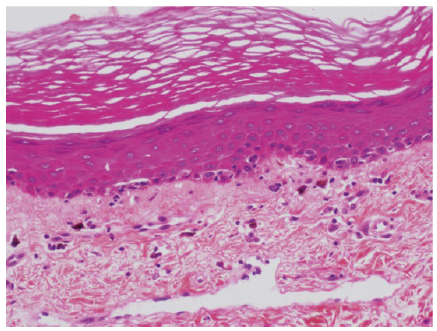 Click to show fullsize
Click to show fullsize