


1Pediatric Dermatology Unit – Department of Medicine DIMED, and 2Department of Statistics, University of Padova, Via Gallucci, 4, IT-35128 Padova, Italy. E-mail: anna.bellonifortina@gmail.com
Accepted Oct 16, 2018; Epub ahead of print Oct 17, 2018
Both adults and children with psoriasis are at risk for comorbidities, including obesity, hypertension, hyperlipidaemia, diabetes mellitus, metabolic syndrome, non-alcoholic fatty liver disease (1–12). Since obesity is a known risk factor for most of these comorbidities, it would be useful to determine whether psoriasis is an independent risk factor for some or all of them (6).
There is some evidence of psoriasis as an independent risk factor for comorbidities (1, 6), but most of the studies are retrospective or have limitations due to inter-institutional variations in data collecting methodologies, data interpretation, different populations studied or limited number of patients.
We performed a single-centre study screening for children with psoriasis who had high blood pressure, but without over-weight, obesity or central obesity, and age- and sex- matched controls.
Among children consecutively referred to the Pediatric Dermatology Unit, Padua University, Padua, Italy, 52 children with plaque-type psoriasis were identified, without over-weight, obesity or central obesity (between the ages of 4 and 16 years) and 52 age- and sex-matched children without psoriasis (control group), also without over-weight, obesity or central obesity.
The control group was recruited among children consecutively attending the Pediatric Dermatology Clinic for non-inflammatory diseases (i.e. warts, naevi, moles, etc.). Children with and without psoriasis were from the same geographical area, with similar demographic characteristics and, presumably, similar lifestyles. The following data were collected for each patient: physical examination, height, body weight, waist circumference, body mass index (BMI), waist-to-height ratio (WHtR), duration and severity of psoriasis, diastolic blood pressure (DBP), and systolic blood pressure (SBP).
Psoriasis severity was classified as mild or moderate-to-severe according to the Psoriasis Area Severity Index (PASI) and Body Surface Area (BSA). When PASI was ≥ 10 or/and BSA was >10 psoriasis was designated as moderate-to-severe (4). Duration of disease was calculated in months, considering the onset of initial clinical symptoms of psoriasis. None of the children was using or had used systemic medications that could increase blood pressure (e.g. corticosteroids, cyclosporine, etc.).
BMI allowed us to classify children as normal-weight, overweight, or obese according to the BMI cut-offs of the 2012 International Obesity Task Force (13). Waist circumference (WC) was measured twice, midway between the lowest border of the rib cage and the upper border of the iliac crest, at the end of normal expiration, using inextensible anthropometric tape with the patients standing erect and relaxed with their arms at their sides and feet positioned close together. The mean values were considered for analysis (4). Evaluation of central obesity was performed using WHtR, calculated as WC divided by height. Patients with a WHtR ≥ 0.5 were classified as having central obesity (4).
Exclusion criteria for patients in both groups were: children with overweight, obesity, or central obesity (WHtR ≥ 0.5), other inflammatory or autoimmune diseases and smoking habit.
The measurement of diastolic and systolic blood pressure (BP) was performed using an aneroid sphygmomanometer with an appropriate sized cuff for each patient. BP was measured in the right arm by using standard measurement practices. The conditions of blood pressure measurements were similar between groups of children. When the initial BP was elevated (≥ 95th percentile), 2 additional measurements were performed at the same visit. Mean values were considered for analysis. BP values were categorized as normal BP (> 50 and ≤ 90th sex, age and height specific percentile), elevated BP (> 90th sex, age and height specific percentile), stage 1 hypertension (stage 1 HTN) (≥ 95th sex, age and height specific percentile), stage 2 hypertension (stage 2 HTN) (≥ 95th sex, age and height specific percentile +12 mmHg) (14).
Demographic and clinical data were summarized using percentages and means and standard deviations. Differences in quantitative variables between subjects groups were assessed with Student’s t-test or Mann–Whitney test, according to the Shapiro-Wilk test of normality. For categorical data the association between variables was assessed with the odds ratio and tested using the Fisher’s
exact test. A logistic regression model was used to determine which covariates were associated with psoriasis and control groups. A receiver operating characteristic (ROC) curve analysis was performed to assess the discrimination ability of the logistic regression. Analysis of covariance (ANCOVA) regression models were used to study how the dependent variables weight, BMI, WHtR, systolic blood pressure and diastolic blood pressure depend on both age and psoriasis and control group.
Statistical significance was set at p < 0.05. Data were analysed using the statistical software R.
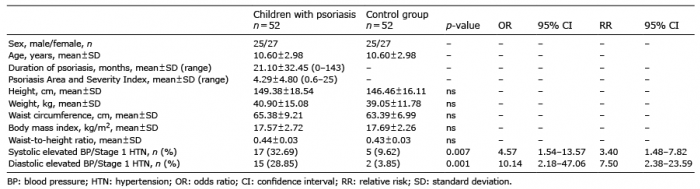
Mean age of the children was 10.60 ± 2.98 years and 27 (51.92%) were girls. Mean systolic blood pressure was 112.27 ± 9.84 mmHg in children with psoriasis and 106.17 ± 9.72 mmHg in controls. Mean value of diastolic blood pressure was 71.01 ± 6.20 mmHg in children with psoriasis and 65.48 ± 6.94 mmHg in controls (Table I).
Among psoriatic children, 28 (53.85%) had normal blood pressure and 24 (46.15%) had systolic or diastolic elevated blood pressure/stage 1 HTN; 8 (15.38%) of these, had both systolic elevated BP/stage 1 HTN and diastolic elevated BP/stage 1 HTN. Among controls, 46 (88.46%) had normal blood pressure and 6 (11.54%) had systolic or diastolic elevated BP/stage 1 HTN; 1 (1.92%) of these had both systolic elevated BP/stage 1 HTN and diastolic elevated BP/stage 1 HTN.
Children with psoriasis, compared with children with-out, had a statistically significant higher prevalence of systolic elevated BP/stage 1 HTN (OR 4.57; p = 0.007) and diastolic elevated BP/stage 1 HTN (OR 10.14; p = 0.001) (Table I).
Table I. Demographic, clinical features and percentage of hypertension in normal-weight children with psoriasis compared with normal-weight children without psoriasis
Among children with psoriasis, no statistically significant difference as regards BMI, WHtR, PASI and duration of psoriasis was found between children with high blood pressure and children with normal blood pressure.
ANCOVA regression models showed that systolic elevated BP and diastolic stage 1 HTN were independently associated with psoriasis in children compared with control group (OR 12.7, p = 0.02; OR 17.3, p = 0.01) (Fig. 1).
Fig. 1. (A) Systolic blood pressure values (mmHg), (B) diastolic blood pressure values (mmHg). (a) Children with psoriasis, (b) control group.
Our study investigating blood pressure in normal-weight children with psoriasis shows an association between psoriasis and high blood pressure independently of over-weight status. Similar results, suggesting psoriasis as an independent risk factor for the development of high blood pressure, have been reported recently from a study investigating a large retrospective database of children with psoriasis (6). Such findings suggest the need to assess comorbidities in all children with psoriasis (i.e. also in children without overweight or obesity). Possible limitations of our study are the relatively small numbers of patients and the lack of multiple blood pressure readings at separate visits.
This work was supported in part by the University of Padova under project CAEPAE.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize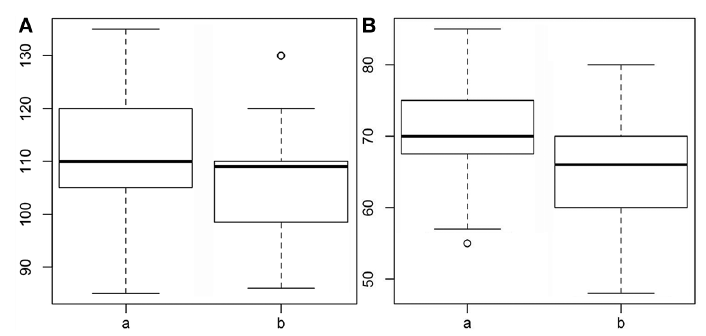 Click to show fullsize
Click to show fullsize