


1Department of Dermatology, Severance Hospital, Cutaneous Biology Research Institute, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 03722, and 2Institute of Health Services Research, Department of Preventive Medicine, Graduate School of Public Health, Yonsei University, Seoul, Korea. E-mail: oddung93@yuhs.ac
#These authors contributed equally to this study.
Accepted Nov 1, 2018; Epub ahead of print Nov 5, 2018
Alopecia areata (AA) is a non-scarring alopecia resulting from an immune response against hair follicles. It occurs equally in both sexes and can affect every age group. AA is a chronic disease that can negatively affect a patient’s mental health due to its relapsing nature and effect on appearance. Previous cross-sectional, case-control studies have demonstrated a relationship between AA and psychological stress (1–5). Among multiple therapeutic approaches, intralesional injection (ILI) of corticosteroids is most widely used for treating alopecic patches of AA, but this invasive procedure usually reflects disease severity and chronicity and is accompanied by painful discomfort.
There is currently a lack of evidence from a large-scale population-based cohort study to directly examine the presence of psychological stress in patients with AA according to the invasive therapeutic modalities used. In this study, psychiatric appointments and the burden of AA were analysed in patients with AA using Korea National Health Insurance Cohort Data (NHICD) from 2002 to 2013. In addition, the study evaluated the association between psychiatric appointments and other factors, such as type of AA and treatment modalities.
From a cohort of subjects younger than 20 years, participants who had been newly diagnosed with AA during the study period were included as the AA group, and those who had never been diagnosed with AA during the same period were included as the control group. Since the study aimed to explore only those patients with new onset of AA, subjects with a history of AA and psychiatric appointments were excluded. The adjusted hazard ratios (HR) and 95% confidence intervals (95% CI) for visits to a psychiatrist were estimated by applying a Cox proportional-hazard regression (see Appendix S1 for details).
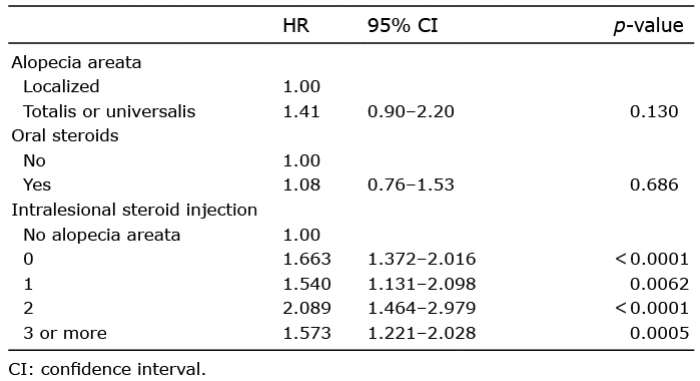
This study included 370,019 subjects, including 4,707 patients with AA (1.3%) and 23,943 patients who had visited the psychiatric clinic at least once during the follow-up period (Table SI). The ratio of patients visiting a psychiatric clinic was approximately 1.6 times higher in patients with AA than in the non-AA group. Patients with AA had higher rate of psychiatric visits compared with controls (2,862.5 vs. 853.7 cases/100,000 person-years). The demographic findings of enrolled participants were investigated based on psychiatric visits (Table SII). The multivariate analyses of all patients were analysed with basic demographic data, including age, sex, income, type of disease and treatment modality. The tendency for visits to psychiatrists was significantly higher in patients with AA compared with the control group (HR 1.64, 95% CI 1.45–1.86) (Table SIII). Moreover, compared with non-AA controls, the adjusted HRs for psychiatric visits were significantly increased according to the number of ILI treatments (Table I, ILI=1 vs. ILI=2 vs. ILI≥3; HR 1.54, 95% CI 1.09–2.03 vs. HR=2.09, 95% CI 1.31–2.02 vs. HR 1.57, 95% CI 1.22–2.03, respectively). Patients with alopecia totalis or universalis showed an increased adjusted HR for psychiatric clinic visits compared with patients with localized AA; however, this was not statistically significant (HR 1.41, 95% CI 0.90–2.20). The psychiatric visit risk for patients who used oral steroids did not differ from that of control groups (HR 1.08, 95% CI 0.76–1.53).
Table I. Adjusted hazard ratios (HR) for outpatient visits to psychiatrists by type of disease and treatment modality
Hair is an important part of our appearance, and hair loss can drastically affect self-esteem and social relationships. A positive correlation between AA and psychiatric appointments has been confirmed through Minnesota Multiphasic Personality Inventory, surveys and questionnaires (6–8). However, most of these studies were case series with a small sample size. To the best of our knowledge, this study was the first longitudinal cohort study, using a large sample size examining the relationship between AA and psychiatric appointments. Our study showed that patients with AA had significantly higher risk for visits to psychiatric clinics compared with the control group, and even higher hazards for visits to psychiatric clinics were observed as the number of ILI increased. The selection of ILI as a treatment option for AA and the frequencies of ILI could reflect the disease severity of AA because the use of topical steroid alone or observational follow-up is more common in mild cases of AA. On the other hand, there could be some personality or psychopathological factors that influence patients’ decisions to accept doctors’ proposal to undergo invasive and potentially painful ILI procedure in AA. Thus, a medical history of ILI might be a “red flag” for risk of mental health problems in patients with AA. However, it is possible that pain during ILI might exacerbate psychological stress in patients with AA, considering that mental health appointments in patients with AA increased with increased number of ILI. However, further research is needed into the relationship between psychological stress and the response and pain to therapy.
The present study has several limitations. Firstly, psychiatric appointments do not strictly imply that the cause of psychological stress is AA. Secondly, initial cohort population only included subjects younger than 20 years, because we wanted to check the psychological stress due to AA at ages when social stress is relatively lacking, which may have led to age selection bias. Nevertheless, these data might represent the status of psychological stress among adolescent patients with AA and further study is needed to directly compare psychological stress between adolescent and adult patients with AA.
In conclusion, this study suggests that AA is closely associated with psychological stress and ILI, a treatment option for AA can be associated with increase in psychological stress because ILI can mirror the disease severity of AA and may result in psychological stress caused by painful procedures. Therefore, dermatologists should pay close attention to psychological stress in patients with AA who receive multiple ILI treatments and consider them for early referral to psychiatrists.
IRB approval status: reviewed and approved by the Graduate School of Public Health at Yonsei University (IRB approval number: 2-1040939-AB-N-01-2014-239).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize