


1Department of Dermatology, Xiangya Hospital, 2Hunan Engineering Research Center of Skin Health and Disease, 3Hunan Key Laboratory of Skin Cancer and Psoriasis, and 4Department of Social Medicine and Health Management, Xiangya School of Public Health, Central South University, Changsha, China
The association of atopic dermatitis and chronic spontaneous urticaria with socioeconomic status has been little studied. The aim of this study was to investigate the prevalence of skin diseases and their association with socioeconomic status in adolescents in China. A cross-sectional study was conducted at Central South University, Changsha, China. All newly enrolled students underwent dermatological examination and completed a survey. Socioeconomic status was measured in terms of parental education level and income. Two-level logistic regression models were used. A total of 8,226 students consented to participate. On dermatological examination, moderate to severe acne (10.2%) had the highest prevalence, followed by chronic spontaneous urticaria (2.7%), atopic dermatitis (2.5%), and tinea (1.7%). Socioeconomic status was positively associated with the prevalence of chronic spontaneous urticaria (ptrend = 0.001) and atopic dermatitis (ptrend = 0.0094). Tinea was inversely associated with socioeconomic status (ptrend = 0.025). Higher parental socioeconomic status was associated with higher risk of atopic dermatitis and chronic spontaneous urticaria, but lower risk of tinea.
Key words: socioeconomic status; atopic dermatitis; chronic spontaneous urticaria; adolescent.
Accepted Dec 6, 2018; E-published Dec 6, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Xiang Chen and Minxue Shen, Department of Dermatology, Xiangya Hospital, Central South University, 87 Xiangya Road, Changsha, Hunan, China 410008. E-mail: chenxiangck@126.com, shenmx1988@csu.edu.cn
This is the first population-based epidemiological survey in Chinese adolescents regarding the prevalence of skin diseases. Health disparities exist in chronic spontaneous urticaria, atopic dermatitis, and tinea across adolescents’ parental socioeconomic status. A deeper understanding of the complex socioeconomic risk factors and mediators for skin diseases, especially allergic skin diseases, is needed.
Skin diseases with atopic or allergic backgrounds, such as atopic dermatitis (AD), allergic contact dermatitis (ACD), and urticaria, have been an increasing focus of attention in recent years (1, 2). AD, a common chronic inflammatory skin disorder affecting one-fifth of the population in developed countries (3), is generally considered as an atopic disease, together with allergic rhinitis and asthma (4). Chronic spontaneous urticaria (CSU), manifesting as recurrent itchy wheals and/or angioedema for more than 6 weeks, affects 0.5–1% of the general population (5), and 0.1–0.3% of children (6). Although their aetiologies are complicated and manifestations varied, AD and CSU, share many similar risk factors related to their increasing prevalence (2). Previously, epidemics of atopic diseases and skin allergies have been recognized more widely in western, developed, countries, compared with less-developed regions of East Asia, Europe and Africa (7–9). How-ever, this global difference in prevalence has reduced, and public health concern is increasing in developing countries. Accumulated evidence has shown that these changing epidemics are associated with altered societal, economic and environmental determinants, in addition to genetic-susceptibility aetiology (10, 11).
Socioeconomic status (SES), an important indicator of socioeconomic determinants, in studying health disparities across different populations, is often measured according to income, education level and occupation at the individual level, and is determined by diverse economic contexts at the population level (12). A systematic review has reported wide variations in associations of SES with allergic rhinitis and asthma (13); however, the association of skin allergy, especially AD, with SES was consistent (4, 14). Globally, the prevalence of AD and CSU in developed countries is higher than in developing countries in general (1). Furthermore, it has been reported that urban citizens with higher SES are more likely to experience allergies than those in deprived areas (14, 15). China, which has a typical transitional economy, has been undergoing rapid economic development, immense urbanization, and frequent socioeconomic mobility since the 1980s, which exert unmeasurable diverse influence on all sorts of disease epidemics. The prevalence of AD has been reported to have increased from 3.1% in 2002 to 12.9% in 2014 among selected children in China (16, 17). For CSU and ACD, population-based epidemiological data is lacking. In short, the prevalence of these conditions in China is unclear, and the impact of socioeconomic determinants has not yet been addressed.
The aim of this study was therefore to investigate the prevalence of primary skin diseases, especially atopic skin diseases and CSU, and to examine their association with indicators of socioeconomic disparities, including SES and ethnicity, through a cross-sectional survey of newly-enrolled college students.
This cross-sectional study hypothesized that health disparities exist across skin diseases. Central South University, Changsha, China, with geographically dispersed enrollment policy, was chosen as the sampling unit. All newly enrolled students who consented to participate underwent a health examination and online questionnaire survey in September 2017.
A web-based questionnaire survey was conducted on a single day, organized by the department of student affairs of the university. The first-year student participants completed the questionnaire in separate computer rooms where privacy was guaranteed. During the survey, 3 investigators were assigned to each room to provide technical support. The questionnaire comprised 84 questions, including demographic information (ethnicity, original regions, parental highest educational level, household annual income (in yuan), number of household members that live together for more than 6 months per year); disease history (cardiovascular/metabolic diseases, autoimmune diseases, infectious diseases, mental disorders, etc.); history of allergy (food, drug, chemicals); cigarette smoking (quantity, frequency, years of smoking, passive smoking), etc.
Socioeconomic determinants were measured mainly by SES and ethnicity. Since all of the participants were newly enrolled college students, parental SES was used to represent the socioeconomic strata of their original families. Parental SES was measured primarily by per-capita annual income and highest parental educational level. Per-capita income was calculated as annual household income divided by the number of household members who lived together for more than 6 months per year, and was then divided into province-level quintiles. The highest parental educational level was categorized into primary school and below, middle-school, high-school, college and above.
In addition to the individual level measure of SES, per-capita gross domestic product (GDP) of China’s provinces, municipalities, and special administrative regions in 2016, obtained from the official site of the National Bureau of Statistics, was used as the secondary indicator of SES.
Diagnosis of skin diseases and enquiry about disease history were performed by certificated dermatologists with wide clinical experience, during the dermatological examination. Clinical manifestation, disease history, and family history of participants were queried, and physical examinations were conducted to diagnose any skin diseases. For recurrent skin diseases, only those with current symptoms and lesions were diagnosed as cases of point prevalence. Height and weight were measured using standardized methods and body mass index was calculated.
Continuous data were presented as means±standard deviations, and between-group difference was tested using analysis of variance. Categorical data were presented as number (%), and between-group difference was tested using χ2 test. Cochran-Mantel-Haenszel χ2 test was used to test the linear trend of skin disease prevalence across SES (diseases with less than 100 cases were not tested because of to the limited power of test). Two-level logistic regression model (individual as level 1 and province as level 2) was used to estimate the fixed effect of SES on prevalence of skin diseases, adjusting for level-1 confounders (age, sex, ethnicity, parental highest educational level, cigarette smoke exposure, pet ownership, history of food allergy, history of drug allergy) and level-2 confounder (provincial per-capita GDP). The effect size of SES was presented as odds ratio (OR) and 95% confidence interval (95% CI). The lowest SES group served as the referent group in all models. The intra-cluster correlation coefficient (ICC) was calculated as τp/(τp+3.29), where τp is level-2 covariance and the constant 3.29 is level-1 error variance. Sensitivity analysis was performed by excluding students from Hunan province (because the university is located in Hunan province and students from this area accounted for 17.3% of the sample). p < 0.05 was considered statistically significant for all tests. Statistical analysis was performed in SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
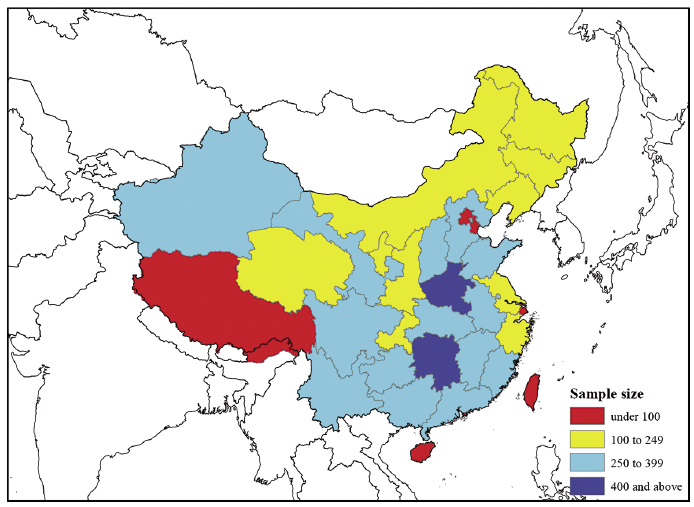
A total of 8,226 students who consented to participate underwent the health examination and completed the questionnaire; and 237/8,463 (2.8%) refused to participate. The geographical distribution of the students’ origin is shown in Fig. 1. The sex-specific number of cases and point prevalence of skin diseases are shown in Table I. The conditions with highest prevalence were: moderate to severe acne (10.2%), followed by CSU (2.7%), AD (1.7%), tinea (1.7%), and inducible urticaria (1.5%).
Fig. 1. Geographical distribution of students’ origin.
Table I. Unadjusted prevalence of skin diseases in the participants
The demographic characteristics of the students are shown in Table II. The distribution of SES was consistent with the rank of provinces by GDP per capita (Spearman correlation r = 0.24, p < 0.001). Han ethnicity was associated with higher SES. Students who chose to major in engineering had relatively lower SES compared with students in other disciplines. Body mass index (BMI) was positively associated with SES.
Table II. Characteristics of participants across per-capita annual income quintiles
The association of SES with skin diseases (with at least 100 cases observed) was tested. As shown in Table III, students with higher family per-capita income had increased prevalence of CSU (ptrend < 0.001) and AD (ptrend = 0.009), yet decreased prevalence of tinea (ptrend = 0.025). By contrast, income was not significantly associated with the prevalence of moderate to severe acne, or inducible urticaria (ptrend > 0.05).
Table III. Association of family per-capita income with the point prevalence of common skin diseases
The associations of SES with skin diseases were further investigated using 2-level logistic regression models. As shown in Fig. 2, crude and adjusted models demonstrate consistent results. The prevalence of CSU was positively associated with SES in a clear dose-response manner (adjusted OR increased from 1.11 to 2.00, compared with the lowest SES group). AD was similar to CSU, with adjusted OR increased from 1.01 to 1.69, although the association was marginally significant (p = 0.066). Tinea was inversely associated with SES in spite of some variations (adjusted OR decreased from 0.75 to 0.43). Ethnicity, highest parental educational level, and per-capita GDP were not significantly associated with the point prevalence of CSU, AD, and tinea in the adjusted models (data not shown).
In addition to the key findings, self-reported allergies to drugs and food were also identified as risk factors for CSU and AD. Sensitivity analysis, by excluding students from Hunan province, showed consistent results (data not shown).
Fig. 2. Fixed effect of socioeconomic status on the prevalence of skin diseases. The effect size was presented as odds ratios (OR) and 95% confidence intervals (CI), estimated by 2-level logistic regression models. Blue and green dots signify crude and adjusted estimates, respectively. Adjustment included level-1 confounders (age, sex, ethnicity, parental highest educational level, cigarette smoke exposure, pet ownership, history of food allergy, history of drug allergy) and level-2 confounder (provincial per-capita gross domestic product (GDP)). The lowest socioeconomic status quintile served as the referent group.
To our knowledge, this study is the first to report the prevalence of skin diseases among young people in China, and the first to link common skin diseases, especially atopic conditions and urticaria (all varieties), with socioeconomic determinants in China.
The study found that the mean point prevalence of CSU among Chinese adolescents with mean age of 18 is 2.7%, which is higher than in most of the world (5, 6, 15). We observed a female predilection in CSU, which is consistent with the findings from Zhong’s hospital-based study of CSU in China (18). The point prevalence of AD in our study is 2.5%, which is lower than the 12.9% reported for urban children in China (17). There are several possible reasons for this: first, we only diagnosed current patients and reported point prevalence by physical examination; secondly, our study researched the population aged approximately 18 years, in contrast to the previous study, which included children up to 7 years of age. Thirdly, our sample had more dispersed geographical distribution and SES, compared with previous urban-based research (18).
The current study proposed a significant positive relationship between SES and the point prevalence of CSU and AD in a dose-response manner; in contrast, tinea showed an inverse association with SES. There were only a few published data regarding the association between atopic skin diseases, skin allergies, and SES, which failed to draw a consistent conclusion (14, 15, 19, 20). Apart from SES, atopic skin diseases have also been reported to be associated with a variety of other social determinants, which may be parallel or downstream factors in SES, such as air pollution, social mobility, and urbanization, and changes in dietary habit (21, 22). In addition, SES could affect certain susceptible factors of allergic diseases, such as birth overweight, childhood obesity, maternal smoking, and caesarean section (21–23). All of these socioeconomic, cultural and environmental factors interweave to co-influence epidemics of allergic diseases. In China in particular, increasingly diverse SES, as well as accelerated urbanization, increased environmental pollution, and high caesarean section rate, constructs an intricate picture of the social determinants of allergic diseases. Several epidemiology studies have attempted to detect the population-level risk factors for asthma and allergic rhinitis in China (24–26), yet no study of skin allergies for this purpose has been studied previously. Hence, population-level concerns in China of skin allergies, such as AD and CSU, deserve higher priority. Dermatologists will continue to track possible mediators of SES of skin allergies in future cohort and clinical research.
This study has some limitations. First, there was a selection bias in representing adolescents in China. Participants were limited to homogeneous adolescents aged approximately 18 years with a similar educational background. Nonetheless, our sampling population came from diverse geographical and socioeconomic backgrounds prior to their enrollment. The per-capita household income is similar to that reported in the China Statistical Yearbook 2017 (27). This specific group was examined, and the results warrant extension of the research to other age groups. Secondly, the study did not take asthma and allergic rhinitis into consideration due to the limited feasibility of diagnosing allergic rhinitis and asthma during the field survey.
The study also has some strengths: it was the first population-based dermato-epidemiological study among Chinese adolescents; secondly, it is the first population-based study proposed to correlate socioeconomic determinants with skin diseases in China, and is a good initial reference regarding socioeconomic disparities in atopic diseases and skin diseases. Thirdly, the current study reinforces the known evidence that socioeconomic determinants diversely affect allergic diseases across different cultural and economic contexts. Finally, the study included a relatively large number of participants, and the participation rate was extremely high owing to the administrative intervention.
This study reported a higher point prevalence of CSU among the Chinese adolescent population than has been reported worldwide; hence the challenge ahead should not be underestimated. It was found that health disparities exist in CSU, AD, and tinea across adolescents’ parental SES, indicating an urgent need for a deeper understanding of the complex socioeconomic risk factors involved in atopic skin diseases and skin allergies. Therefore, clinical dermatologists, allergists, researchers, and patients should view atopic diseases from a broader perspective, and allergy prevention and control should be advocated at the macro level.
The authors would thank the following dermatologists who participated in the field survey (in alphabetical order of family name): Lei Cai, Duling Cao, Qin Cao, Chao Chen, Menglin Chen, Jia Guo, Yeye Guo, Rui Hu, Xing Hu, Kai Huang, Xinwei Kuang, Li Lei, Keke Li, Wenyuan Li, Yayun Li, Dihui Liu, Nian Liu, Panoan Liu, Runqiu Liu, Manyun Mao, Qunshi Qin, Lirong Tan, Ling Tang, Ni Tang, Tianhao Wu, Yun Xie, Siyu Yan, Lin Ye, Yi Yu, Hu Yuan, Rui Zhai, Zhibao Zhang, Yaqian Zhao, and Youyou Zhou. The investigators are from the Department of Dermatology, Xiangya Hospital, Central South University.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki. All procedures involving patients were approved by the institutional research ethics boards of Xiangya Hospital, Central South University (Changsha, China). Electronic informed consent was obtained from all students prior to the investigation.
This work was supported by the Ministry of Science and Technology of the People’s Republic of China (2015FY111100, 2016YFC0900802), and the Department of Science and Technology of Hunan Province (2018SK2086).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize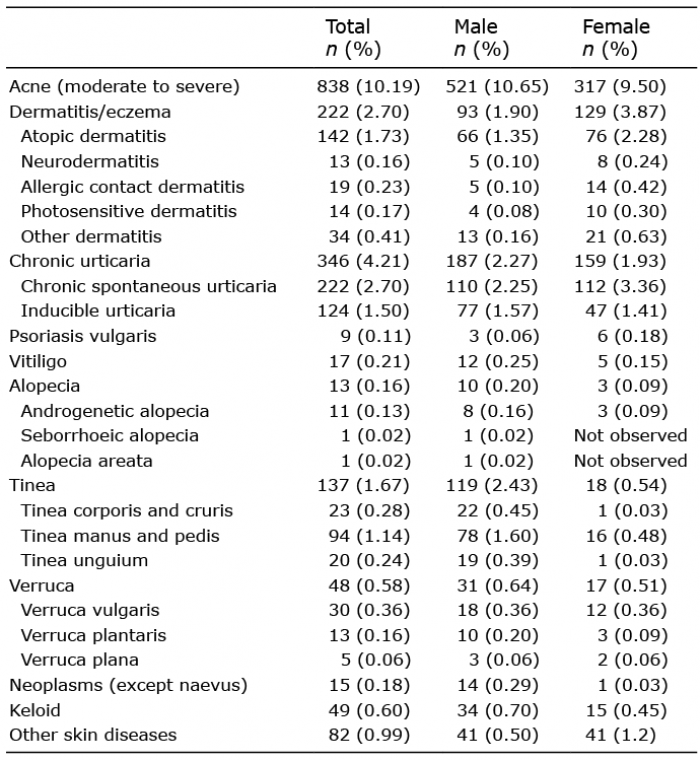 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize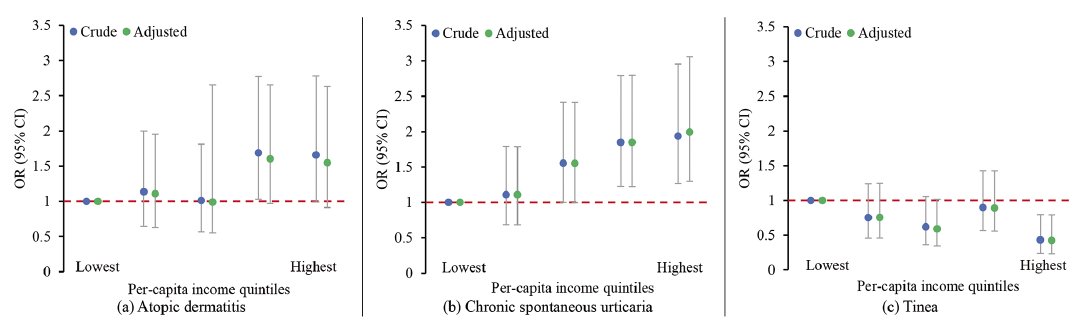 Click to show fullsize
Click to show fullsize