


1Department of Dermatology, University of Colorado Denver School of Medicine, 1665 Aurora Court, Denver CO 80045, 2Department of General Surgery and 4Department of Dermatology, University of Illinois, Chicago, Chicago, IL, and 3Department of Pathology, Presence Saint Joseph Hospital, Chicago, IL, USA. E-mail: agflorek@gmail.com
Accepted Dec 6, 2018; E-published Dec 6, 2018
Massive localized lymphedema (MLL) is an emerging complication of the obesity epidemic and a challenging clinical entity mimicking liposarcoma. It presents as an ill-defined mass of the proximal medial extremities in morbidly obese adults (1). MLL is caused by the compression of regional lymphatic vessels by massive adipose tissue (1–3). Although benign, the diagnosis can be challenging since atypical lipomatous tumors and liposarcomas present in the same manner (2, 3). Furthermore, MLL can transform to an angiosarcoma, in a phenomenon known as Stewart-Treves syndrome (2, 3). This case highlights the need for clinical vigilance for dermatologists to recognize this entity morphologically and to institute appropriate investigation and management.
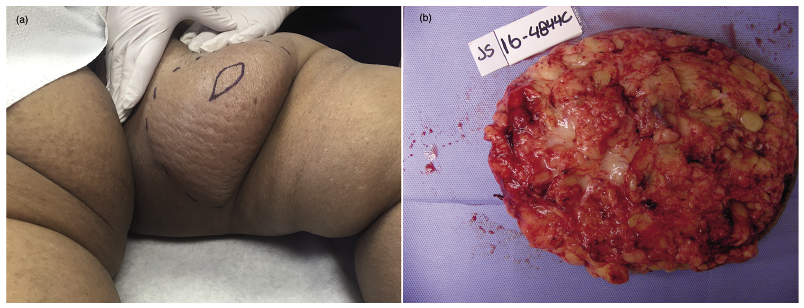
A 52-year-old morbidly obese woman (weight 145.9 kg, body mass index 53.4 kg/m2) with no significant medical or surgical history, presented with a one-year duration of a gradually enlarging, asymptomatic swelling of the left upper inner thigh. Physical exam revealed an ill-defined, skin-colored, firm mass with a woody induration, peau d’orange appearance, and non-pitting edema (Fig. 1a).
Fig. 1. a) Ill-defined, non–tender, skin-colored, pendulous mass on the left upper inner thigh with thick, firm, woody induration, peau d’orange appearance, and non-pitting edema. b) The patient underwent wide excision of the tumor (21.8 × 14.9 × 4.6 cm; 83.1 g) with clear margins confirmed on histopathology with identical findings to original incisional biopsy.
An incisional biopsy revealed a markedly edematous dermis with increased ectatic lymphatic channels, spindle-shaped cells, floret-like multinucleated cells, and atypical stromal spindle cells (Fig. 2a). The spindle-shaped cells and floret-like multinucleated cells were positive for CD34 (Fig. 2b) and negative for CD31 and smooth muscle actin. These findings were most consistent with massive localized lymphedema (MLL).
The patient underwent wide excision of the tumor (21.8 × 14.9 × 4.6 cm; 831.1 g) with clear margins confirmed on histopathology (Fig. 1b). Over the next 12 months, patient was monitored closely and showed no recurrence of the tumor.
Fig. 2. a) Markedly edematous dermis with increased ectatic lymphatic channels. There were increased spindle-shaped cells and floret-like multinucleated cells, as well as atypical stromal spindle cells (hematoxylin and eosin, × 400). b) The spindle-shaped cells and floret-like multinucleated cells were positive for CD34 stain (CD34 stain, magnification × 400).
Massive localized lymphedema is a rare entity that presents with long-standing, painless, slow-growing, ill-defined soft tissue mass in middle age morbidly obese adults (2, 3). This condition is more frequently found in women and has a predilection for the inner thigh (2, 3).
MLL may resemble a liposarcoma both clinically as well as histologically. Although MLL is a non-neoplastic lesion, its rapid growth, hypercellularity, cytologic atypia and mitotic activity make it prone to be misdiagnosed as a sarcoma. Histological diagnosis of MLL remains challenging for pathologists. Bogusz et al. (4) have summarized morphologic features which distinguish MLL from atypical lipomatous tumor (ALT)/well differentiated liposarcoma (WDL) (Table I). Grossly, these lesions are large with thickened, indurated overlying skin and peau d’orange appearance. The dermis and the subcutaneous tissue are fibrotic, and the septa in the subcutaneous fat are thickened and filled with edema fluid, fibroblasts, and collagen, thus diminishing the relative volume of the fat cells. These thickened septa mimic the fibrous bands in a liposarcoma. The overlying epidermis is acanthotic and hyperkeratotic, while the dermis is fibrotic and contains dilated lymphatic channels. What distinguishes MLL from a liposarcoma is the absence of lipoblasts and neoplastic cells with severe nuclear atypia. Additionally, another distinguishing marker is the presence of MDM2 gene amplification in ALT/WDL, compared to its absence in MLL (5). Lastly, the overall architecture of the subcutaneous fat is relatively preserved in MLL compared to liposarcoma.
Table I. Histological features distinguishing massive localized lymphedema (MLL) and atypical lipomatous tumor (ATL)/well-differentiated liposarcoma (WDL)
The preferred mode of treatment is surgical excision, in order to restore mobility, prevent recurrent infections, and confirm the diagnosis (2, 3). In minority of cases, the lesions may be managed conservatively with weight loss, physical therapy, compression, drainage, and skin hygiene. Without weight loss, due to the continued compression of the lymphatics, recurrence rates after excision have been reported to be as high as 50% (1).
The distinct clinical presentation and its characteristic histologic findings should alert dermatologists to the possibility of MLL versus its malignant mimickers. For these reasons, it is imperative for dermatologists to be able to recognize and treat the early signs of MLL.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize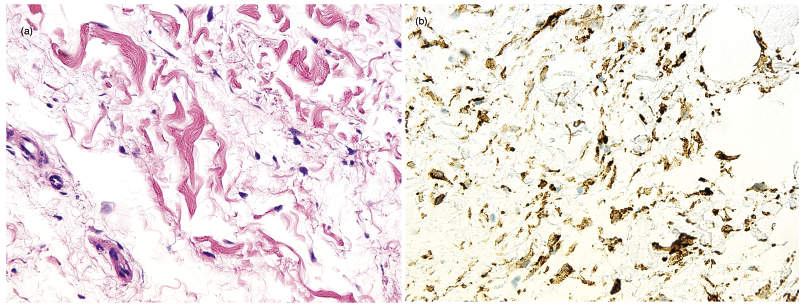 Click to show fullsize
Click to show fullsize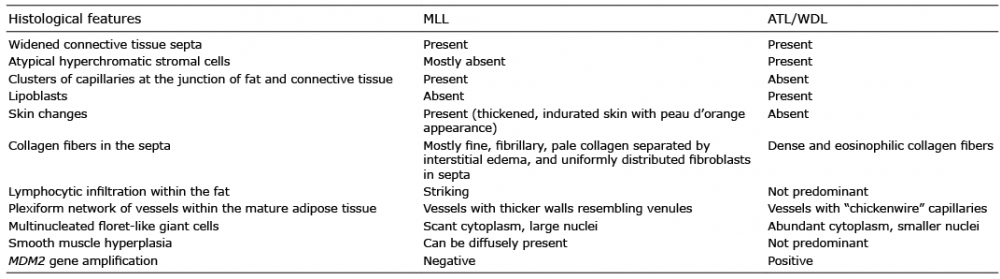 Click to show fullsize
Click to show fullsize