


1Department of Dermatology, 2Department of Epidemiology, Biostatistics and Health Technology Assessment, Radboud University Medical Center, and 3Radboud University, Nijmegen, The Netherlands
Methotrexate (MTX) and biologics are frequently used treatments for psoriasis. Exploring patients’ beliefs about their treatment may help to elucidate patients’ attitudes towards these therapies. A cross-sectional survey was conducted using the Beliefs about Medicines Questionnaire-Specific (BMQ-Specific) in patients treated with methotrexate or biologics. BMQ-Specific scores (Necessity and Concerns scales) were calculated and patients were classified as “accepting”, “indifferent”, “ambivalent” or “sceptical” towards their treat-ment. Biologics users scored higher on the Necessity scale than did methotrexate users. Both groups had lower Concerns scores than Necessity scores. A high Necessity scale was associated with a low Psoriasis Area and Severity Index score in both groups and long treatment duration in the methotrexate group. Although this study cannot make a direct comparison, it was observed that most patients on biologics could be classified as “accepting” (59%), and most patients on MTX could be classified as “indifferent” (47%). In conclusion, the BMQ-Specific is useful to identify patients with a sceptical, ambivalent or indifferent profile. These profiles may negatively influence patient’s attitude towards their medication.
Key words: psoriasis; beliefs about medicines; biologics; metho-trexate; BMQ; cross-sectional.
Accepted Dec 13, 2018; E-published Dec 13, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Marisol E. Otero, Department of Dermatology 370, Radboud University Medical Center, PO Box 9101, NL-6500 HB Nijmegen, The Netherlands. E-mail: Marisol.kooijmans-otero@radboudumc.nl
Methotrexate and biologics are the most-used systemic treatments for psoriasis. This study describes the beliefs (necessity to use, and concerns about these treatments) of patients using these treatments, and factors associated with these beliefs. Patients using biologics were found to have a higher necessity to use the treatment than those using methotrexate. A high necessity was associated with a low Psoriasis Area and Severity Index in both treatment groups, and with longer treatment duration in the metho-trexate group. Most patients using biologics could be classified as “accepting” the treatment, and most patients using methotrexate as “indifferent” to the treatment. Identifying patients with a sceptical, ambivalent or indifferent profile could be useful, because these profiles could negatively influence patient’s attitude towards their medication.
Psoriasis is a chronic, immune-mediated inflammatory skin disease, affecting 2–4% of the population in western countries (1). Moderate-to-severe psoriasis is usually treated with systemic therapies, such as metho-trexate (MTX) or biologics. Since psoriasis is a chronic disease, patients need long-term treatment to control the disease. MTX is a well-known conventional systemic therapy for continuous treatment of moderate to severe plaque psoriasis; biologics are often the next step in the treatment when conventional systemic therapies fail or are contraindicated (2, 3). It is important that patients use these therapies adequately in order to obtain disease control. It is well-known that the attitudes of patients towards medicines, including adherence, are influenced by their beliefs about the prescribed medication (4–9). The Beliefs about Medicines Questionnaire Specific (BMQ-Specific) is the most-used tool to assess these beliefs, expressed as Necessity and Concerns scores, about the prescribed medication for a specific disease. The use of this questionnaire in other chronic diseases has shown that patients who perceive high Necessity and low Concerns towards their medication are more likely to use their treatment as recommended by the prescriber (4). Assessing the balance between patients’ Necessities and Concerns about their prescribed medication helps elucidate the attitude (positive or negative) of patients towards their medication (4, 10).
Because MTX and biologics are among the most important systemic treatments for psoriasis in daily clinical practice, it is crucial to explore the beliefs of patients regarding these treatments. In addition, identifying the factors that may affect these beliefs is important in order to search for specific interventions (e.g. counselling) to prevent treatment failure. The objective of this study was therefore to explore the beliefs about medicines in patients with psoriasis treated with MTX or biologics, using the BMQ-Specific questionnaire (10). In addition, this study sought determinants that were associated with either high Necessity or low Concerns scores.
This cross-sectional survey was conducted between 6 January 2014 and 23 June 2015 at the outpatient clinic of the Department of Dermatology, Radboud University Medical Center (Radboudumc) in Nijmegen, the Netherlands. Adult patients (> 18 years) with plaque psoriasis who were treated with MTX or biologics (either adalimumab, etanercept, infliximab or ustekinumab) for psoriasis, were asked at the time of consultation to complete the BMQ-Specific. Consecutive patients visiting the outpatient clinic were asked to participate until 100 patients treated with MTX and 100 patients treated with biologics were included. This study did not require approval from an institutional review board according to ethics guidelines in the Netherlands.
The BMQ-Specific is a validated instrument that assesses beliefs about medication (10). This instrument can be adapted to a specific treatment by adding the name of the medication investigated to the questionnaire. In the current study, the BMQ-Specific was adapted to patients with psoriasis, with reference to their specific treatment for psoriasis being MTX, adalimumab, etanercept, infliximab or ustekinumab. Patients treated with a combination of systemic anti-psoriatic therapies were asked to answer the questionnaire only for their main treatment, which was a biologic in case of biologic combined with another systemic treatment.
The BMQ-Specific consists of 2 5-item scales assessing Necessity and Concerns regarding the prescribed medication. An example of a Necessity item is: “Without this medication, I would be very ill”, and an example of a Concerns item is: “These medicines disrupt my life”. Each item is measured on a 5-point Likert scale, ranging from “strongly disagree” (=1) to “strongly agree” (=5), with “uncertain” in the middle. The sum of the scores of the individual items of the Necessity scale and Concerns scale for MTX and biologics was used to calculate each scale score. The scales scores range from 5 to 25. A higher score on the Necessity scale reveals stronger beliefs in the necessity of that particular medication, while a higher score on the Concerns scale indicates stronger concerns about that particular medication (4, 10). In addition, the Necessity and Concern scales were split at the midpoint (15 points) to create 4 “attitude subgroups”: accepting (high Necessity and low Concerns), ambivalent (high Necessity and high Concerns), indifferent (low Necessity and low Concerns), and sceptical (low Necessity and high Concerns) (11).
A Necessity–Concerns Differential (NCD) was calculated by subtracting the Concerns scores of each patient from their Necessity scores. This differential results in a score ranging from – 20 to +20. Higher scores on this differential indicate higher perceived necessity than concerns. See Appendix S1 for the BMQ-Specific.
Demographic and clinical characteristics were extracted from electronic medical records. For this study, the following data were extracted: age, sex, age at onset of psoriasis, the PASI score at the time of the survey, diagnosis of psoriatic arthritis (PsA) (yes/no), disease duration at time of survey, age at start of MTX or biologic treatment, and history of systemic therapies and phototherapy for psoriasis prior to the investigated drug.
Results were reported as follows: continuous parametric variables as means with standard deviations (SDs), continuous non-parametric variables as medians with ranges, and categorical variables as percentages. This accounts for the scores of the Necessity and Concerns scales, the NCD and baseline parameters. The individual item scores were categorized into 3 categories: scores below 3 were categorized as “disagreement”, scores equal to 3 were categorized as “uncertain”, and scores above 3 were categorized as “agreement”. To avoid a judgment on the answer “uncertain”, because it is unknown what it meant to the patient, it was decided to score this answer separately. The proportions of patients per category were analysed.
Univariable linear regression analysis was performed to evaluate the possible association between the Necessity scale, Concerns scale or NCD, with general patient and treatment characteristics for the MTX and for the biologics group separately. Variables with a p-value < 0.2 in univariable analysis were analysed further using multivariable linear regression analysis with backward selection to assess which variables were independently associated with the Necessities or Concerns scales and NCD. Inclusion of candidate predictors in the regression model was set at a cut-off point of p < 0.2 in univariate testing. This is rule of thumb to select candidate predictors with potential predictive value without being too strict.
Due to the observational nature of this study, no formal statistical comparison between the MTX and biologic group was presented, because the groups were different in multiple, essential, confounding aspects which it was not possible to correct for.
Analyses were performed with SPSS version 20.0 (SPSS, Inc., Chicago, IL, USA). A p-value ≤ 0.05 was considered statistically significant.
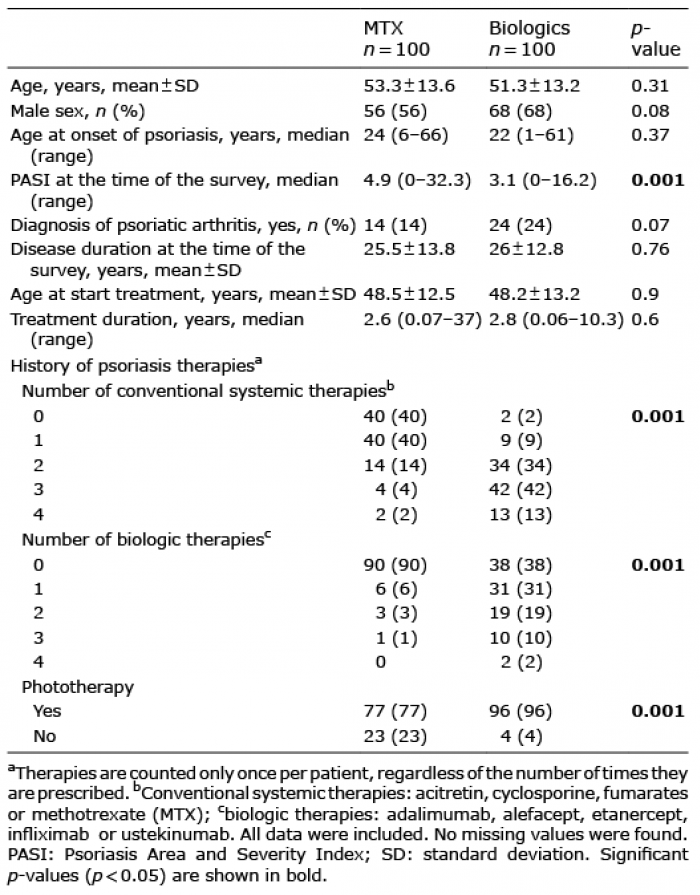
All invited patients agreed to participated and completed the questionnaire (response rate 100%). A total of 200 patients completed the BMQ-Specific questionnaire. One hundred patients were treated with MTX and 100 with biologics (adalimumab, n = 35; etanercept, n = 31; infliximab, n = 7; ustekinumab, n = 27). Table I shows the characteristics of the MTX and biologic groups.
Table I. General characteristics of patients
In the MTX group, 2 patients were treated with MTX in combination with other conventional systemic therapy (one patient started cyclosporine and MTX at the same time, due to the severity of the psoriasis at that time, and the other one started fumarates during the MTX treatment due to insufficient efficacy of MTX). In the biologic group, 15 (15%) patients received combination systemic therapy at the time of the survey (14 patients were treated with biologics in combination with MTX (adalimumab, n = 6; etanercept, n = 3; infliximab, n = 2, and ustekinumab, n = 3) and one patient was treated with ustekinumab in combination with acitretin).
Significant differences were found between the MTX and biologic groups for the baseline PASI score, the number of previous systemic therapies for psoriasis (conventional and biologics) and phototherapy (p = 0.05). The differences in patient and treatment characteristics split between 3 main biologic treatments in the study (adalimumab, etanercept and ustekinumab), are shown in Appendix S2.
Patients treated with biologics scored higher than MTX patients on all items of the Necessity scale, as shown in Table II. The highest scores in both treatment groups were found for the item “My psoriasis medication protects me from becoming worse” (MTX = 65% vs. biologics = 72%), followed by “My life would be impossible without my psoriasis medication” (MTX = 46% vs. biologics = 71%). Furthermore, in the biologics group, 62% of the patients believed that their present health depended on their psoriasis medication (reference: 42% in the MTX group) and 58% believed that their health in the future will depend on their psoriasis medication (reference: 35% in the MTX group).
Table II. Percentage of Beliefs about Medicines Questionnaire Specific (BMQ)-Specific scores per treatment group
In both treatment groups, most patients reported no concerns on all items, except for the item “I sometimes worry about the long-term effects of my psoriasis medication” where 49% of the MTX patients and 41% of the biologic patients reported concerns.
Tables III and IV summarize the mean and 95% confidence interval (95% CI) of the Necessity scale, Concerns scale and the NCD scores for the MTX and biologic groups in general and stratified for treatment duration and PASI scores. Fig. 1 shows the mean and the standard deviations (SD) of the BMQ-Specific scores split for MTX and biologics.
Table III. Beliefs about Medicines Questionnaire (BMQ)-Specific scale and Necessity–Concerns Differential (NCD) scores for methotrexate and biologics
Table IV. Beliefs about Medicines Questionnaire (BMQ)-Specific scale and Necessity-Concerns Differential (NCD) stratified by treatment duration and Psoriasis Area and Severity Index (PASI) scores
Fig. 1. Beliefs about Medicines Questionnaire Specific (BMQ-Specific) scores split for methotrexate (MTX) and biologics. Means with standard deviations of the BMQ-Specific scores split for MTX and biologics are depicted in this figure. Biol: biologics NCD: Necessity-Concerns Differential.
Patients treated for more than 1 year with MTX reported higher Necessity (p = 0.04) for the treatment than patients treated for less than 1 year (15.9 ± 4.4 and 13.8 ± 5, respectively). In the biologic group, patients with a PASI score ≤ 5 reported higher Necessity (p = 0.007) for the treatment than patients with a PASI score greater than 5 (18.7 ± 4.3 and 16 ± 4.4, respectively). Dividing the patients into 4 attitude subgroups showed that, in the MTX group, 29% of the patients could be categorized as accepting, 12% as ambivalent, 47% as indifferent, and 12% as sceptical. In the biologic group, 59% of patients could be categorized as accepting, 10% as ambivalent, 28% as indifferent, and 3% as sceptical (Fig. 2). The NCD resulted in a positive score for both treatment groups. This indicates a stronger belief in the necessity of MTX or biologics treatment than in the concerns about taking these medications (3.0 ± 5.9 and 6.3 ± 5.6, respectively). In addition, statistically significant differences (p = 0.003) were found for the NCD split for the PASI score in the biologic group (7.2 ± 5.1 and 3.5 ± 6, respectively).
Fig. 2. Classification of patients in 4 attitudes subgroups on the basis of their Necessity and Concerns (methotrexate (MTX) n = 100; biologics n = 100).
MTX group. Univariable analyses showed that age, sex, age at onset of psoriasis, PASI score at the time of the survey and MTX treatment duration were possibly associated with the Necessity scale in the MTX group when selecting those with a p-value below 0.2. The factor possibly associated with the Concerns scale was the number of previous systemic conventional therapies. The factors possibly associated with the NCD were: age at onset of psoriasis, height of the PASI score at the time of the survey and MTX treatment duration (all p-values < 0.2) (see Appendix S3 for more information on the univariable analyses).
Those variables identified in the univariable analyses were included in the multivariable regression analysis. This revealed that in the MTX group the PASI score (beta –0.246, 95% CI (–0.437;–0.055); p = 0.012) and the treatment duration (beta 0.180, 95% CI (0.042; 0.318); p = 0.011) were associated with the Necessity scale. This means that the higher the PASI score at the time of the survey, the lower the Necessity score for MTX treatment: and the longer the MTX treatment duration, the higher the Necessity score for MTX treatment. For the Concerns score, only one factor, namely “history of conventional therapies”, could be selected based on the p-value of 0.2 in the univariable analyses; however, that variable did not reach statistical significance (p = 0.08).
Regarding the NCD, also the PASI score (beta –0.249, 95% CI (–0.497; –0.002); p = 0.05) and the MTX treat-ment duration (beta 0.195, 95% CI (0.017; 0.374); p = 0.032) were found to be associated with the NCD.
Biologic group. Based on the univariable analysis, the factors possibly associated with the Necessity scale in the biologic group were: the PASI at the time of the survey and the number of previous biologic therapies. The factors possibly associated with the Concerns scale were: sex, diagnosis of PsA and the number of previous conventional therapies. The factors possibly associated with the NCD were: PASI score at the time of the survey and diagnosis of PsA (all p-values < 0.2). Again, the variables selected in this first step were included in the multivariable regression analysis. This revealed that the PASI score (beta –0.343, 95% CI (–0.598; 0.087); p = 0.01) was associated with the Necessity scale. This means, the higher the PASI score at the time of the survey the lower the necessity of the patients for the biologic treatment. None of the possible factors associated with Concerns for the biologic group in the univariable analysis reached statistical significance in the multivariable analysis. Furthermore, the PASI score (beta –0.420, 95% CI (–0.741; –0.099); p = 0.011) and the diagnosis of PsA were found to be associated with the NCD (beta 2.606, 95% CI (0.097–5.116); p = 0.042). This means that the presence of PsA at the time of the survey was associated with an increase in the belief of the patients about the necessity of the biologic treatment compared with the absence of PsA.
Table V shows a summary of the results of the multivariable regression analysis.
Table V. Summary of backward stepwise multivariable regression analysis for methotrexate (MTX) and biologics
This study found that most patients treated with MTX or biologics have a positive balance between Necessity and Concerns regarding their MTX or biologic treatment. In other words, the patients treated with MTX or biologics often reported more necessity for the prescribed medication to control their disease than concerns about taking these drugs. However, most of the patients treated with biologics could be classified as “accepting”, while most patients in the MTX group could be classified as “indifferent”.
In the Necessity scale, both treatment groups scored highest for the item “My psoriasis medication protects me from becoming worse”, followed by “My life would be impossible without my psoriasis medication” and “My health at the present depends on my psoriasis medication”. This indicates that patients acknowledge the need for medication to control their disease. With regards to the Concerns Scale, the item “I sometimes worry about the long-term effects of my psoriasis medication” was most often scored positively (40% of patients).
The high scores on the Necessity scale in the biologic group could be explained by the long history of psoriasis therapies previous to the biologic treatment. This probably means that they have failed to respond to many other therapies, which can result in feelings of dependency on biologic therapy as a last resort. These feelings could be reinforced by the fact that in the most European countries, biologic therapy can only be prescribed by failure or contraindication of conventional systemic therapies. Higher Necessity scores in patients treated with biologics than in those treated with conventional systemic therapies were also reported in the study of Michetti et al. (12) To our knowledge, the study of Michetti et al. is the only study that has investigated the BMQ-Specific questionnaire in patients with psoriasis. They focused on conventional therapies in general and on tumour necrosis factor inhibitors treatments (TNFi). The current study focused specifically on MTX as the most-used conventional treatment, and was not limited to TNFi treatments, but also included interleukin 12/23 treatment (ustekinumab). In addition, the study presented factors that might influence beliefs about medicine in patients with psoriasis.
Multivariable regression analyses revealed factors both positively and negatively associated with the Necessity scale and with the NCD. Longer MTX treatment duration was positively associated with higher Necessity for MTX treatment and with a positive NCD. Correspondingly, patients treated > 1 year reported higher Necessity for MTX than patients treated < 1 year. As an explanation, we hypothesized that patients will remain on MTX as long as their disease remains controlled, thus they experience high necessity. Another positive factor associated with the NCD, was the diagnosis of PsA in the biologic group. In the current study, the frequency of PsA in biologic patients was higher than PsA in MTX-treated patients. This could be explained by the fact that biologic treatments are prescribed when PsA does not respond to systemic conventional treatments. This might be likely to increase the necessity of these patients to receive a biologic treatment to control their arthritis and their skin disease. A negative factor associated with the Necessity scale and the NCD, in the MTX as well as the biologic groups, was a high PASI score. Correspondingly, patients with a low disease severity (PASI score ≤ 5) reported higher Necessity scores than patients with more disease activity. This could mean that when patients experience less effect of their medication, they experience less necessity for that treatment.
These results should be interpreted in the light of some limitations. First, we decided not to perform formal statistical comparisons between the MTX and biologic groups, because the groups were different in multiple, essential, aspects that are an inherent bias in non-randomized studies. Secondly, due to the nature of the current study design, it was not possible to measure the number and severity of adverse events experienced by the participants associated with current or previous treatments. Therefore, these adverse events were not included as candidate predictors in the current study. Participants’ experiences with adverse events could hypothetically lead to more concerns about treatments. However, our results showed no statistically significant differences in Concerns between the participants treated for less or more than one year in both treatment groups. Thirdly, at the time we were analysing our data, Thorneloe et al. (13), suggested that some patients with psoriasis might experience difficulties completing the BMQ and that medication beliefs were underestimated or not fully captured in the BMQ items. However, that study was based on a small number of patients recruited from a non-clinical setting, who might interpret items differently from a clinical population under systemic treatment, as in the current study. In addition, the external validity of the study may be influenced by socioeconomic and demographic characteristics, which might be different in other populations.
A strength of the current study is the 100% response rate. Therefore, the generalizability of the study is not limited by volunteer bias.
It is quite reassuring that patients expressed more necessity than concerns. However, not all patients could be classified as “accepting” with regards to their medication. Non-accepting profiles, such as sceptical, indifferent or ambivalent ones, could negatively influence a patient’s attitude towards the use of prescribed medicines. Measuring the BMQ-Specific in daily practice could reveal an individual patient profile that should be taken into account during counselling. For example, sceptical or ambivalent patients experience high levels of concerns about their medication use and might be helped by more information about a realistic risk profile of their medication. At least these patients should be monitored on therapy adherence because they could be prone to non-adherent behaviour.
MEO has acted as consultant for Eli Lilly. JMPAvdR carries out clinical trials for AbbVie, Janssen and Celgene, and received speaking fees from Abbvie, Eli Lilly and Janssen and reimbursement for attending symposia of Janssen, Pfizer, Celgene and AbbVie. Fees were paid directly to the institution. PCMvdK serves as a consultant for Merck Sharp Dome, Celgene, Centocor, Almirall, UCB, Pfizer, Sofinnova, AbbVie, Actelion, Galderma, Novartis, Janssen-Cilag, Ely Lilly, Amgen, Mitsubishi, and LEO Pharma. PCMvdK receives research grants from Centocor, Pfizer, Merck Sharp Dome, Merck Serono, AbbVie and Philips Lighting. MMBS received grants from/was involved in clinical trials from Abbvie, Almirall, Astellas, Janssen, Leo Pharma, Eli Lilly and Pfizer. She served as a consultant for Abbvie, Almirall, Boehringer Ingelheim, Janssen, Eli Lilly and Pfizer, gave lectures for Abbvie, Janssen, Eli Lilly and Pfizer and travelled with Abbvie, Eli Lilly, Pfizer and Leo Pharma to meetings; fees were paid directly to the institution. EMGJdJ has received research grants for the independent research fund of the department of dermatology of Radboud University Medical Center Nijmegen, the Netherlands from AbbVie, Pfizer, and Janssen; has acted as consultant and/or paid speaker for and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie, Janssen, MSD, Pfizer, Novartis, Lily, Amgen, Celgene and Leo Pharma; all funding is not personal but goes to the independent research fund of the department of dermatology of Radboud University Medical Center Nijmegen, the Netherlands. JSM and WK have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize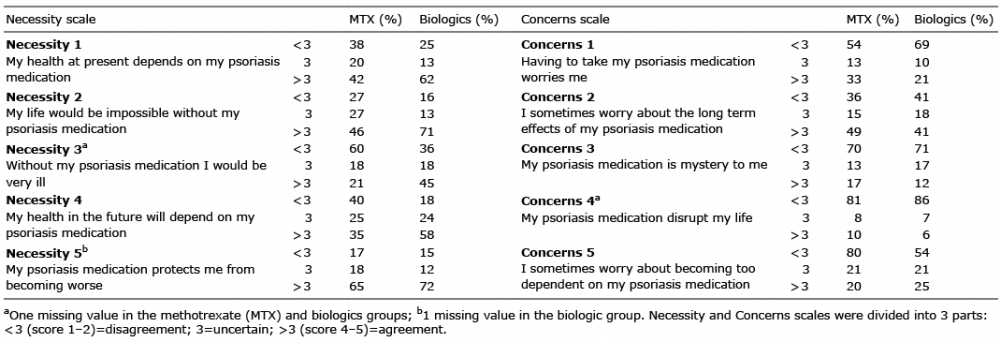 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize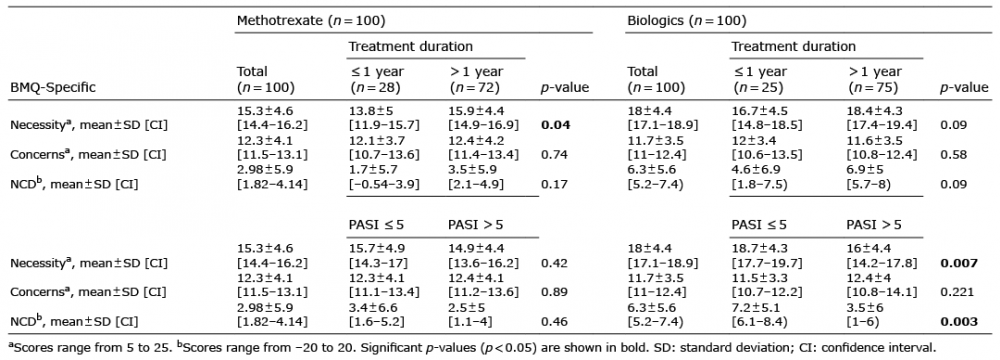 Click to show fullsize
Click to show fullsize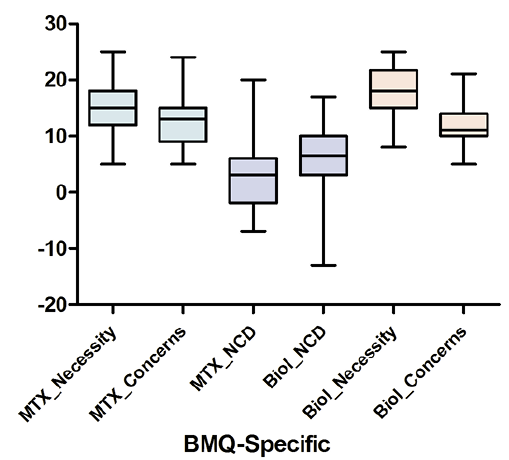 Click to show fullsize
Click to show fullsize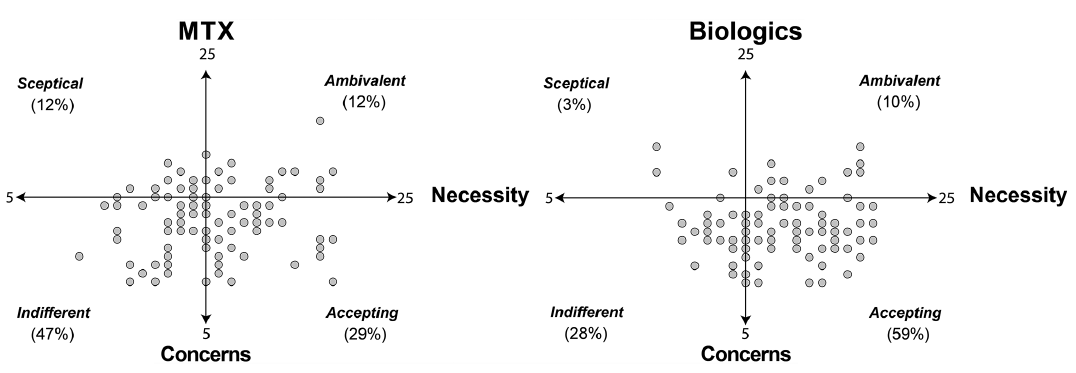 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize