


1Department of Dermatology, College of Medicine, Kaohsiung Medical University, 2Department of Dermatology, Kaohsiung Medical University Hospital, 3Department of Medical Research, Kaohsiung Medical University Hospital, 4Translational Research Center, Kaohsiung Medical University Hospital, Kaohsiung Medical University, and 5Department of Public Health and Environmental Medicine, School of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
The epidemiology of depression in patients with psoriasis has not been well defined in the Asian population. This study evaluated the epidemiological features of, and risk factors for, depression among patients with psoriasis in Taiwan. A nationwide population-based cross-sectional study was undertaken using the National Health Insurance Research Database. This study included 17,086 patients with psoriasis and 1,607,242 patients from the general population. The prevalence of depression in patients with psoriasis was 11.52%, while the prevalence of depression in the general population was 7.73% (prevalence ratio 1.49, 95% confidence interval 1.43–1.55). Multivariable analysis showed that, in patients with psoriasis, risk factors associated with depression were: age 20–50 years, female sex, low income, and major comorbid diseases, including liver cirrhosis, renal disease, cardiovascular disease and cerebrovascular disease. Therefore, the prevalence of depression is higher in patients with psoriasis, particularly in young and middle-aged women with low income and major comorbidities.
Key words: psoriasis; depression; prevalence; cross-sectional study.
Accepted Feb 7, 2019; E-published Feb 8, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Hung-Pin Tu, Department of Public Health and Environmental Medicine, School of Medicine, College of Medicine, Kaohsiung Medical University, 100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan. E-mail: p915013@kmu.edu.tw
This nationwide population-based cross-sectional study demonstrates that the prevalence of depression is higher in patients with psoriasis compared with non-psoriasis patients in the Taiwanese general population. In patients with psoriasis, risk factors associated with increased prevalence of depression include: age 20–50 years, female sex, lower income, and comorbid diseases, including liver cirrhosis, renal disease, cardiovascular disease and cerebrovascular disease. Therefore, clinicians should be vigilant for increased prevalence of depression in patients with psoriasis, especially those with the aforementioned risk factors. In addition, more clinical effort should be focused on the prevention and treatment of this serious psychiatric disorder in patients with psoriasis.
Psoriasis is a common disease with a worldwide prevalence of approximately 2%. Patients with psoriatic skin disease usually present with erythematous plaques with silver scales on the skin, while patients with psoriatic arthritis present with joint pain and deformities (1–3). The disease has been shown to have detrimental effects on patients’ functional abilities and quality of life (4–9). Recent studies have also shown that psoriasis is not only a disease that affects the skin and joints, but that it may be associated with various systemic inflammatory and cardiometabolic diseases, including diabetes (10), hypertension (11), hyperlipidaemia (12), obesity (13), metabolic syndrome (14), myocardial infarction (15) and cerebrovascular disease (16). Therefore, psoriasis is now regarded as a systemic chronic inflammatory disease.
Depression is a common and serious psychiatric disorder, characterized by low mood and loss of interest in activities (17, 18). It is an important cause of functional disability and impaired quality of life (19, 20), and may have major socioeconomic consequences (21). Severe forms of depression may lead to suicidal ideations. In patients with psoriasis, depression may also be associated with poor adherence to treatment (22), which may negatively impact clinical outcomes. Therefore, in patients with concurrent psoriasis and depression, it is important to treat both diseases in order to optimize clinical outcomes.
Although previous studies have shown an association between psoriasis and depression (23), these studies have produced heterogeneous results, with the prevalence of depression in patients with psoriasis ranging from 6% to 62% (23–25). Moreover, many of these studies were performed in single tertiary centres (with a limited number of patients), and lack a non-psoriasis control group (26). Furthermore, the prevalence and epidemiological features of depression in patients with psoriasis have not been well defined in the East Asian population and, in particular, similar studies have not been performed in Taiwan. The epidemiology of depression is likely to be different in the Taiwanese and Han Chinese population, compared with Western countries, due to differences in genetic, cultural and lifestyle factors, higher degree of social support, and lower rate of divorce and family breakdown.
This study evaluated the epidemiological features of depression in patients with psoriasis and the general population in Taiwan. A nationwide population-based epidemiological study was undertaken using the National Health Insurance Research Database (NHIRD), in order to determine whether there is an increased prevalence of depression in patients with psoriasis, and to identify the underlying risk factors.
The Taiwanese National Health Insurance System is a nationwide compulsory health insurance scheme established in 1995, which provides almost universal coverage to Taiwan’s 23 million population (current coverage rate is greater than 98%). Citizens of Taiwan are normally enrolled in the health insurance programme from the date of birth until the time of death. The information from this health insurance programme is contained within the NHIRD database, including the patient’s demographic information, International Classification of Diseases (ICD) diagnostic codes, and inpatient and outpatient claims data. The NHIRD database has been extensively used by researchers for epidemiological studies (27, 28). Patient identification information in this database was encrypted to protect patient confidentiality.
In the current study, the NHIRD (2000–2015) database was used, which was provided by the Ministry of Health and Welfare for research purposes. A total of 2,000,126 people were randomly sampled from the insured population of Taiwan in the year 2010. This database represents a closed cohort, since no additional subjects could be added once the cohort was defined. The database provides demographic and medical information for these 2 million patients from January 2000 to December 2015. According to Ministry of Health and Welfare reports, the sampled NHIRD (2000–2015) database is representative of the Taiwanese insured population, with no statistically significant differences in the distributions of age, sex, income level or geographical location between the sampled and original NHIRD database (29). Institutional review board approval for this study was obtained from our hospital.
A nationwide cross-sectional study was performed. The diagnosis of psoriasis and depression was based on ICD-9 codes: 696.0, 696.1 and 696.8 for psoriasis, and 296.2, 296.3, 300.4 and 311 for depression. In order to ensure diagnostic accuracy and reduce information (misclassification) bias, the diagnosis of psoriasis and depression was defined as 2 or more outpatient or inpatient claims with ICD-9 codes for these disorders. After excluding patients with birth date after 2000 and those with only one ICD-9 code for psoriasis or depression, 1,624,328 people were included in the current study. These patients were classified into 3 groups: patients with psoriasis with depression (n = 1,968), patients with psoriasis without depression (n = 15,118) and non-psoriasis patients in the general population (n = 1,607,242). The 2 groups “psoriasis with depression” and “psoriasis without depression” had been identified to evaluate whether the demographic and clinical characteristics differ between patients with psoriasis with and without depression, enabling the determination of possible risk factors for depression in patients with psoriasis (e.g. age, sex, income level, various comorbid diseases). The third group “general population” was identified to determine whether the demographic features, clinical characteristics (various metabolic and systemic diseases), and prevalence of depression differ in patients with psoriasis and the non-psoriasis general population.
In addition, a matched analysis was performed. The 17,086 patients with psoriasis were matched to 17,086 non-psoriasis controls from the general population (1:1 matching by age, age group, sex and income category).
Since the association between psoriasis and depression may be confounded by different comorbid disorders, the diseases that are known to be associated with psoriasis and depression were identified by their ICD-9 codes. These comorbid diseases included hypertension (codes 401.0–405.9), diabetes mellitus (codes 250.x), dyslipidaemia (codes 272.0–272.4), obesity (code 278.0), liver cirrhosis (codes 571.2, 571.5 and 571.6), renal disease (codes 580–589), cardiovascular disease (codes 410–414), and cerebrovascular disease (codes 430–438). In addition, patients were categorized as having 0, 1 or ≥ 2 comorbidities.
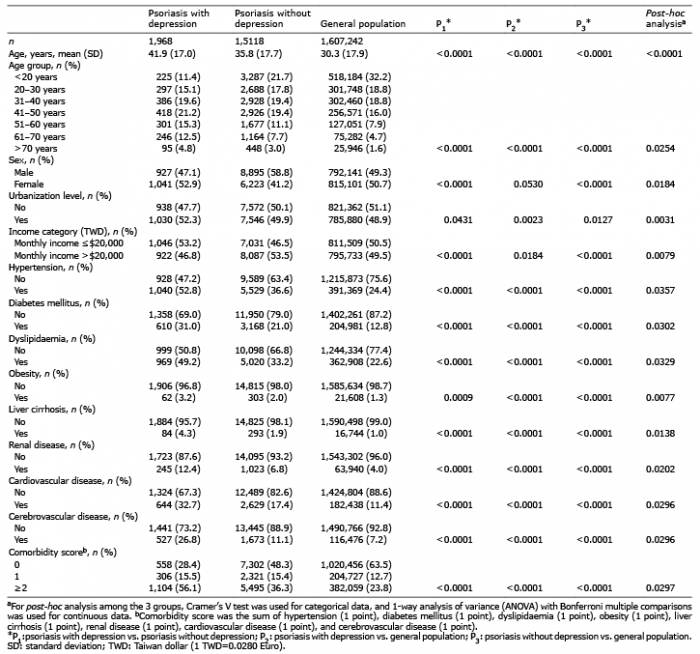
The demographic and clinical features between patients with psoriasis with depression, patients with psoriasis without depression, and non-psoriasis patients in the general population were compared using the χ2 test for categorical variables, and the t-test for continuous variables (Table I). For post-hoc analysis among the 3 groups, Cramer’s V test was used for categorical data, and 1-way analysis of variance (ANOVA) with Bonferroni multiple comparisons for continuous data.
Table I. Demographic and clinical characteristics of patients with psoriasis with depression, patients with psoriasis without depression, and non-psoriasis patients in the general population
The prevalence ratio of depression (and its 95% confidence interval (95% CI)) in patients with psoriasis relative to the general population was determined by a generalized linear model, using the log-binomial method (Table II). In the matched analysis, the adjusted odds ratio (OR) and 95% CI for depression in patients with psoriasis relative to matched non-psoriasis controls was determined using a multivariable logistic regression model, after adjustment for comorbid diseases (Table III).
Table II. Period prevalence of depression in patients with psoriasis and the general population in years 2000–2015
Table III. Odds ratio (OR) for depression in patients with psoriasis relative to matched non-psoriasis controls
In addition, a multivariable logistic regression was used to evaluate the adjusted OR and 95% CI for risk factors associated with increased prevalence of depression in patients with psoriasis (Table IV). For the logistic regression analysis of risk factors, the dependent variable was depression, and the independent variables were age group, sex, urbanization level, income category, hypertension, diabetes, dyslipidaemia, obesity, liver cirrhosis, renal disease, cardiovascular disease, and cerebrovascular disease. The logistic regression model was adjusted for age, sex, urbanization level, income category, and comorbid diseases. The Hosmer-Lemeshow test and C-statistics showed that the model fitted well with the data.
Table IV. Multivariable analysis to determine risk factors for depression in patients with psoriasis
To determine the temporal trend in the yearly prevalence of depression from years 2000 to 2015, the yearly prevalence of depression (in patients with psoriasis or the general population) and the prevalence ratio were calculated according to the following equations:
The yearly prevalence of depression in patients with psoriasis and the general population was compared using the χ2 test.
For all analyses, p < 0.05 was considered to be statistically significant. SAS software version 9.4 (SAS Institute, Cary, NC, USA) was used for statistical analysis.
There were significant differences in the demographic and clinical features of patients with psoriasis with depression, patients with psoriasis without depression, and non-psoriasis patients in the general population (Table I). Compared with patients with psoriasis without depression, patients with psoriasis with depression were older, more likely to be female, lived in urbanized area, had lower income, had higher prevalence of comorbid disorders (including hypertension, diabetes mellitus, dyslipidaemia, obesity, liver cirrhosis, renal disease, cardiovascular disease and cerebrovascular disease), and were more likely to have multiple (≥ 2) comorbidities.
Compared with non-psoriasis patients in the general population, patients with psoriasis with or without depression were more likely to be older, lived in urbanized area, had higher prevalence of comorbid disorders (including hypertension, diabetes mellitus, dyslipidaemia, obesity, liver cirrhosis, renal disease, cardiovascular disease and cerebrovascular disease), and more likely to have multiple (≥ 2) comorbidities.
In the years 2000 to 2015, the period prevalence of depression in patients with psoriasis was 11.52%, while the period prevalence of depression in non-psoriasis patients from the general population was 7.73% (Table II). The crude prevalence ratio of depression in patients with psoriasis relative to the general population was 1.49 (95% CI 1.43–1.55). Therefore, the prevalence of depression was significantly higher in patients with psoriasis compared with the general population.
When further stratified by demographic characteristics, it was found that the prevalence of depression was higher in patients with psoriasis compared with the general population in various age groups, in both males and females, in both urbanized and non-urbanized residents, and in both low- and high-income categories (Table II). In particular, the presence of psoriasis increased the prevalence of depression to a greater extent in patients < 20 years of age, in males, and in those with lower income. When further stratified by comorbidities, it was found that the prevalence of depression was higher in patients with psoriasis compared with the general population in those with and without hypertension, diabetes mellitus, dyslipidaemia, liver cirrhosis, renal disease, cardiovascular disease and cerebrovascular disease. In general, the presence of psoriasis increased the prevalence of depression to a greater extent in those without comorbidities. However, since the psoriasis group and the general population were not matched and not adjusted for age, sex or socio-economic status, the data in Table II only represent crude prevalence ratios.
Further analysis was performed using a matched design. The 17,086 patients with psoriasis were matched (by age, age group, sex and income category) to 17,086 non-psoriasis controls from the general population. As shown in Table III, the crude OR for depression in patients with psoriasis relative to matched controls was 1.44 (95% CI 1.34–1.54), and the adjusted OR after adjustment for comorbid diseases was 1.33 (95% CI 1.24–1.43). Therefore, the risk of depression was significantly higher in patients with psoriasis compared with matched non-psoriasis controls.
Multivariable analysis using logistic regression showed that, in patients with psoriasis, risk factors significantly associated with increased prevalence of depression were: age 20–50 years, female sex (adjusted OR 1.80), lower income (adjusted OR for higher income=0.79), liver cirrhosis (adjusted OR 1.77), renal disease (adjusted OR 1.19), cardiovascular disease (adjusted OR 1.52), and cerebrovascular disease (adjusted OR 2.16) (Table IV). On the other hand, urbanization level, hypertension, diabetes, dyslipidaemia, and obesity were not associated with increased prevalence of depression in patients with psoriasis.
Fig. 1 shows the time-related changes in the yearly prevalence of depression in patients with psoriasis and the general population. From years 2000 to 2015, the yearly prevalence of depression increased from 1.15% to 3.96% in patients with psoriasis and from 0.80% to 2.54% in the general population. The prevalence of depression was increased in patients with psoriasis compared with non-psoriasis patients in the general population with significant differences from 2001 to 2015 (p < 0.05). Prevalence ratios of depression in patients with psoriasis relative to the general population increased from 1.44 in 2000 to 2.11 in 2006, then decreased to 1.56 in 2015.
Fig. 1. Temporal trend in the yearly prevalence of depression in patients with psoriasis and the general population from years 2000 to 2015.
Psoriasis is a common disorder that affects approximately 2% of the world’s population (30). It is a chronic immune-mediated disease, which mainly affects the skin and joints (1–3). Psoriasis skin disease is characterized by localized or generalized erythematous plaques with silver scales on the skin, while psoriatic arthritis is characterized by joint pain and deformities. The disease varies in severity between different patients, and may have detrimental effects on the patient’s functional abilities and quality of life (4–9). Systemic treatments for psoriasis include phototherapy, oral immunosuppressive drugs (methotrexate, cyclosporine), and biological therapies (tumour necrosis factor (TNF)-α) and interleukin (IL)-17 inhibitors) (31–33).
Depression is a common and serious psychiatric disorder, which is characterized by low mood and loss of interest in activities (17). It may be associated with impairments in psychosocial functions, reduced quality of life, and suicidal ideations. Although previous reports have shown an association between psoriasis and depression (23–25), the epidemiological features of and risk factors for depression in patients with psoriasis have not been well defined in the East Asian population. In particular, similar studies have not been performed in Taiwan.
The current study showed that, compared with the general population, patients with psoriasis had a greater prevalence of various comorbid disorders, including hypertension, diabetes, dyslipidaemia, obesity, liver cirrhosis, renal disease, cardiovascular disease and cerebrovascular disease. This is consistent with previous epidemiological studies showing that psoriasis is associated with increased prevalence of various systemic inflammatory and cardiometabolic disorders (14, 15, 34, 35). Moreover, the prevalence of these comorbidities was higher in patients with psoriasis who had depression compared with patients with psoriasis without depression, suggesting that they may be possible risk factors for depression in patients with psoriasis.
In particular, this study found that the prevalence of depression was 11.52% in patients with psoriasis and 7.73% in the general population, with a crude prevalence ratio of 1.49 (95% CI 1.43–1.55). Therefore, the prevalence of depression was higher in patients with psoriasis compared with the general population. Moreover, further analysis using a matched design (patients with psoriasis matched to non-psoriasis controls by age, age group, sex and income category) showed that the crude OR for depression in patients with psoriasis vs. matched controls was 1.44 (95% CI 1.34–1.54), and the adjusted OR after adjustment for comorbid diseases was 1.33 (95% CI 1.24–1.43). Therefore, the association between psoriasis and depression still exists after controlling for demographic features and comorbid diseases. These results are consistent with a previous meta-analysis showing that the prevalence of depression in patients with psoriasis was 12% when diagnosed by ICD codes, and 19% when diagnosed by Diagnostic and Statistical Manual of Mental Disorders IV (23). The meta-analysis also showed that patients with psoriasis were 1.57 times more likely to experience depression compared with controls, which was slightly higher than the crude and adjusted OR obtained in the current study. This may be due to differences in genetic, cultural, social and lifestyle factors between patients in Taiwan and Western countries.
In addition, temporal trend analysis demonstrated that the yearly prevalence of depression in both patients with psoriasis and the general population increased from years 2000 to 2015, and the yearly prevalence of depression was higher in patients with psoriasis compared with the general population throughout this time period. Further studies are required to determine whether the increase in prevalence of depression over this time-frame is due to an increase in diagnostic rate for depression, or a true increase in disease prevalence.
There may be a number of explanations for the association between psoriasis and depression. Psoriasis often has a negative impact on a patient’s physical appearance, which may lead to low mood, loss of self-esteem, stigmatization and social withdrawal (36). This may result in impaired quality of life and increase the likelihood of experiencing depression (37, 38). Moreover, patients with psoriasis may have greater prevalence of comorbid cardiometabolic and systemic disorders, which may have adverse impacts on their functional abilities and quality of life, thus leading to depression (34).
In addition, the production of inflammatory cytokines may play a role in the association between psoriasis and depression. Th1 and Th17 cells are known to be important in the pathophysiology of psoriasis (39, 40). The blood and skin plaques of patients with psoriasis have been shown to contain higher levels of Th1 and Th17 cytokines (41, 42). Similarly, patients with depression have higher serum levels of Th1 and Th17 cytokines, which may contribute to the pathogenesis of depression (43–46). Moreover, treatment of patients with psoriasis with TNF-α or IL12/23 antagonists has been demonstrated to reduce depressive symptoms (47–49). Treatment of patients with depression with antidepressants has also been shown to restore the abnormal cytokine profile (50, 51), and decrease the need for systemic anti-psoriatic medications in patients with psoriasis (52). Therefore, it is possible that shared cytokine pathways may play an important role in the association between psoriasis and depression.
Furthermore, multivariable logistic regression analysis demonstrated that, in patients with psoriasis, demographic risk factors associated with increased prevalence of depression were age 20–50 years, female sex and lower income. This is consistent with previous epidemiological studies showing higher risk of depression in young to middle-aged females with low socioeconomic status (53, 54). The increased prevalence of depression in women may be due to hormonal factors, psychosocial stressors, or behavioural differences (55). In addition, comorbid diseases, including liver cirrhosis, renal disease, cardiovascular disease and cerebrovascular disease, were found to be associated with increased prevalence of depression in patients with psoriasis. Since these comorbid diseases affect major organs, they are more likely to be associated with significant symptoms, and may negatively affect the patients’ physical functioning, quality of life and socioeconomic status. Thus the contribution of these comorbidities to the risk of depression in patients with psoriasis is conceivable. On the other hand, hypertension, diabetes, dyslipidaemia and obesity were not significantly associated with prevalence of depression in patients with psoriasis. Since these metabolic disorders may have less impact on the patients’ physical functions and quality of life, they are less likely to lead to depression in patients with psoriasis.
The design of this study has a number of strengths. First, this is a nationwide population-based study using a large sample of patients, and therefore the findings may be generalizable to the entire Taiwanese population. Secondly, the Taiwanese Health Insurance System offers universal and compulsory coverage to more than 98% of the Taiwanese population, which avoids potential selection bias. Thirdly, the NHIRD database contains medical records from all the hospitals and clinics in Taiwan, and hence the information may be more comprehensive compared with study designs that involve questionnaires (which may be affected by recall bias) or review of medical charts (which may not contain medical records from other hospitals and clinics). Fourthly, a matched analysis was performed in addition to the cross-sectional study, which allowed us to determine whether psoriasis is significantly associated with depression after controlling for demographic features (age, sex, income level) and comorbid diseases.
A number of limitations also need to be considered in this study. First, the cross-sectional nature of the current study means that the temporal relationship between the onset of psoriasis and development of depression cannot be analysed, and some confounding factors may not have been fully adjusted for. Secondly, studies using information from insurance claims data may be subject to disease misdiagnosis or miscoding. However, since both psoriasis and depression have characteristic clinical presentations, misdiagnosis of these diseases is less likely to occur. Moreover, the lack of a referral system in Taiwan means that patients usually see a specialist at their first medical visit, and therefore the diagnoses of psoriasis and depression are likely to have been made by dermatologists or psychiatrists. Lastly, information regarding disease severity, laboratory values, education, occupation, marital status, and lifestyle factors are not available in the NHIRD database, and therefore these variables could not be analysed in the current study.
The findings of this nationwide population-based cross-sectional study demonstrate that the prevalence of depression is higher in patients with psoriasis compared with non-psoriasis patients in the Taiwanese general population. In patients with psoriasis, risk factors associated with increased prevalence of depression include age 20–50 years, female sex, lower income, and comorbid diseases, including liver cirrhosis, renal disease, cardiovascular disease and cerebrovascular disease. Therefore, clinicians should be vigilant for the increased prevalence of depression in patients with psoriasis, especially those with the aforementioned risk factors. In addition, more clinical efforts should be focused on the prevention and treatment of this serious psychiatric disorder in patients with psoriasis.
This work was supported by grants from the Ministry of Science and Technology, Taiwan (104-2314-B-037-048-MY3, 107-2314-B-037-060, 107-2314-B-037-088) and Kaohsiung Medical University Hospital (KMUH105-5R51, KMUH106-6R63). The data source was from Health and Welfare Data Science Center, Ministry of Health and Welfare (HWDC, MOHW).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize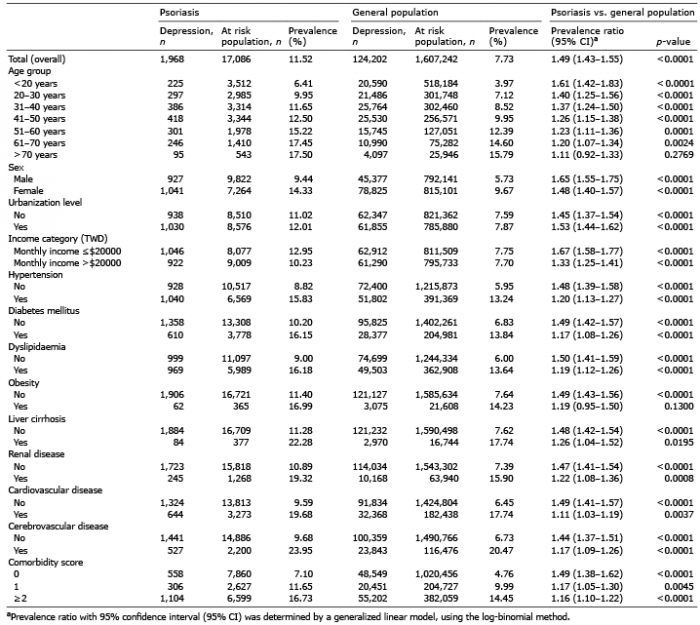 Click to show fullsize
Click to show fullsize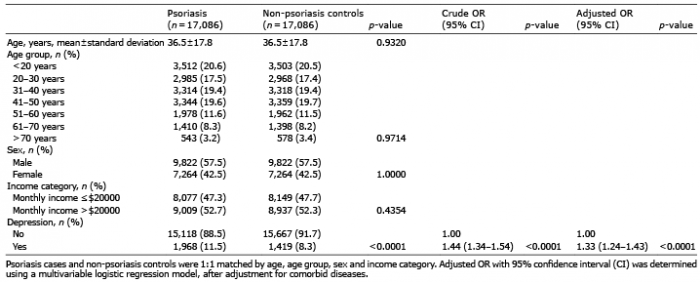 Click to show fullsize
Click to show fullsize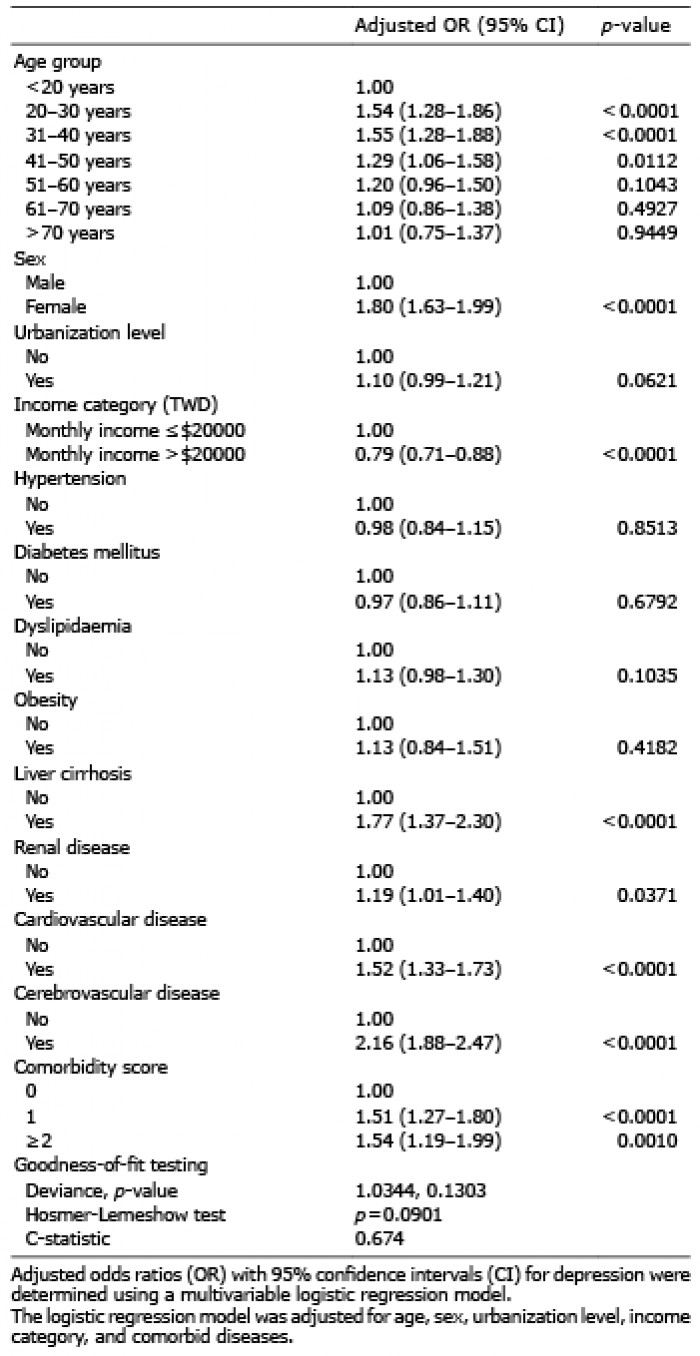 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize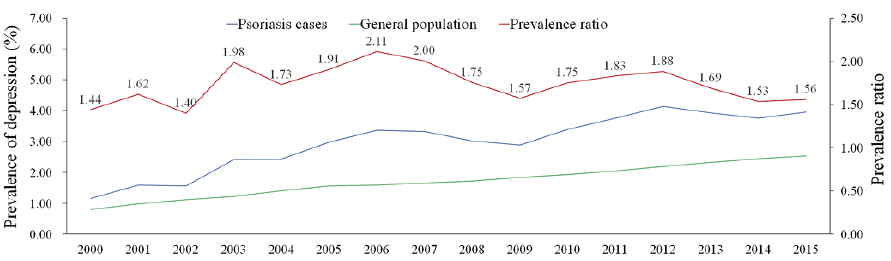 Click to show fullsize
Click to show fullsize