


1Research Laboratory on Neuropeptides (IBIS), 2Virgen del Rocío University Hospital, Pediatric Intensive Care United (PICU), Av. Manuel Siurot s/n, ES-41013 Seville, and 3Institute of Neurosciences of Castilla y León (INCYL), Laboratory of Neuroanatomy of the Peptidergic Systems, University of Salamanca, Salamanca, Spain. E-mail: miguel.mmunoz@gmail.com
Accepted Feb 7, 2019; E-published Feb 8, 2019
A recently published study of 8 patients with cutaneous T-cell lymphomas (CTCL) treated with aprepitant (1) reported that the neurokinin-1 receptor (NK-1R) antagonist aprepitant did not completely modify CTCL disease activity. The authors concluded that these findings do not support future research focused on the anti-lymphoma action of NK-1R antagonists (1). The same group publi-shed another study of 17 patients, which reported that, in primary CTCL, there was an improvement in refractory pruritus, and that aprepitant was safe, well-tolerated and effective for treatment of severe chronic itch in patients with CTCL who failed to respond to classical antipruritic treatments (2). The latter study is in agreement with the data suggesting that, in the skin, NK-1R antagonists play an important role in anti-itch activity (2). These authors reported that the best antipruritic response was found in lymphomas limited to skin (stages IB–IIB) and non-erythroderma cutaneous lesions (stage T4) (2). In both studies (1, 2), aprepitant (standard 125–80–80 mg) was administered every 2 weeks for a mean of 20 weeks, or weekly for 8 weeks. In standard clinical practice, aprepitant (first day 125 mg; second day 80 mg; third day 80 mg) is used to treat chemotherapy-induced nausea and vomiting.
The aim of this short correspondence is to explain why, in the studies described above (1, 2), the authors found that aprepitant did not modify global disease activity in CTCL or, in other words, why aprepitant exerted antipruritic, but not antitumour, action.
It is known that undecapeptide substance P (SP) is a main mediator in pain (pruritus is a type of pain) and neurogenic inflammation, and that tumour cells express SP and NK-1R (e.g. T-lymphocytes and human IM-9 B-lymphoblasts express 7,000–10,000 and 25,000–30,000 NK-1R per cell, respectively) (3, 4). After binding to NK-1R, undecapeptide (through autocrine and/or paracrine mechanisms) promotes mitogenesis/migration of tumour cells, an antiapoptotic effect in these cells and an angiogenic effect (3). In later-stage CTCL (stages IIB–III), a significant increase in SP level has been reported; however, the undecapeptide level in erythroderma (stages T4) has not been investigated (in this case it is possible that the SP level was higher) (5). By contrast, NK-1R antagonists (e.g. aprepitant), in a concentration-dependent manner, block the above-mentioned actions mediated by SP (3). There are 2 isoforms of NK-1R; full-length (fl-NK-1R) and truncated forms (tr-NK-1R) (3). In papillary or epidermal CD3+ T lymphocytes of patients with CTCL, the expression of fl-NK-1R is lacking (1, 5). However, it is important to note that the anti-NK-1R antibody used to detect the fl-NK-1R form in papillary or epidermal CD3+ T lymphocytes was unable to detect the truncated form (5), which means that the presence of the tr-NK-1R form in these lymphocytes is unknown. In sum, fl-NK-1R has not been observed in malignant CTCL cells, but tr-NK-1R has not being studied (5). Thus, the presence of the truncated form must not be discounted until it is determined whether truncated receptors are present in malignant CTCL cells. It is also important to note that tumour cells predominantly express the tr-NK-1R isoform (e.g. acute lymphoblastic leukaemia T (ALL) cells express both isoforms of NK-1R and overexpress NK-1R 30-fold higher than non-tumour cells) (4, 6).
Many in vitro and in vivo studies have reported the antitumour action of NK-1R antagonists. For example, aprepitant exerts an antitumour action against acute leukaemia T-ALL cells (IC50 and IC100 were 19.5 and 45.6 µM, respectively) (6). Extrapolating these concentrations to mg/kg/day, the doses are approximately 10.5 and 24.3 mg/kg/day, respectively. That is, in the studies mentioned above (1, 2), the concentration of aprepitant had an antipruritic effect, but, to exert an antitumour effect, the patients should be given a dose of approximately 25 mg/kg/day. Moreover, to obtain an antitumour effect, aprepitant should be administered daily, and hence treatment should not be stopped, as it was in the previous studies (1, 2) focused on the antipruritic effect of aprepitant (this drug is eliminated in 24 h). In sum, the antipruritic (125–80–80 mg aprepitant) dose administered to patients with CTCL (1, 2) is much lower than is necessary to exert an antitumour effect (25 mg aprepitant/kg/day).
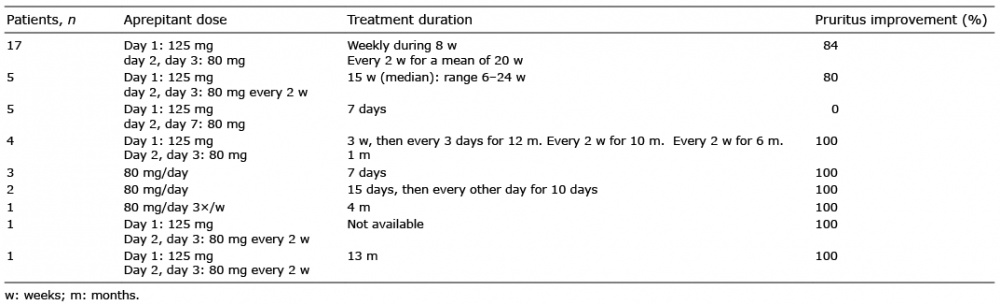
Thus, in patients with CTCL, a higher dose of aprepitant than was used in these studies (1, 2) will exert both antipruritic and antitumour action. However, it is not known if the antitumour dose suggested here is safe. This key question must be resolved in further clinical studies. Doses of aprepitant higher than that used in standard clinical practice (120–80–80 mg) have been tested. In all cases, aprepitant was safe and well tolerated. Thus, aprepitant (300 mg/day, during 45 days) had the same antidepressant effect as paroxetine, and similar side-effects to those of placebo (7). However, in another clinical trial, aprepitant (160 mg/day, during 45 days) did not have an antidepressant effect (8). This was because the dose of aprepitant did not reach the threshold needed to exert a therapeutic effect, in relation to the amount of NK-1Rs that the drug needs to block. Moreover, in a hepatoblastoma xenograft mouse model, aprepitant (80 mg/kg/day for 24 days) decreased tumour growth (reduced tumour volume and weight) (9). In breast cancer metastasis to the brain, no side-effects have been reported and an improvement in the clinical condition was reported when the patient was treated with aprepitant (80 mg/day initially, followed by an increase to 125 mg/every third day for 7 months) (10). Finally, in patients with HIV, administration of aprepitant (375 mg/day for 2 weeks) was safe and well tolerated. In aprepitant-treated patients, the number of CD4+ PD-1-positive cells and plasma levels of soluble CD163 and SP decreased (11). Improvement in pruritus has been reported in patients with CTCL treated with aprepitant (Table I) (2, 12–14).
Table I. Patients with cutaneous T-cell lymphomas (CTCL) treated with aprepitant
In conclusion, in patients with CTCL, it is possible that aprepitant exerts both antipruritic (stages III and erythro-derma IV included) and antitumour therapeutic effects when an adequate dose (> 20 mg/kg/day) is administered daily for at least 45 days. This is in agreement with data reporting that, by using a higher dose of aprepitant than is used in standard clinical practice, and by increasing the number of days on which aprepitant is currently administered, aprepitant (NK-1R antagonists) could be an excellent candidate to be used as an antitumour strategy (15). Thus, in patients with CTCL, a clinical assay must be performed to test the antitumour action of NK-1R antagonists (aprepitant 25 mg/kg/day, for a long period of time according to the response to treatment).
The authors thank Ms Diane Haun for editing the English text.
USPTO Application number 20090012086 “Use of nonpeptidic NK-1 receptor antagonists for the production of apoptosis in tumor cells” (Miguel Muñoz).


 Click to show fullsize
Click to show fullsize