


1Center for Chronic Pruritus, Department of Dermatology, University Hospital Münster, 2Institute of Biostatistics and Clinical Research, University of Münster, Münster, 3German Center for Health Services Research in Dermatology (CVderm), Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Few studies have validated standard measurement instruments for evaluation of chronic pruritus. The Chronic Pruritus Tools Questionnaire PRURITOOLS assembles a set of instruments for the assessment of pruritus, such as the visual analogue scale (horizontal 100-mm line), numerical rating scale (0–10), verbal rating scale, and information on pruritus quality and improvement during therapy. This study, with 40 subjects, analysed PRURITOOLS regarding convergent validity and test–retest reliability (60 min), followed by a feasibility questionnaire. Test–retest reliability for PRURITOOLS items was excellent (intraclass correlation coefficient 0.84–1). Strong to very strong correlations between the pruritus intensity scales indicated convergent validity. The feasibility questionnaire showed an overall acceptance of PRURITOOLS, and the majority of subjects (82.5%) considered it an appropriate questionnaire to measure pruritus. In conclusion, PRURITOOLS offers validated tools for rapid pruritus assessment in routine care or endpoints of clinical trials.
Key words: numerical rating scale; itch; prurigo; visual analogue scale; dynamic pruritus scale; worst pruritus.
Accepted Mar 4, 2019; E-published Mar 5, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Claudia Zeidler, Center for Chronic Pruritus, Department of Dermatology, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: Claudia.Zeidler@ukmuenster.de
Itch lasting for longer than 6 weeks (chronic pruritus) is one of the main symptoms in dermatology and can appear not only in dermatological disorders, but also in systemic, neurological and psychological diseases. Chronic pruritus is often difficult to treat and has a high level of impact on a patient’s quality of life. There are only a few validated standard measurement instruments available for the evaluation of chronic pruritus, which makes it difficult to assess this symptom objectively. This study validated the Chronic Pruritus Tools Questionnaire PRURITOOLS, which assembles a set of tools for the assessment of pruritus and can now be used in routine care or in clinical trials.
Chronic pruritus (CP) is, according to the International Forum for the Study of Itch (IFSI), defined as an itching sensation lasting over 6 weeks (1). This distressing symptom is associated with a variety of dermatological conditions and non-dermatological diseases, such as chronic renal insufficiency or liver diseases (2–5). Pruritus, described as the urge to scratch the skin to obtain relief, can have a high level of impact on quality of life (1, 6–8). New therapies are needed, since current treatments do not control pruritus in all patients and are often accompanied by side-effects (9–11). Collecting information on different aspects and attributes of pruritus is important for feedback on treatment efficiency and comparability of the assessed aspects across different studies. The problem of assessing CP in daily routine and clinical trials is that pruritus is a subjective multidimensional symptom, the presentation of which varies from patient to patient. Finding a suitable, objective method of measurement is therefore challenging (12) and thus patient-reported outcomes (PRO) currently constitute the standard tools for assessment of pruritus. Validated and reliable PRO measurement tools evaluating CP in patients are required in order to collect and process information about CP both individually and collectively, especially in clinical trials. Not only for the assessment of chronic distress, but also for a more active involvement of patients in shared decision-making about treatment of their CP, simple and reliable tools measuring progress and outcome are required (13). However, although pruritus is prevalent in 17% of the adult population (assessed in a large cohort of the working age population in Germany) (7), to date there are only a few validated standard measurement tools for the evaluation of pruritus. Unidimensional scales, such as the visual analogue scale (VAS), numerical rating scale (NRS) or verbal rating scale (VRS), have been validated in several languages (14, 15) and thus provide a method to obtain data to establish baselines for pruritus and accompanying symptoms in clinical trials (14). They show good reproducibility, are easily understood by the general population and have good psychometric properties (16). However, the qualities of sensory symptoms (pruritus, burning, stinging) assessed, recall periods and reference points (worst/mean pruritus) of the intensity scales used in different trials and in routine care vary largely and not all scales currently in use are validated. The aim of this study was to close the gap of pending validations and evaluate a set of tools that can be used in clinical practice and trial. Here, we validated, for the first time, a VRS for stinging and burning sub-qualities in patients with CP. In addition, one of the scales validated is the Dynamic Pruritus Score (DPS), a novel instrument that assesses the patients’ global impression of change in pruritus (17). In this study, we broke down the information collected by the DPS into single questions in order to collect the same information in a simpler fashion. Our newly developed PRURITOOLS covers a comprehensive set of VRS, VAS, NRS, and carefully selected questions on improvement of symptoms (based on the DPS) in patients with CP. With PRURITOOLS, a 2-page hand-out consisting of 12 validated items, we aimed to assemble suitable tools for the assessment of CP, which serve for selection of instruments in routine care or endpoints in clinical trials.
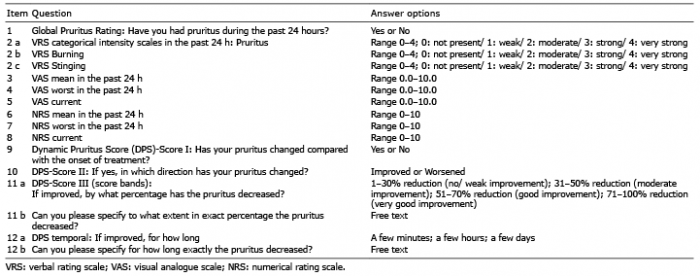
PRURITOOLS (Table I) was developed based on already validated instruments (e.g. VRS, VAS) with modification of the recall periods (current pruritus, past 24 h), categorical qualities (pruritus, burning, stinging assessed on the VRS) and reference points (mean and worst pruritus). The original Dynamic Pruritus Score (DPS) was subdivided into Questions 9 (DPS I), 10 (DPS II), 11 (DPS III) and 12 (DPS temporal).
Table I. PRURITOOLS questions
Routine patients presenting at the Center for Chronic Pruritus at the University Hospital Münster, Germany, were recruited from September 2014 to March 2015. Adults (≥ 18 years old) with CP reporting a score of 2 or more out of 10 on the NRS were asked to participate in the study. Prior to any study-specific procedures, all subjects gave written informed consent for data collection and analysis. The study was performed in accordance with the Declaration of Helsinki with later revisions. The ethics committee of the University of Münster approved the validation trial (No. 2014-385-f-S), which is registered at the German Clinical Trials Register DRKS00009902.
After providing informed consent subjects completed PRURITOOLS and were also asked to complete routine questionnaires for pruritus intensity evaluating different recall periods and reference points (VAS: mean pruritus in the past 4 weeks, worst pruritus in the past 4 weeks, mean pruritus in the past 24 h; NRS: mean pruritus in the past 24 h; VRS: mean pruritus in the past 24 h). Subjects then completed the original DPS, the Dermatology Life Quality Index (DLQI) and ItchyQoL, a pruritus-related quality of life questionnaire (with the subscales Symptom, Emotion and Function, comprising 22 questions), as well as the Hospital Anxiety and Depression Scale (HADS with subscales Anxiety (HADS-A) and Depression (HADS-D), 14 questions) (17–20). After 60 min, subjects were asked to complete PRURITOOLS questionnaire again, along with a feasibility questionnaire of 10 questions on the usability, readability and convenience of the assessment of pruritus via PRURITOOLS.
Statistical analyses were performed with IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA). All items were tested for test–retest reliability (using Cohen’s kappa for nominal variables and intraclass correlation coefficient (ICC) for continuous variables), convergent validity (inter-item correlations). The Mann–Whitney U test was applied to compare independent subgroups of continuous or ordinal variables, while the Kruskal–Wallis test was used to compare a continuous variable between 3 independent diagnosis subgroups. Differences between 2 independent subgroups of categorical variables were tested using the χ2 test. Pearson product-moment correlation coefficient and the Spearman’s rank correlation coefficient were used to estimate the strength of the relationship between 2 continuous or ordinal variables. Statistical significance was assumed if p < 0.05 (2-sided). Exploratory factor analysis was used to identify the pattern of correlations within items 2–8 (a set of the pruritus intensity and quality variables).
Based on previous studies (18), 40 patients (22 women; age (mean ± standard deviation (SD)): 58.4 ± 16.7 years) with CP were included (Table II). The average pruritus intensity in the past 24 h assessed on the NRS was 5.73 ± 2.55. No statistical difference in pruritus intensity between the underlying disease categories was found (p = 0.686). In addition, no correlation was found between pruritus intensity and the duration of CP (Spearman’s rho r = 0.04; p = 0.808). The results of all assessed parameters including PRURITOOLS data are displayed in Tables II–IV. Exploratory factor analysis showed that PRURITOOLS items 1–8 (Table I) had acceptable distributions and good internal consistency. There was no significant difference between the results of PRURITOOLS considering age (p > 0.6), sex (male/female; Mann–Whitney U test, p > 0.6) and diagnosis subgroups (Kruskal–Wallis test, p > 0.6) of the subjects.
Table II. Subject demographics and routine instruments
Table III. PRURITOOLS data including mean, standard deviation, median, maximum and minimum (n = 40)
Table IV. PRURITOOLS data of Dynamic Pruritus Score (DPS) (n = 40)
ICCs of the pruritus intensity scales ranged from 0.843 (item 5, VAS current) to 0.98 (item 6, mean pruritus-NRS in the last 24 h; Table V). The ICCs of the VRS intensity scales (range 0–4: 0: not present, 1: weak, 2: moderate, 3: strong, 4: very strong) ranged from 0.936 (item 2c, stinging) to 0.974 (item 2 a, pruritus).
The kappa coefficient of the DPS I and DPSII (items 9 and 10, pruritus change) was significant at 1.0 (p < 0.001), while ICC of DPS III (items 11A and 11B, pruritus improved/worsened) varied between 0.91and 1.0 (p < 0.001) (Table V).
Table V. Analysis of test–retest reliability: correlation coefficients and subject responses
Tables VI and VII show the convergent validity of PRURITOOLS with regard to each item of the routine questionnaires. The correlation between the routine pruritus intensity scales and PRURITOOLS pruritus intensity scales varied from 0.630 to 0.937 (strong to very strong correlations). As for the routine pruritus intensity scales and PRURITOOLS VRS categorical intensity scales for different qualities, such as pruritus, burning and stinging, the correlation coefficient ranged from 0.401 to 0.868 (moderate to strong). All other parameters, including DLQI, ItchyQoL (total score), ItchyQoL subscores symptom, function and emotion, HADS-A and HADS-D, showed low to strong correlations to PRURITOOLS (Tables VI, VII).
Table VI. Convergent validity (PRURITOOLS item 2 to 8 vs. routine VAS, NRS, original DPS, DLQI, ItchyQoL and HADS)
Table VII. Convergent validity (PRURITOOLS Item 9-12 vs. routine VAS, NRS, original DPS, DLQI, ItchyQoL, HADS)
A significant association was found between the mean VAS of the past 24 h and DPS-Score II (item 10, improved vs. worsened) and between the original DPS and DPS-Score II: if the pruritus had improved, the mean VAS of the past 24 h was 3.36 points lower and the original DPS was 29.61 points higher than in the group in which the pruritus had worsened (p = 0.024; p = 0.002). Strong correlations were found between the mean VAS-score of the past 24 h and item 10 (difference: 3.36 points, p = 0.024) and item 12 (r = –0.734, p = 0.004), respectively, as well as between the mean NRS-score of the past 24 h and item 11b (r = –0.755, p = 0.012). The original DPS also correlated with item 10 (difference: 29.61 points, p = 0.002) and item 11b (r = 0.796, p = 0.006). Between the remaining routine parameters and items 9 to 12, again, only low correlation coefficients were found.
All but one patient (n = 39, 97.5%) felt sufficiently informed about the purpose of PRURITOOLS. Ninety-five percent of patients (n = 38) thought that the individual questions were phrased clearly. In mean, it took them 7.51 ± 5.82 min to complete the questionnaire (Table VIII).
Eight subjects (20%) felt that important aspects were not expressed. Specifically, they felt that PRURITOOLS does not address the psychological welfare of the patient, and that the time-frame in which pruritus is evaluated via the questionnaire is too short (just covering the past 24 h). On the other hand, 22.5% (n = 9) of the subjects thought the questionnaire was too long and 20% (n = 8) felt that they had to put too much effort into answering the questions. The majority of subjects (n = 27, 70%) had no difficulty in finding answers for the questions. Those who did (n = 8, 20%), found items 11 and 12 to be most difficult. Twenty-seven subjects (67.5%) stated that they would participate in a clinical trial including PRURITOOLS. Overall, 33 subjects (82.5%) felt that PRURITOOLS is an appropriate tool to measure CP.
Table VIII. PRURITOOLS feasibility evaluation among subjects
The proper validation of health measurement instruments for the use in routine care and clinical trials is a prerequisite for data interpretation and the establishment of international standards (19). There is still a lack of consensus on the optimal assessment of CP, including the recall period of the pruritus intensity scales VAS, NRS and VRS. Several approaches have been tried in the past in randomized controlled trials, such as recall periods of “just now”, 24 h, 3, 5 or 7 days or the calculation of means of single assessments over 3–7 days: the interpretation of the data is difficult, as patients give a number for a certain period of time without providing details on fluctuations in pruritus intensity, quality or localization. To minimize potential fluctuations, we selected a recall period of 24 h for PRURITOOLS. This allows a once-daily assessment and potentially enhances the compliance in clinical trials compared with a 12-h recall period necessitating twice daily assessment. Here we could show that a 24-h assessment produces reliable data. Most of the patients felt that the time-frame in which the pruritus was evaluated was adequate. The test–retest reliability testing provided excellent results, with ICCs between 0.84 and 1.0. The time between tests (60 min) was selected to reduce the risk of distractions by the natural fluctuation of itch and by the possible doctors’ visit in between the tests. On the other hand, it cannot be excluded that some patients might remember their first answers, resulting in a high test–retest reliability. Convergent validity tests showed strong to very strong correlations between the pruritus intensity scales (up to 0.937), confirming the comparability of the scales used. The population included in this study was already familiar with these tools in general, as we regularly use them in our pruritus centre (20). Thus, there were few missing data, a quick response time and very good feasibility responses, including the question on the face validity. However, importantly, prior to the first use of such instruments, patients with CP need to be familiarized with the tools (14, 15). While explaining the written instructions of the instruments, it is important that physicians and/or study nurses avoid their own interpretation, such as, for example, “a value of 3 is like a mosquito bite” as this may produce considerable bias.
For the convergent validation of PRURITOOLS, pruritus intensity instruments as used in our routine care and according to a previous tool validation (14), but also additional well-established tools, such as the DLQI, ItchyQoL and HADS questionnaire were analysed. The results of the convergent validation analysis solidified the high validity of PRURITOOLS. Interestingly, VAS worst, but also to a slightly lesser degree NRS worst, showed the highest correlations with convergent variables compared with the average or current itch intensity. These results may be a first hint for a superior association of VAS worst and NRS worst in regard to correlations with quality of life questionnaires compared with the means of VAS and NRS. However, studies with larger collectives are necessary in order to prevent over-interpretation of our results. There was no significant correlation with one of the HADS subscales. An explanation could be that the subscores for HADS were slightly low in this study group, so that the intensity of pruritus has no negative impact on the HADS scores.
The original DPS was developed as an instrument to assess the patient’s impression of change of pruritus in a certain period (17). The original version showed moderate correlations with PRURITOOLS pruritus intensity scales reflecting a different construct (change of pruritus vs. current pruritus intensity). The novel DPS was basically broken down into 3 questions (items 9–11a). Due to its pyramid structure of subsequent questions, the modified DPS was challenging to compare with established parameters of existing questionnaires and scales. However, the data obtained in this study suggest a good separation between these patients who had an improvement in the intensity of pruritus and those whose pruritus had worsened.
Good correlations with significant separation between the answers for the pruritus intensity scales. In addition, the original and modified DPS showed good correlations, encouraging further research and the use of the novel DPS instrument on mobile applications for which it was developed. In another project, we already used the modified DPS on the ItchApp© for Android smartphones (18). In the future, the DPS could be an interesting instrument that allows the definition and validation of responder populations in clinical trials.
The PRURITOOLS has been designed as a collection of validated instruments with the same recall timescale of 24 h for assessment of CP of any origin. Validation data suggested a superiority of VAS worst and NRS worst over the mean VAS/NRS tools. PRURITOOLS will serve for instrument selection in routine care and endpoint selection in clinical trials, but might also be used as a whole in patients to obtain a comprehensive overview on the pruritus level. In order to test the sensitivity in the future, PRURITOOLS must be tested before and after treatment.
This article was supported by the German Federal Ministry of Education and Research (BMBF; No. 01KG1305 to SST), and by the European Academy for Dermatology and Venereology (EADV, No. 2016-012 to MP). We acknowledge support from the Open Access Publication Fund of the University of Muenster.
The questionnaire is available, on request, from sonja.stander@ukmuenster.de.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize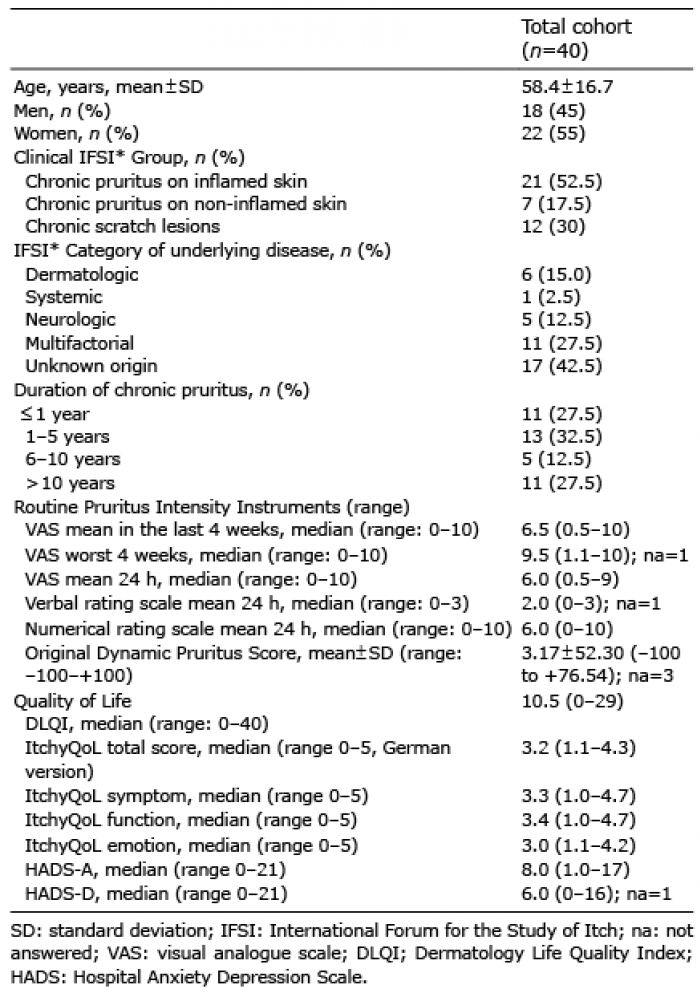 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize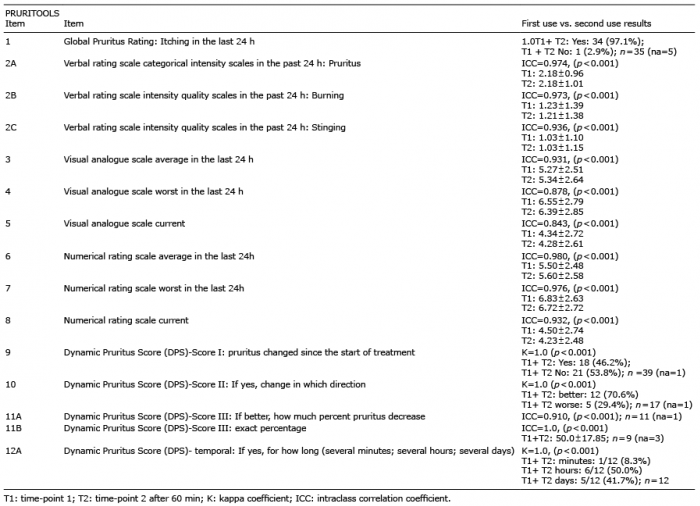 Click to show fullsize
Click to show fullsize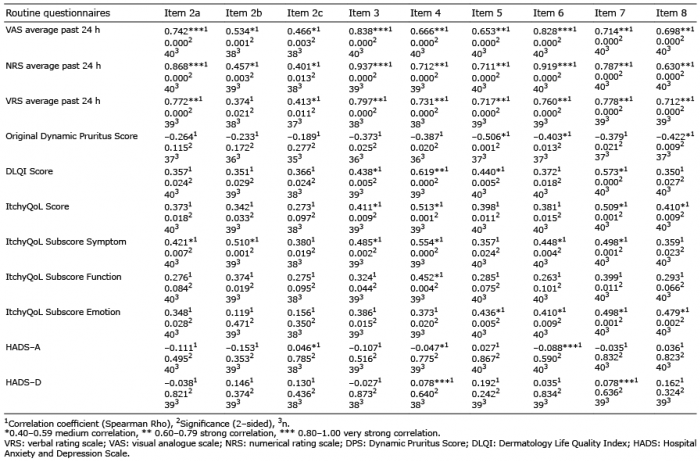 Click to show fullsize
Click to show fullsize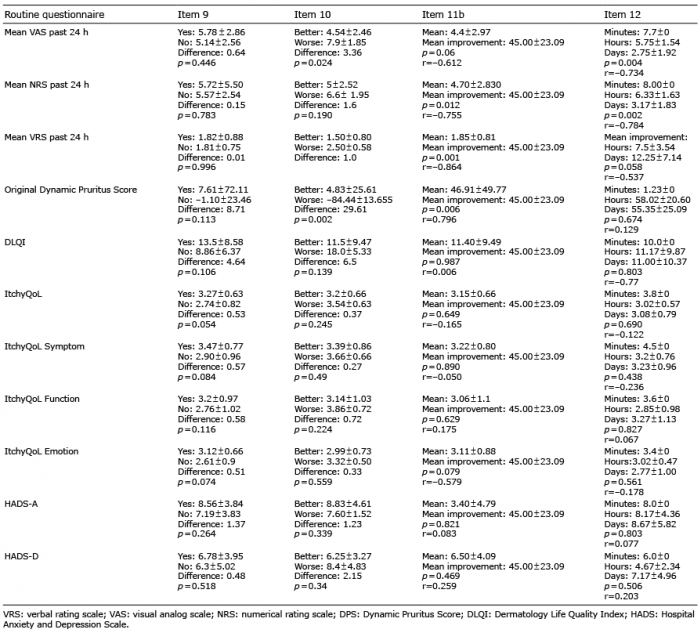 Click to show fullsize
Click to show fullsize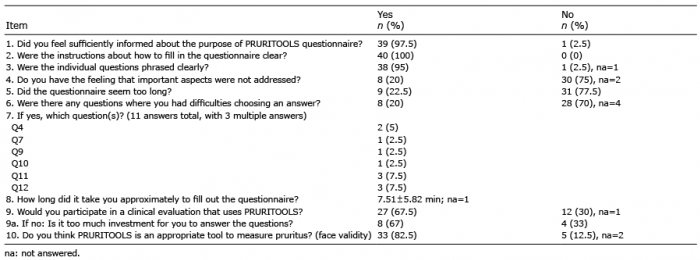 Click to show fullsize
Click to show fullsize