


1Department of Dermatology, Nara Medical University School of Medicine, 840 Shijo, Kashihara, Nara 634-8522, Japan, and 2Department of Dermatology, Osaka City University Graduate School of Medicine, 1-4-3 Asahimachi, Abeno, Osaka 545-8585, Japan. E-mail: fumim@naramed-u.ac.jp
Accepted Apr 2, 2019; E-published Apr 2, 2019
Nivolumab is a fully human monoclonal antibody against the programmed cell death (PD)-1 receptor, an immune checkpoint receptor, which is expressed on activated T cells. PD-1 acts as a negative regulator of the anti-tumour T-cell effector functions when bound to its programmed death ligand 1 (PD-L1) (1). The expression of PD-L1 on tumour cells can help tumours escape from host immune responses, and thus, blocking PD-1/PD-L1 interactions, with therapeutic antibodies, results in the stimulation of antitumor T cells (1, 2).
Treatment with nivolumab or a PD-1 inhibitor can induce immune-related adverse events (irAE), such as lichen planus (LP), as it results of T-cell activation (3). Typically, the lichenoid reactions, caused by nivolumab, demonstrate similar cutaneous manifestations to the well characterized lichenoid drug reactions, caused by a variety of other medications, such as anti-hypertensive and β-adrenergic blockers; i.e., violaceous, flat-topped papules (4). However, the mucous membranes are usually spared (5).
We report an unusual case of a lichenoid drug reaction caused by nivolumab, which was restricted to the oral cavity and anal region. In this case, painful hemorrhagic erosions arose on the lips and oral mucosa, which looked similar to the mucosal lesions seen in Stevens-Johnson syndrome (SJS).
A 75-year-old Japanese man presented with painful oral and anal erosions after 19 cycles of nivolumab treatment. The lesions first appeared after the 13th cycle of therapy. The patient was started on 3 mg/kg nivolumab every 2 weeks for stage IV gastric cancer (T4bN3aM1), which was refractory to multiple lines of chemotherapy, 9 months before his presentation.
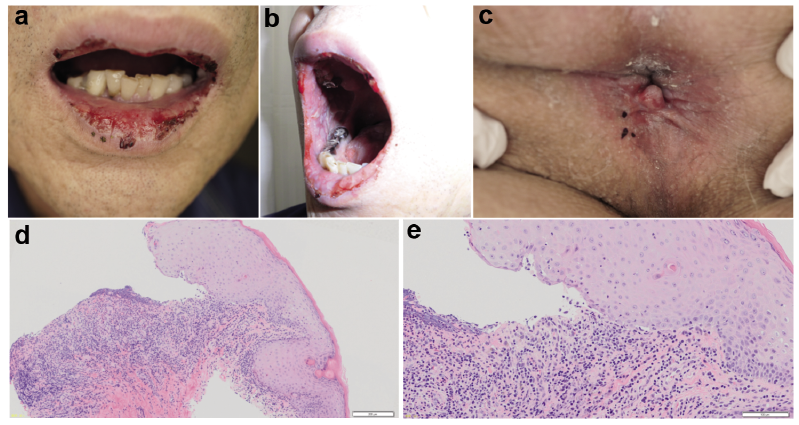
A physical examination showed erosions limited to the mucous membranes; the buccal, gingival and glossal mucosae; the lips (Fig. 1a, b); and the perianal region (Fig. 1c). Massive hemorrhagic erosions covered by crusts were seen on the lip (Fig. 1a, b). The skin was not affected. He had also developed erosions on his glans penis, but they had spontaneously healed a few weeks ago. His medical history included hypertension and alcoholic liver disease.
Fig. 1. (a) Painful hemorrhagic erosions, coated by crusts on the lip. (b) Extensive erosions on the oral mucosae. (c) Perianal erosions. (d) Histopathology of the anal lesions (x40). Lichenoid inflammation and scattered necrotic keratinocytes in the epidermis were detected. (e) Higher magnification of (d) (x100).
Laboratory tests showed the following abnormalities: red blood cells: 368 × 104/µ (normal range: 435–555), hemoglobin: 11.9 g/dl (13.7–16.8), hematocrit: 35.1% (40.7–50.1), C-reactive protein: 2.42 mg/dl (< 0.14), albumin: 3.8 g/dl (4.1–5.1), alkaline phosphatase: 1,221 U/l (106–322), γ-glutamyltranspeptidase: 249 U/l (13–64), and cholinesterase: 182 U/l (240–486). Enzyme-linked immunosorbent assays for anti-desmoglein 1, anti-desmoglein 3, anti-BP180, and anti-BP230 antibodies were all negative. Histopathological examinations of the lesions on the lip and anus showed subepidermal clefts, vacuolization of the basal layer, and the infiltration of band-like inflammatory cells into the dermal–epidermal junction, which was associated with scattered necrotic keratinocytes in the epidermis (Fig. 1d, e). Direct immunofluorescence of the perilesional biopsy samples taken from each lesion produced negative results.
Indirect immunofluorescence of normal human skin and 1M NaCl-salt-split skin produced negative results. Immunoblot analyses using normal human epidermal extracts, the BP180NC16a domain recombinant protein, the BP180 C-terminal domain recombinant protein, a concentrated HaCaT cell culture supernatant, normal human dermal extracts, and purified human laminin-332 all produced negative results.
These findings confirmed the diagnosis of mucosal LP. Nivolumab was discontinued, and treatment with 30 mg/day prednisolone was initiated. The perianal lesion had resolved within two weeks, and the oral lesions gradually improved. Therefore, the prednisolone dose was tapered to 5 mg/day. Three months after the nivolumab treatment had been stopped, a computed tomography scan revealed that the patient’s gastric cancer had progressed; thus, nivolumab was re-administered. After 5 additional cycles, he again developed erosions on his buccal mucosae, lip, and gingivae. Nivolumab was discontinued, and the prednisolone dose was increased to 30 mg/day. The oral lesions resolved, and the dose of prednisolone was gradually decreased. Nivolumab was no longer considered as a treatment option for the patient’s gastric cancer.
PD-1 inhibitors, including nivolumab, represent an effective treatment for various cancers, but they can induce irAE affecting the skin, gastrointestinal tract, liver, endocrine system, and other organ systems (3). In a previous study of 82 patients who received an anti-PD-1 therapy for metastatic melanoma, cutaneous reactions occurred in 30–40% of the patients, with lichenoid reactions (17%), eczema (17%), and vitiligo (15%) being the most common conditions (5). Thus, PD-1 inhibitors can be added to the expanding list of drugs associated with lichenoid eruptions (4).
Previously published studies have demonstrated that mucous membrane-limited LP is very rare in cases of lichenoid drug eruptions. LP can affect the mucosal surfaces of the mouth, vagina, esophagus, conjunctiva, urethra, anus, nose, and larynx, and this condition is called mucosal LP (6). Most cases of mucous membrane-limited, PD-1 inhibitor-induced LP involved typical reticular white lines or plaques (Wickham’s striae) appearing in the oral cavity (3, 7–9). These mucosal lesions were usually managed with topical corticosteroids and did not require the discontinuation of therapy (8, 9). However, several cases with severe oral ulcers have been reported (10–12). Our case represents a rare and extremely severe case of mucous membrane-limited, nivolumab-induced LP, mimicking mucosal lesions in SJS. In the current case, SJS could be excluded because the patient did not develop skin eruptions, fever, or ocular lesions. Our case demonstrated that nivolumab-induced LP affecting the oral mucosa could be as severe as the oral mucosal lesions seen in SJS. In addition, these oral lesions induced pain and bleeding, which severely affected oral intake, resulting in a reduced quality of life and malnutrition, which should not be underestimated.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize