


1Dermatology Unit, Policlinico Tor Vergata, Rome, 2Dermatology Unit, Hospital ‘Bianchi Melacrino Morelli’, Reggio Calabria, 3Department of Dermatology, Papardo Hospital, Messina, 4Dermatologic Clinic of Terni, University of Perugia, Perugia, 5Division of Dermatology, University Hospital Policlinico “S. Orsola-Malpighi”, Bologna, 6Department of Dermatology, University of Modena and Reggio Emilia, Modena, 7Institute of Dermatology, Catholic University of Rome, Fondazione Policlinico Universitario A. Gemelli – IRCCS, Rome, 8Department of Dermatology, University of Pisa, Pisa, 9Department of Medical Sciences and Public Health, Section of Dermatology, University of Cagliari, Cagliari, 10Section of Dermatology and Venereology, Department of Medicine, University of Verona, Verona, 11Department of Dermatology, University of Padua, Padova, 12Istituto Dermopatico dell’Immacolata IDI-IRCCS, Rome, 13Dermatologic Clinic, G. D’Annunzio University, Chieti, 14Dermatology Unit, Sapienza University of Rome, Polo Pontino, Latina, 15UOC of Dermatology, Umberto I Hospital, Università La Sapienza, Rome, 16Dermatology, Department of Biotechnological and Applied Clinical Sciences, University of L’Aquila, L’Aquila, 17Department of Advanced Biomedical Sciences, University of Naples Federico II, Naples, 18Department of Dermatology, University of Bari, Bari, 19Dermatology Unit, Department of Clinical and Molecular Sciences, Polytechnic Marche University, Ancona, 20Department of Clinical Dermatology, San Gallicano Dermatological Institute Istituto di Ricovero e Cura a Carattere Scientifico, Rome, 21Department of Health Sciences, Dermatology Section, University of Florence, Firenze, 22Novartis Farma SpA, Origgio, 23Unit of Dermatology, IRCCS Humanitas Research Hospital, Rozzano, Milan, and 24Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Milan, Italy
This study evaluated whether secukinumab treatment for patients with moderate to severe plaque psoriasis correlates with improvements in symptoms of anxiety and depression. SUPREME was a 24-week, phase IIIb, multicentre, prospective study conducted across 50 centres in Italy with an extension period of up to 72 weeks. Assessments used were: Psoriasis Area Severity Index (PASI), Hospital Anxiety and Depression Scale (HADS) – Anxiety (HADS-A), and HADS – Depression (HADS-D) scores and Dermatology Quality Life Index (DLQI). Compared with baseline, a significantly greater proportion of patients who reported moderate to severe clinical symptoms of anxiety or depression (HADS-A or HADS-D ≥ 11) were free of moderate to severe symptoms at weeks 16 and 48. The PASI and DLQI scores reduced over time with secukinumab treatment. Psoriasis treatment with secukinumab for 48 weeks resulted in significantly improved skin clearance and a parallel improvement in symptoms of anxiety and depression, assessed by HADS.
Key words: anxiety; depression; psoriasis; secukinumab; quality of life.
Accepted Nov 27, 2020; Epub ahead of print Dec 3, 2020
Acta Derm Venereol 2021; 101: adv00422.
doi: 10.2340/00015555-3712
Corr: Antonio Costanzo, Dermatology Unit, Department of Biomedical Sciences, Humanitas University, IRCCS Istituto Clinico Humanitas, Via Alessandro Manzoni 113, IT-20089, Rozzano-Milan, Italy. E-mail: antonio.costanzo@hunimed.eu
Improvements in psoriatic symptoms may improve anxiety and depression symptoms in patients with psoriasis, who also suffer from these psychiatric disorders. We evaluated whether secukinumab treatment, over 48 weeks, might improve anxiety and depression symptoms in patients with moderate to severe plaque psoriasis who participated in the SUPREME clinical trial. Our findings show that 66.7% and 70.6% of patients changed their status from having symptoms of anxiety at baseline to not having anxiety symptoms at Weeks 16 and 48, respectively. Similarly, 81.3% and 70.6% of patients exhibited improvement in symptoms of depression at weeks 16 and 48, respectively.
Psoriasis is a chronic, immune-mediated, inflammatory skin disease (1, 2). Approximately 80–90% of patients with psoriasis develop well-demarcated, red, scaly plaques on the skin (2), typically located on the extensor aspect of the limbs (elbows and knees), scalp, lumbosacral region, and umbilicus (1). Plaques may also appear on the palms, soles, and nails (1, 2). Patients with psoriasis may also experience psychiatric disorders, among other comorbid conditions (3). There is a higher prevalence of psychiatric disorders in patients with psoriasis, compared with the general population and patients with other dermatological conditions (3–5). Patients with painful and disfiguring psoriasis plaques on the visible areas of the body may encounter high levels of stigma, and develop negative self-esteem and issues with body image that may contribute to anxiety or depression (6, 7). In addition to impairment in quality of life (QoL) due to the psoriatic disease, comorbid anxiety or depression may further worsen patients’ QoL. Although the mechanisms through which anxiety and depression may interfere with the clinical course of psoriatic disease are unknown, improvements in the symptoms are expected to reduce patients’ burden of anxiety or depression and improve their QoL.
Secukinumab is a fully human monoclonal antibody that selectively neutralizes interleukin (IL)-17A, a essential cytokine involved in the development of psoriasis. Treatment with secukinumab has shown long-lasting efficacy and a favourable safety profile in various domains of psoriatic disease (8–17).
The aim of this study was to evaluate the effect of treatment of psoriatic disease with secukinumab on concurrent symptoms of anxiety and depression in patients in the SUPREME study (18), in a 49-week evaluation using the Hospital Anxiety and Depression Scale (HADS) (19, 20). Absolute Psoriasis Area and Severity Index (PASI) scores over time according to depression and anxiety status were also analysed. Furthermore, this study reports changes in QoL according to baseline anxiety and depression status.
Study design and patients
The SUPREME study was a 24-week, phase IIIb, multicentre, prospective study conducted across 50 centres in Italy, with an extension period of up to 72 weeks (18, 21). The aim of the SUPREME study was to explore the efficacy and safety profile of secukinumab 300 mg in patients with moderate to severe chronic plaque-type psoriasis, stratified by human leukocyte antigen (HLA)-Cw6 status. The detailed study design and patient characteristics have been previously reported (18).
The current study is a post hoc analysis of data from patients enrolled in the SUPREME study who were observed for at least 48 weeks. Inclusion criteria were: patients aged ≥ 18 years diagnosed with moderate to severe chronic plaque-type psoriasis of ≥ 6 months’ duration. Moderate to severe plaque-type psoriasis was defined at enrolment by PASI score ≥ 10 or PASI score > 5 and < 10, and Dermatology Life Quality Index (DLQI) ≥ 10. The study also included patients with concomitant nail, scalp, or psoriatic arthritis (PsA) according to the Classification Criteria for Psoriatic Arthritis (CASPAR). All patients provided written informed consent before enrolment in the SUPREME study. The study protocol was approved by the institutional review board of each participating centre. The trial was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice, and in compliance with all federal, local and regional requirements.
Assessments
The severity of psoriasis was measured using PASI weekly until week 16 and then at weeks 20, 24, 36 and 48 (22).
The Hospital Anxiety and Depression Scale (HADS) was used to assess anxiety and depression in the SUPREME study population. The HADS is a patient-reported anxiety (HADS-A) and depression (HADS-D) assessment comprising 7 questions for each subscale (anxiety or depression), with responses for each item ranging from scores of 0 to 3 (total 0–21) and higher scores indicating more severe symptoms. A cut-off of HADS score ≥11 was used to identify patients with moderate to severe clinical signs of anxiety and depression (19, 20).
The DLQI questionnaire was used to assess QoL of patients enrolled in the SUPREME study.
Population analysis
A 1-year observation set included all treated patients with at least one year of observation and a valid HADS assessment at week 48. The following 2 cohorts were defined starting from the 1-year observation set: (i) anxiety cohort: all 1-year observation patients with a baseline HADS-A score ≥ 11; (ii) depression cohort: all 1-year observation patients with a baseline HADS-D score ≥ 11.
Statistical analysis
The study population included patients with visits up to week 48, and with baseline and week 48 HADS measurements. Data are presented as n (%) or mean ± standard deviation (SD) and 95% confidence interval (95% CI), as appropriate. A nominal p-value < 0.05 was considered statistically significant.
Demographic and baseline characteristics of patients, including previous treatments, were summarized and presented by depression and anxiety status. Significance tests for baseline differences between patients with and without depression or anxiety, included t-test or Wilcoxon test or χ2 test or Fisher’s exact test, as appropriate.
For identifying determinants of anxiety or depression, univariate logistic regression analysis, and multivariate logistics analysis with stepwise selection were performed. Beta estimate for continuous variables and odds ratios with 95% CI were reported. Baseline variables included in the regression model were: age, time since first diagnosis of psoriasis, weight, body mass index, waist circumference, body surface area, nail psoriasis (present vs absent), scalp psoriasis (present vs absent), PASI score, smoking status (current vs never; former vs never), presence of PsA (yes vs no), anxiety or depressive status (HADS-A/D ≥ 11 vs < 11). The following variables were also included in the regression model: DLQI, HLA-Cw6 status (positive vs negative), number of comorbidities, and number of prior treatments for psoriasis.
PASI score over time was plotted for patients with and without anxiety or depression, and the Wilcoxon test was used to assess a significant difference between time-points. At weeks 16, 24, 36, and 48, the proportion of patients with PASI 90/75 was evaluated by anxiety and depression cohorts; the χ2 test assessed a significant difference between cohorts.
The correlation between HADS and DLQI total score at each time-point was explored using the Spearman’s coefficient according to the non-normal distribution of data. In addition, changes in DLQI total score by baseline anxiety or depression were analysed at baseline, weeks 16, 24, and 48, and significance was tested using the Wilcoxon test. Absolute changes in values were considered.
Patient demographics and disease characteristics
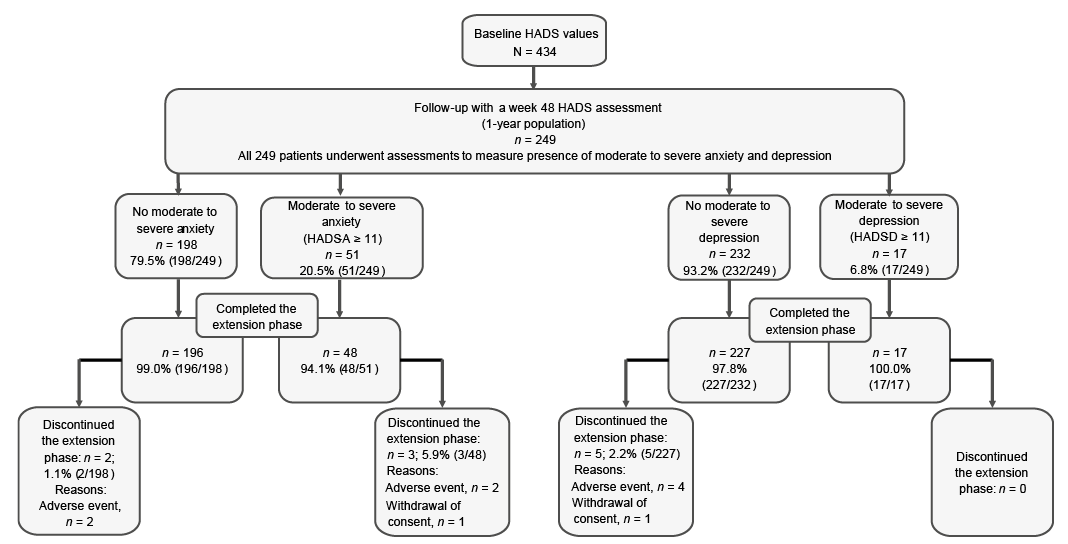
A total of 434 patients were enrolled in the SUPREME study with baseline HADS measurements. Of these, 249 patients had a valid HADS assessment up to 48 weeks. At baseline, 20.5% (51/249) and 6.8% (17/249) of patients had HADS-A or HADS-D scores of ≥11, respectively. Details of patient disposition are shown in Fig. 1.
Fig. 1. Patient disposition by study cohort (1-year population). HADS-A/D: Hospital Anxiety and Depression Scale – Anxiety/Depression subscale; N: total number of patients; n: number of patients.
Baseline demographics and disease characteristics, by depression and anxiety status, are shown in Table I.
Table I. Baseline demographics and disease characteristics by anxiety and depression status (1-year population)
In the anxiety status cohort, all patients with moderate to severe anxiety at baseline were aged < 65 years, were predominantly female, had significantly earlier time since PsA diagnosis, and had a slightly higher presence of concomitant PsA, compared with patients with no moderate to severe anxiety. In the depression status cohort, patients with moderate to severe depression at baseline had a significantly higher waist circumference compared with patients with no moderate to severe depression. No significant difference was observed in the type of prior psoriasis treatment received by the patients by baseline anxiety or depression status. Likewise, no significant difference was found in the smoking history of patients by their baseline anxiety or depression status. There was no significant difference in psoriasis disease severity, as measured by PASI and Investigator’s Global Assessment modified version 2011 (IGA mod 2011) scores, according to patients’ baseline anxiety or depression status.
Determinants of anxiety and depression status at baseline
Considering the univariate model for determinants of anxiety, the following covariates were found to be statistically significant: presence or absence of moderate to severe depression at baseline (i.e. HADS-D ≥ 11), DLQI at baseline, and number of comorbidities (Table II). The stepwise approach in the multivariate regression model confirmed DLQI (i.e. patients with a greater score have a greater probability of also having a HADS-A ≥ 11) and depression (i.e. patients with HADS-D ≥ 11 have a greater probability of having anxiety) as significant determinants of anxiety. Furthermore, HLA-Cw6-positive patients have a statistically significant greater probability of having anxiety. Similarly, anxiety status, DLQI at baseline, and waist circumference were significant covariates in the univariate model for determinants of depression (Table II). Further stepwise analysis in a multivariate logistic regression model confirmed DLQI and anxiety status at baseline as significant determinants of depression in patients with psoriasis.
Table II. Determinants of anxiety and depression status
Efficacy
A marked reduction in PASI score was observed with secukinumab treatment in all patients irrespective of their baseline anxiety or depression status. Absolute PASI (mean ± SD) scores in patients without moderate to severe anxiety at baseline (HADS-A<11; n = 198) vs patients with moderate to severe anxiety at baseline (HADS-A ≥ 11; n = 51) were 0.73 ± 1.58 vs 0.90 ± 1.40 (p = 0.07) at week 16, and 0.74 ± 2.15 vs 1.30 ± 2.61 (p = 0.05) at week 48 (Fig. 2a). Similar trends were observed in patients without moderate to severe depression at baseline (HADS-D < 11; n = 232) vs patients with moderate to severe depression at baseline (HADS-D ≥ 11; n = 17); a mean absolute PASI score of 0.77 ± 1.58 vs 0.65 ± 0.75 (p = 0.17) at week 16, and 0.88 ± 2.33 vs 0.53 ± 0.83 (p = 0.35) at week 48 (Fig. 2b).
Fig. 2. Psoriasis Area and Severity Index (PASI) score over time: mean score by (a) anxiety and (b) depression status (1-year population). HADS-A/D: Hospital Anxiety and Depression Scale – Anxiety/Depression subscale.
A significantly higher proportion of patients with moderate to severe anxiety at baseline reported a decrease in HADS-A scores to < 11 at week 16 (66.7%; p < 0.001) and at week 48 (70.6%, p < 0.001; Fig. 3a). Instead, a very small proportion of patients who did not show moderate to severe anxiety at baseline demonstrated an increase in HADS-A scores to 11 or more at weeks 16 (2.2%) and 48 (3.0%). Similarly, a significantly higher proportion of patients with moderate to severe depression at baseline showed HADS-D scores of less than 11 at weeks 16 (81.3%; p < 0.001) and 48 (70.6%; p = 0.06, Fig. 3b). In a very small proportion of patients without moderate to severe depression at baseline, the HADS-D score increased to ≥ 11 at weeks 16 (0.5%) and 48 (3.0%).
Fig. 3. Prevalence of (a) anxiety and (b) depression: baseline vs follow-up visits. *p < 0.001 and p < 0.001 vs baseline. HADS-A/D: Hospital Anxiety and Depression Scale – Anxiety/Depression subscale. HADS-A or D ≥ 11: no moderate to severe anxiety or depression; HADS-A or D < 11: moderate to severe anxiety or depression.
At week 16, in cohorts without and with moderate to severe anxiety (at baseline), 86.9% and 80.4% of patients achieved PASI 90 scores, and 98.0% and 92.2% of patients achieved PASI 75. Similarly, a consistently higher proportion (≥ 75%) of patients in cohorts both with and without anxiety achieved PASI 90 and 75 scores at weeks 24, 36, and 48 (Table III). At all time-points, patients without moderate to severe anxiety at baseline showed significantly higher PASI 90 responses than patients with moderate to severe anxiety at baseline. In addition, except at week 48, a similar trend was observed for PASI 75 responses between patients with and without moderate to severe anxiety at baseline. In comparison with baseline depression status, at week 16, 85.8% and 82.4% of patients achieved PASI 90 scores, and 96.6% and 100.0% of patients achieved PASI 75 scores in the without and with depression groups, respectively. A similar proportion of patients in comparison with baseline depression status achieved PASI 90 scores at weeks 24, 36, and 48; likewise, ≥ 95% patients without depression (at baseline) and 100% of patients with depression (at baseline) achieved PASI 75 scores at the same time-points (Table III). At almost all time-points, there was no statistical difference between patients with and without moderate to severe depression at baseline in achieving PASI 75 and PASI 90 responses.
Table III. Psoriasis Area and Severity Index (PASI) 90 and 75 scores over time by baseline anxiety and depression status
Correlation between HADS and DLQI scores
Spearman’s correlation coefficients highlight a significant positive correlation at baseline between HADS-A score and DLQI score and HADS-D and DLQI score; 0.4080 and 0.4433, respectively. At baseline, patients with moderate to severe anxiety or depression had significantly higher total DLQI scores compared with patients without anxiety or depression, respectively. At weeks 16, 24, and 48 total DLQI scores in patients with anxiety and depression decreased compared with baseline values, but remained higher than DLQI total score observed in patients without moderate to severe anxiety or depression (Fig. 4). At weeks 16, 24, and 48, > 75% of patients with no moderate to severe anxiety or depression at baseline achieved a DLQI score of 0 or 1. Similarly, up to 60% of patients with anxiety and depression at baseline achieved a DLQI score of 0 or 1 as soon as week 16, and retained this response through weeks 24 and 48 (Fig. 5).
Fig. 4. Relationship between anxiety and depression status by baseline and Dermatology Life Quality Index (DLQI) scores: (a) DLQI score by anxiety status over time; (b) DLQI score by depression status over time.
Fig. 5. Proportion of patients with Dermatology Life Quality Index (DLQI) score of 0 or 1 by anxiety or depression status. (a) DLQI 0/1 by anxiety status overtime; (b) DLQI 0/1 by depression status over time.
Psychological outcomes have garnered prominence in chronic diseases research and, as a result, studies have investigated psychological well-being in chronic conditions, such as cancer, (23) diabetes, (24) chronic heart failure, (25) and chronic pain (26). The presence of anxiety and depression has been established in patients with psoriasis, (3, 4, 27) and studies (28–31) have investigated the effect of treatment for psoriatic disease on improving symptoms of anxiety and depression. Baseline HADS data in the present analysis confirms the presence of anxiety (51/249; 20.5%) and depression (17/249; 6.8%) in patients with psoriasis. Patients’ characteristics in the present analysis were similar to those of patients in previous studies investigating anxiety and depression in psoriasis (28, 32–36).
In the current study, secukinumab treatment was found to be associated with a significant improvement in skin clearance and amelioration of symptoms of anxiety and depression in most patients with psoriatic disease, regardless of HADS baseline score, suggesting that psychological impairments may improve in parallel with improvements in psoriatic disease.
This study analysed, over a 48-week period, the proportion of patients in whom symptoms of moderate to severe anxiety or depression were ameliorated by secukinumab treatment, as measured by HADS thresholds. At weeks 16 and 48, a significantly greater proportion of patients changed status from having symptoms of anxiety or depression (HADS-A or HADS-D ≥ 11) at baseline to not having symptoms of anxiety (66.7% and 70.6%) or depression (81.3% and 70.6%).
In the current analysis, the presence of baseline depression or anxiety, a higher DLQI score at baseline, HLA-Cw6 positive status, and higher waist circumference were estimated as determinants of anxiety or depression status at baseline. A study of 133 patients with psoriasis revealed that female sex and higher PASI score were associated with increased risk of anxiety, while female sex, higher PASI score and longer disease duration were correlated with increased risk of depression (35). A study of 193 patients from Poland demonstrated that the effect of psoriasis on social anxiety was moderated by age of onset, whereas negative body-related emotions mediated the relationship between the severity of disease and depression (6). Furthermore, a study of 300 patients from Spain concluded that patients with moderate to severe psoriasis associate with a higher risk of depression and anxiety symptoms (37). Another study, of 441 patients with psoriasis, found that the rate of depression and anxiety is significantly higher in patients with PsA than those without PsA (38). Genetic association and linkage studies demonstrated a strong association between HLA-Cw6 alleles and psoriasis susceptibility (39–41). HLA-Cw6-positive status increases the risk of psoriasis 10 times and is also associated with early-onset psoriasis and more severe disease (39, 42). However, the relationship between HLA-Cw6-positive status and psychological symptoms in patients with psoriasis has not been documented. In the current analysis, HLA-Cw6-positive status at baseline was a statistically significant determinant of anxiety. Speculatively, this latter data could be explained by evidence that there is a higher risk of developing psoriasis in HLA-Cw6-positive patients exposed to stressful life events or to other conditions known to be associated with psychological distress, such as cigarette smoking or obesity (39, 43). The current study did not analyse the correlation between HLA-Cw6 status and secukinumab treatment effect on anxiety and depression symptoms in patients with psoriasis.
Baseline DLQI scores revealed that patients with psoriasis who have depression or anxiety have a significant negative impact on QoL compared with patients with psoriasis and without symptoms of anxiety and depression. Furthermore, Spearman’s correlation analysis revealed a notable association between anxiety or depression and DLQI scores. Treatment with secukinumab over 48 weeks resulted in improvement in QoL (decreased DLQI scores) in patients both with and without depression or anxiety at baseline. Interestingly, in the current study, patients with no moderate to severe anxiety or depression at baseline showed significantly higher PASI 90 and 75 responses than did patients with moderate to severe baseline anxiety at all time-points until week 48. However, the difference in PASI 90 and 75 responses was not significant in patients with or without moderate to severe depression at baseline. In addition, QoL outcomes, as measured by DLQI, were significantly improved in patients with no moderate to severe anxiety or depression at baseline than those with moderate to severe anxiety or depression. The reasons for observed differences in PASI 90 and DLQI outcomes should be explored in future studies.
Across the secukinumab clinical trial programme, no safety concerns were observed for depression, anxiety, or suicide (44–46). In a pooled analysis of data from 10 clinical studies, incidence of depressive disorders, anxiety or suicidal ideation and behaviour was less than 2 per 100 patient years of exposure in the secukinumab group. The study concluded that there is no elevated risk of depression, anxiety or suicidality with secukinumab (44). To our knowledge, the current study is the first evidence in an Italian cohort that demonstrates the ability of secukinumab to also improve symptoms of anxiety and depression in patients with moderate to severe plaque psoriasis.
Three phase III studies of brodalumab (IL-17 receptor antagonist) were terminated in May 2015; according to a news release from the pharmaceutical company Amgen, “this decision was based on events of suicidal ideation and behaviour in the brodalumab program” (47, 48). The US prescribing information (49) and the European Medicine Agency (EMA) assessment report (50) outlines the potential risk of suicidal behaviour with the brodalumab therapy. However, such risks are not listed for IL-17A inhibitors, such as ixekizumab and secukinumab; nevertheless, it is important to assess the effect of psoriasis therapies on psychiatric symptoms.
The results of this study should be interpreted considering the number of patients having symptoms of anxiety or depression (HADS-A ≥ 11, n = 48, and HADS-D ≥ 11 n = 17) in the anxiety and depression assessment cohorts. Furthermore, it is noteworthy to account the post hoc nature of the analysis and the limitations of the scale to measure anxiety or depression. The HADS has been used to measure the prevalence of anxiety and depression in moderate to severe plaque psoriasis, but some studies have proposed that HADS is ideal for screening rather than measurement of severity of anxiety and depression over time (28). In addition, the clinical usefulness of HADS threshold to define essential improvement in symptoms of anxiety or depression has yet to be conclusively demonstrated (28).
In conclusion, in patients with moderate to severe plaque psoriasis, over a period of 48 weeks, secukinumab treatment improved skin clearance, with 80–87% patients achieving a PASI 90 response irrespective of baseline anxiety and depression status, and, in parallel, symptoms of anxiety and depression improved, as measured by HADS. However, it remains to be investigated whether skin clearance alone leads to this phenomenon, or whether specific IL-17A targeting plays an additional role. Anxiety and depression are critical psychiatric comorbidities in patients with moderate to severe psoriasis that affects patients’ quality of life, and therefore dermatologists and other healthcare providers must be aware of the effect of psoriasis therapies on these psychiatric disorders. Future mechanistic studies may elucidate the relationship between inhibition of IL-17A with secukinumab and its impact on the physiopathology of anxiety and depression in patients with psoriasis.
The authors thank Avinash Thakur and Sumeet Sood (Novartis Healthcare Pvt. Ltd, Hyderabad) for editorial and medical writing support, which was funded by Novartis Farma S.p.A., Italy, in accordance with the Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Funding for this study was provided by Novartis Pharma AG, Basel, Switzerland. Novartis Pharma AG contributed to the study design, data collection, data analysis, data interpretation, manuscript preparation and the decision to submit the paper for publication. An advisory committee was involved in the study design and data interpretation, together with authors from Novartis Pharma AG.
Conflicts of interest: AC served as advisory board member and consultant, and has received fees and speaker’s honoraria or has participated in clinical trials for AbbVie, Biogen, Fresenius Kabi, Leo Pharma, Lilly, Janssen, Novartis, Sanofi Genzyme and UCB Pharma. GP has been speaker and consultant for Novartis and AbbVie. PA received honoraria for speaker from AbbVie, Janssen, Eli Lilly, Novartis, Pfizer, Celgene and Sanofi. MCF has served as a speaker, board member and/or received research grants from Abbvie, Leo Pharma, Celgene, UCB, Eli Lilly, Pfizer, Janssen, Novartis, Sanofi-Genzyme. AC has been an advisory board member and consultant, and has received fees and honoraria or has participated in clinical trials for AbbVie, Biogen, Leo Pharma, Eli Lilly, Novartis, UCB-Pharma, Sandoz, and Janssen Cilag. PG has been a consultant and/or speaker for AbbVie, Almirall, Celgene, Janssen, Leo-pharma, Eli Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Sandoz, and UCB. AO acted as a speaker and consultant for AbbVie, Eli Lilly, Novartis, Celgene, Sanofi, Galderma, Leo Pharma, Pierre Fabre, outside of the present work. FP reports personal fees for advisory board from AbbVie, Biogen, Eli Lilly, Celgene, Leo Pharma, Novartis, Sanofi and Janssen-Cilag, outside of the present work. SP has consulted (includes advisory boards and podium presentations) for AbbVie, Almirall, Celgene, Galderma, Janssen-Cilag, Leo Pharma, Lilly, MSD, Novartis and UCB Pharma. MT, GM, YN, FB, CM, FC, CP, AB, CB and FL report no conflict of interest. AC acted as a speaker and consultant for AbbVie, Eli Lilly, Novartis, Almirall, Celgene, Sanofi, Janssen and Pfizer. MB, AR, EA and RO are employed by Novartis.
SUPREME Study Group: Luca Bianchi, Valeria Brazzelli, Cinzia Buligan, Martina Burlando, Giacomo Caldarola, Anna Campanati, Angelo Cattaneo, Francesco Cusano, Paolo Dapavo, Stefano Dastoli, Clara De Simone, Micol Del Giglio, Vito Di Lernia, Sergio Di Nuzzo, Daniele Dusi, Rosaria Fidanza, Maria Laura Flori, Chiara Franchi, Marco Galluzzo, Alberto Ghilardi, Giampiero Girolomoni, Federica Giuliani, Dario Graceffa, Katharina Hansel, Piergiorgio Malagoli, Valentina Mastrandrea, Matteo Megna, Santo Raffaele Mercuri, Maria Letizia Musumeci, Luigi Naldi, Alessandra Narcisi, Diego Orsini, Manuela Papini, Annalisa Patrizi, Monica Pau, Giovanni Pellacani, Ketty Peris, Severino Persechino, Leonardo Pescitelli, Lucia Pietroleonardo, Alberto Reseghetti, Marco Romanelli, Franco Rongioletti, Filomena Russo, Roberta Scuderi, Riccardo Sirna, Nevena Skroza, Giuseppe Stinco, Luca Stingeni, Sara Trevisini, Marina Venturini, Cristina Zane, Leonardo Zichichi, Antonio Zini.


 Click to show fullsize
Click to show fullsize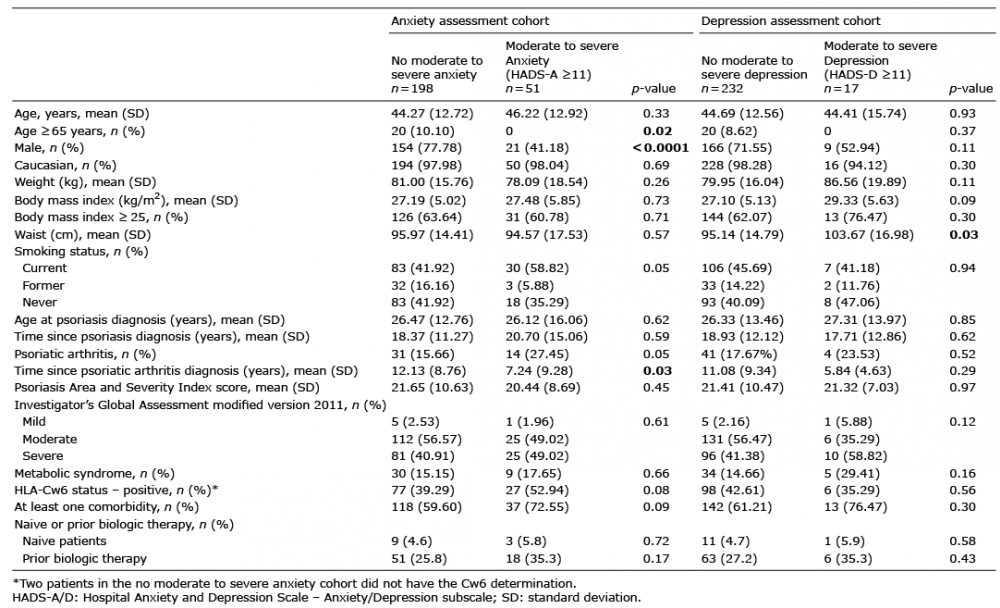 Click to show fullsize
Click to show fullsize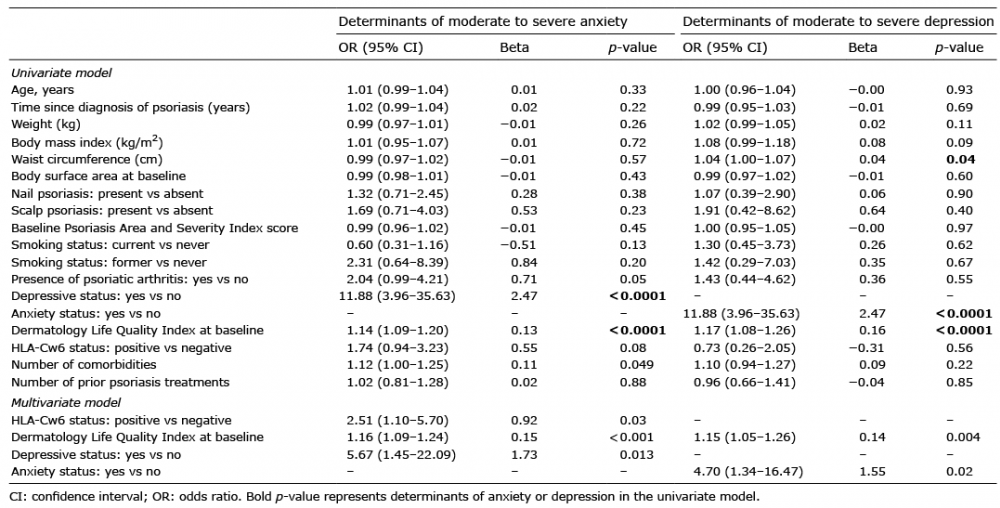 Click to show fullsize
Click to show fullsize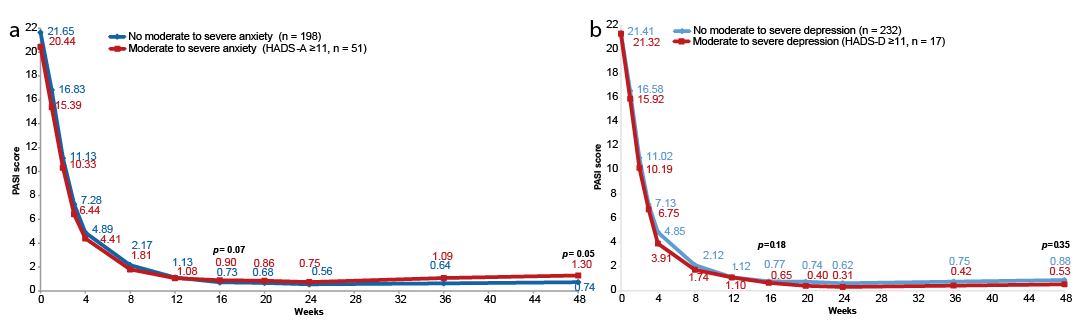 Click to show fullsize
Click to show fullsize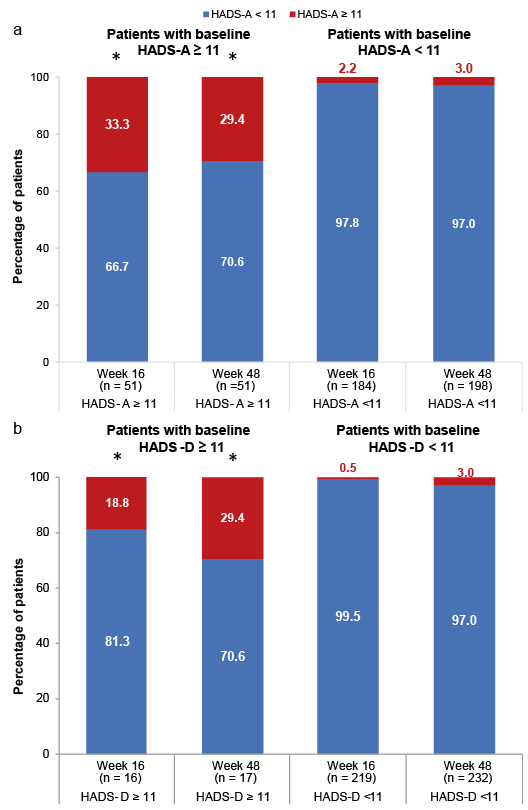 Click to show fullsize
Click to show fullsize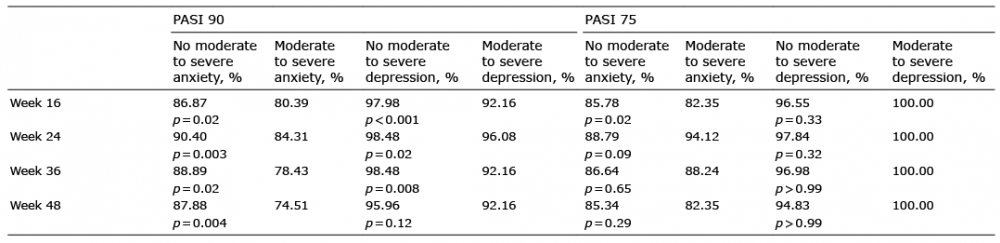 Click to show fullsize
Click to show fullsize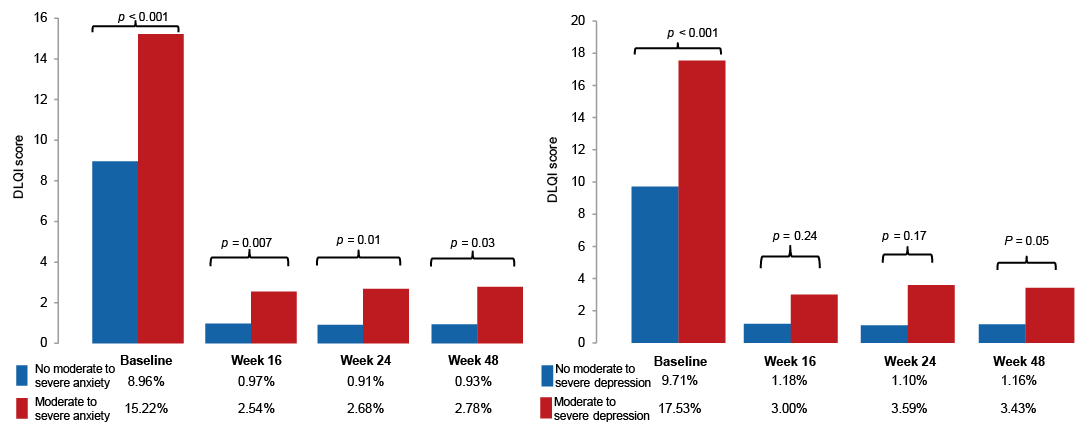 Click to show fullsize
Click to show fullsize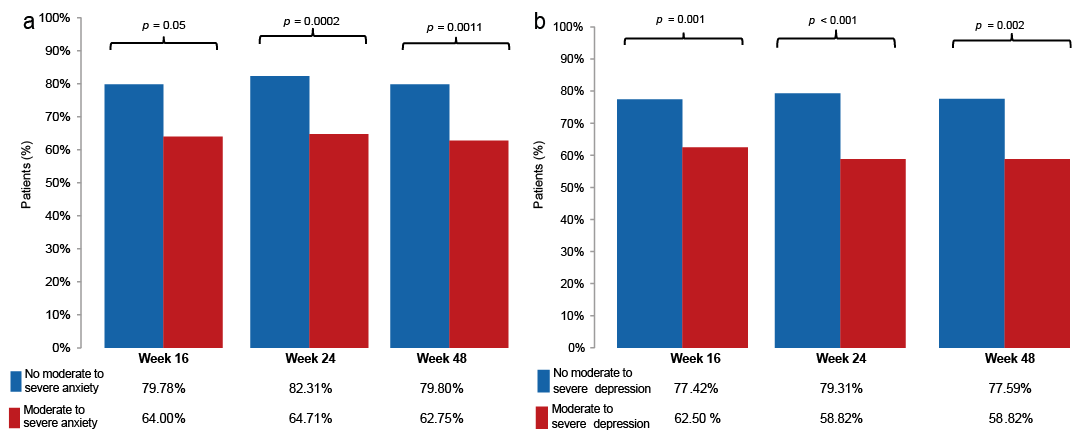 Click to show fullsize
Click to show fullsize