
From the 1Basalt Rehabilitation Centre, The Hague and Leiden, Department of Innovation, Quality + Research, 2Leiden University Medical Center, Department of Biomedical Data Sciences, Leiden, 3The Hague University for Applied Sciences, Faculty of Health, Nutrition and Sports, The Hague, 4Leiden University Medical Center, Department of Orthopaedics, Rehabilitation and Physical Therapy, Leiden, 5Merem Medical Rehabilitation, Hilversum and 6Flevo Hospital, Department of Rehabilitation, Almere, The Netherlands
Objective: To compare the effect on disability and quality of life, of conventional rehabilitation (control group) with individualized, tailored eRehabilitation intervention alongside conventional rehabilitation (Fast@home; intervention group), for people with stroke.
Methods: Pre–post design. The intervention comprised cognitive (Braingymmer®) and physical (Telerevalidatie®/Physitrack®) exercises, activity-tracking (Activ8®) and psycho-education. Assessments were made at admission (T0) and after 3 (T3) and 6 months (T6). The primary outcome concerned disability (Stroke Impact Scale; SIS). Secondary outcomes were: health-related quality of life, fatigue, self-management, participation and physical activity. Changes in scores between T0–T3, T3–T6, and T0–T6 were compared by analysis of variance and linear mixed models. Results: The study included 153 and 165 people with stroke in the control and intervention groups, respectively. In the intervention group, 82 (50%) people received the intervention, of whom 54 (66%) used it. Between T3 and T6, the change in scores for the SIS subscales Communication (control group/intervention group –1.7/–0.3) and Physical strength (–5.7/3.3) were significantly greater in the total intervention group (all mean differences< minimally clinically important differences). No significant differences were found for other SIS subscales or secondary outcomes, or between T0–T3 and T0–T6. Conclusion: eRehabilitation alongside conventional stroke rehabilitation had a small positive effect on communication and physical strength on the longer term, compared to conventional rehabilitation only.
Key words: eHealth; stroke; rehabilitation; comprehensive healthcare; patient-reported outcome measures; telerehabilitation; Stroke Impact Scale; eRehabilitation.
Accepted Dec 16, 2020; Epub ahead of print Dec 28, 2020
J Rehabil Med 2021; 53: jrm000161
Correspondence address: Berber Brouns, Basalt Rehabilitation Centre, The Hague and Leiden, Department of Innovation, Quality + Research, Leiden, The Netherlands. E-mail: b.brouns@lumc.nl, b.brouns@basaltrevalidatie.nl
Doi: 10.2340/16501977-2785
Digital eRehabilitation, including cognitive/physical exercises, activity-tracking and psycho-education, is available for rehabilitation after stroke. In daily practice, these are used in parallel, and evidence regarding the effect of combining applications is scarce. The aim of this study was to investigate the effect of eRehabilitation in clinical practice. Outcomes for 153 people with stroke admitted to conventional rehabilitation only (control group) were compared with the outcomes for 165 people with stroke admitted when eRehabilitation was available (intervention group). A total of 82 people in the intervention group (50%) received the intervention, of whom 54 (66%) used it. In the first 3 months of rehabilitation, no differences were found between the groups. Between 3 and 6 months, the intervention group as a whole showed greater improvements regarding communication and physical strength. However, differences were below minimal clinical importance. In conclusion, adding eRehabilitation alongside conventional stroke rehabilitation had a small positive effect on communication and physical strength on the longer term, compared to conventional rehabilitation only.
W
orldwide, approximately 9 million people have a stroke each year, in many cases leading to a broad range of long-term disabilities with a major impact on multiple areas of life (1). More than half of people with stroke still have physical, mental and/or cognitive impairments 6 months post-stroke (2, 3). In order to enhance recovery of functioning, people with stroke may be referred to inpatient or outpatient specialized rehabilitation facilities offering multidisciplinary treatment (4). In the Netherlands, approximately 10% of people with stroke are admitted to such facilities, mostly those with severe disability and the potential for recovery (5).
During the last decade there has been increasing interest in the use of digital technologies to deliver rehabilitation, termed eRehabilitation, in specialized rehabilitation facilities. Examples of eRehabilitation applications relevant for stroke rehabilitation are: virtual reality (6), online communication and consultation (7, 8), and applications for the delivery of specific physical or cognitive exercises (9). A number of systematic reviews on eRehabilitation in stroke, published in the past 10 years, have assessed their effectiveness within the first 6 months after stroke, and concluded that these applications may result in increased access to care (9) and time spent on therapy-related activities (6). Moreover, improved healthcare outcomes, such as in walking speed, balance and mobility (6), cognition and mood (8), and health-related quality of life (HRQoL) (7), were found.
To date, most studies on eRehabilitation in stroke have focused on interventions targeting a single domain of rehabilitation treatment (9). In daily practice, however, people with stroke face multiple and distinct problems. Therefore, different applications may be useful at the same time. However, making an appropriate selection and handling different means of access are only a few of the many challenges people with stroke and healthcare professionals face in the use of eRehabilitation. Integrating a selection of various eRehabilitation applications within a single combined intervention would greatly increase their user-friendliness, especially if the selection appropriately addresses the needs of the individual patient (10).
Evidence on the effectiveness of such comprehensive eRehabilitation interventions, combining eRehabilitation applications covering more than one domain of early rehabilitation treatment is scarce. Three controlled clinical trials have studied multiple applications combined in a single intervention, i.e. online exercise programmes with activity tracking or stroke-related education (11–13). All 3 studies compared a comprehensive eRehabilitation intervention with conventional rehabilitation, showing equal effect with respect to improvement in motor function and knowledge about stroke (11–13). However, none of these studies included people with stroke admitted to a specialized rehabilitation facility (14), nor did they explore the effects of eRehabilitation when integrated with conventional rehabilitation service delivery. The latter is striking, as it is suggested that eRehabilitation should preferably be offered alongside conventional stroke rehabilitation in order to achieve its full potential (15).
The aim of the current study was to compare the effect on disability and HRQoL of a comprehensive eRehabilitation intervention, Fit After STroke @home (Fast@home), consisting of different components offered in addition to conventional stroke rehabilitation in a specialized rehabilitation facility.
Design and setting
This pre-post test, controlled, pragmatic clinical trial was conducted at 2 rehabilitation centres; in Basalt The Hague, and Leiden, the Netherlands. Two groups were compared; the control group (CG; May 2016–April 2017) receiving only conventional stroke rehabilitation and the intervention group (IG; May 2017–April 2018) receiving Fast@Home alongside conventional rehabilitation. Data were gathered in an ongoing, observational study, Stroke Cohort Outcomes of REhabilitation (SCORE; Dutch Trial Register no. 4293). Assessments were performed at admission (T0), and 3 (T3) and 6 months (T6) after admission. The assessors were not blinded.
The SCORE study was approved by the Medical Ethics Review Committee (protocol NL46531.058.13) of Leiden University Medical Center. All participants gave written informed consent. Details and results of SCORE are published elsewhere (16–19). Reporting of the current study was done according to the STROBE Checklist (20), the description of the intervention was performed according to the TIDieR Checklist (21).
Participants
Inclusion criteria were: age over 18 years and first ever/recurrent stroke less than 6 months ago. Exclusion criteria were: severe psychiatric conditions; unable to communicate in Dutch; concurrent acquired brain injury; and/or drug or alcohol abuse. At admission, the treating rehabilitation physician checked the criteria. Eligible people with stroke were informed by the research team within 2 weeks. All people included in the SCORE study between May 2016 and April 2018 were considered eligible for the current analysis on the effect of eRehabilitation. From May 2017, the intervention was implemented in conventional rehabilitation. In rare cases, Fast@Home had already started before inclusion in the study was accomplished. People were excluded if they used the intervention 7 or more days before T0.
Conventional rehabilitation
During the control and intervention periods, people with stroke received conventional rehabilitation according to a national guideline (22). Treatment was provided by a multidisciplinary team, which included a rehabilitation physician (RP), physical therapist (PT), occupational therapist (OT), speech therapist, psychologist and social worker. Rehabilitation treatment could focus on improving motor, cognitive/psychological function, speech, or participation. Inpatient or outpatient rehabilitation was provided, conditional on the severity of the individual’s impairments and living situation (23).
eRehabilitation intervention
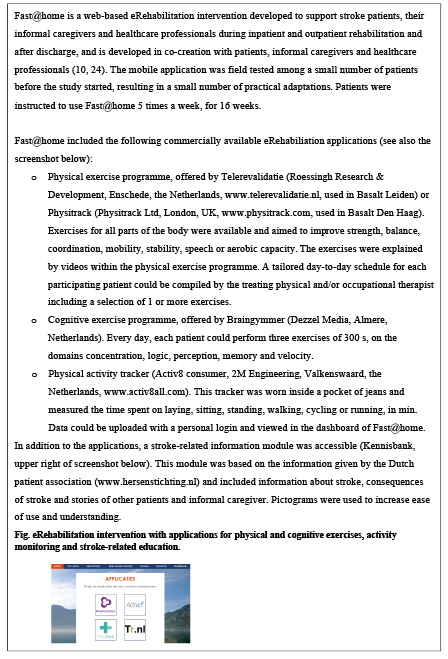
During the intervention period, all people with stroke had free access to the intervention Fast@home (Fig. 1), which comprised several commercially available applications for cognitive and physical exercises, activity-tracking and stroke-related psycho-education. The intervention was accessible on a smartphone, laptop/PC or tablet. Some applications could be used with, and some without, the support, or interaction with, a healthcare professional.
Fig. 1. The Fast@home intervention.
A tailored strategy, based on barriers and facilitators identified in preceding studies (10, 24) was used to implement the intervention. Implementation included, among others, structured integration in the healthcare process, providing education and information to healthcare professionals, people with stroke and their caregivers, and providing a helpdesk/support for all users. Implementation activities were mostly executed as planned and supplemented with instructional activities. Of the 49 healthcare professionals who were invited for the instructional session (RPs, OTs and PTs only), 47 (95.9%) attended. Of those professionals trained to deliver the intervention, 75.8% actually delivered it. The main areas for improvement in the implementation of eRehabilitation are found to be related to healthcare professionals’ perceptions of the intervention, integration of eRehabilitation into conventional rehabilitation, and technical and organizational contextual factors. More information about the implementation strategy, including fidelity and adaptations and details about the training provided for the healthcare professionals, is published elsewhere.
The intervention was delivered as follows:
1. All people with stroke were registered as users of Fast@Home by the research team. Log-in credentials for people with stroke were recorded in the electronic patient record, and forwarded to the patient by email.
Every registered patient had access to the psycho-education module.
Delivery of applications for cognitive exercises, physical exercises and/or the activity tracker was tailored to the individual’s needs and goals. For the selected applications, treating therapists compiled an individualized programme.
2. People with stroke could access the eRehabilitation intervention for 16 weeks. Its precise composition was defined for each individual. All people with stroke were encouraged to use it on a regular basis (multiple times per week), with the intended dose depending on the nature of the intervention. For the cognitive exercise programme a dose of 300 s (5 min) of use every day was advised; for the physical exercise programme the recommended intensity and frequency could vary, depending on the individual’s situation and the nature of the exercises (at least 2–3 days of the week). With every training session, people with stroke needed to sign in only once, and were automatically linked to the different applications in their individualized programme. A training session could be performed at any location with enough space and internet access, which was mostly at home or in the rehabilitation facility. People with stroke could receive reminders to use the intervention, by email or text message. An email/telephone helpdesk was available during working hours.
3. Healthcare professionals received reports on the number/repetitions of exercises performed, in order to support the patient during conventional consultations and/or adapt the programme if necessary.
Assessments
Stroke and personal characteristics were derived from medical files, and health outcomes were collected with questionnaires. Questionnaires were available digitally and on paper, with reminders by telephone after 2 and 4 weeks. Use of the intervention was also recorded. Table SI shows an overview of the timing and content of assessments.
Sociodemographic and clinical characteristics
From the medical records, stroke type (ischaemic/haemorrhagic) and localization (right/left/other) were derived, and information on time between stroke and admission to rehabilitation (days), use of inpatient and/or outpatient rehabilitation and length of rehabilitation (days) was retrieved.
The admission questionnaire included living situation (alone or living with spouse/partner/children), educational level (low: up to and including lower technical and vocational training; medium: up to and including secondary technical and vocational training; high: up to and including higher technical and vocational training and university) and paid employment before stroke (yes/no). Depression and anxiety were measured by the Hospital Anxiety and Depression Scale (HADS (25)), including 7 items each on anxiety and depression (4-point Likert scale 0–3 points), yielding 2 subscale scores ranging from 0–21 (a higher score indicates a higher level of depression or anxiety).
Use of the intervention
The use of the applications was routinely recorded by each application and included: date, starting time and duration per exercise, type of exercise and, per exercise, the number of repetitions. For the activity tracker, the number of uploads was recorded. For an upload, the patient had to connect the activity tracker to a computer, after which the newly recorded activities were shown. A patient was defined as a user of the intervention if they had performed at least one exercise or one upload from the activity tracker. People with stroke who were registered and/or offered the intervention, but did not log into any of the applications, were defined as non-users.
Primary outcomes
The primary outcome was the Stroke Impact Scale (SIS), which included the following subscales: Physical Strength (4 items, minimal clinical important difference (MCID) 9.2 (26)), Memory (7 items), Feelings & emotion (9 items), Communication (7 items), Activities of Daily Living (ADL, 10 items, MCID 5.9), Mobility (9 items, MCID 4.5) and Meaningful Activities (T3 and T6 only, 8 items). The item scores range from 0 (very difficult) to 5 (not difficult), and the subscale scores from 0 to 100, with lower scores indicating more impact. The SIS has shown excellent internal consistency and good test–retest reliability (27). The subscale hand function was originally included in this study, but because of errors during the collection process, data were not valid.
Secondary outcomes
The EuroQol-5D-3L (EQ5D) measures HRQoL and comprises 5 subscales; mobility, self-care, usual activities, pain/discomfort, and anxiety/depression (28). Each dimension had 3 possible answer options: no problems, some problems, extreme problems. Utilities were calculated from the 5 subscales and the visual analogue scale (VAS), using the Dutch tariff (28). A utility of 1 reflects complete health, and –0.239 reflects death.
The 12-item Short-Form Health Survey (SF-12) was used at T3 and T6 to measure mental and physical health. Mental and physical scores can be computed, both scores ranging from 0 to 100 and higher scores indicating better QoL (29).
Fatigue was measured using the 9-item Fatigue Severity Scale (FSS), yielding a total score, being the mean of the 9 items (item scores and total score range 0–7), with higher scores indicating more fatigue (30). The FSS has good internal consistency, test–retest reliability and discriminative validity (31).
The Patient Activation Measure Short Form 13 (PAM-13) was used to assess people with stroke’s knowledge, skills and confidence for self-management (item scores 0 (totally disagree) to 5 (totally agree)), yielding a continuous total scale (0–100), higher scores indicating higher levels of patient activation. The shortened 13-item version is both reliable and valid (32).
Participation was measured with the Utrecht Scale for Evaluation of Rehabilitation-Participation (USER-P) (33), consisting of 3 scales (all range 0–100); Frequency of Activities (11 items), Restrictions (11 items), and Satisfaction with participation (10 items). The internal consistency and test–retest reliability in the rehabilitation population were satisfactory (33).
Physical activity was measured with the 7-item International Physical Activity Questionnaire Short Form (IPAQ-SF), regarding time spent on physical activities and sedentary time (days/h/min) during the last week (34).
Analyses
The target sample size was based on the ability to detect a change in score of 5 points on the SIS subscale mobility, with a standard deviation (SD) of 14 points (35). With an alpha of 0.05, 2-sided testing, power of 80%, and a drop-out rate of 20%, 296 people with stroke in total were needed to detect a significant difference.
Patient characteristics were described using means and SD, median with interquartile range (IQR) or numbers and percentages, depending on the type and distribution of the data. Normal distribution was checked by visual inspection and Kolmogorov–Smirnov tests. Characteristics of participants who did and did not complete the study, and characteristics of people with stroke in the CG and IG were compared by means of independent-samples t-tests, Mann–Whitney U tests, or Fisher’s exact tests.
Data were analysed on an intention-to-treat basis (ITT), meaning that all participants were included in the analysis. For the IG group, all people with stroke were considered, regardless of whether they received and/or used the intervention. In addition, all analysis were repeated, comparing all people in the CG with only those people in the IG who actually used the intervention (per-protocol analysis; PP).
Primary and secondary outcomes were compared between T0–T3 and T3–T6 within and between the CG/IG. The periods T0–T3 and T3–T6 were analysed separately, since those periods differ from each other in clinical activity; during the first period, people with stroke receive rehabilitation, where during the second period most people finished rehabilitation. Within-group analysis comprised paired t-tests, Wilcoxon signed-rank tests or McNemar tests, where appropriate.
Change scores between T0–T3 and T3–T6 were compared between the IG and CG by means of multivariate analysis of covariance (MANCOVA), while adjusting for baseline characteristics that differed significantly between the groups (age and type of rehabilitation). For both T0–T3 and T3–T6, 2 separate MANCOVAs were performed; 1 with 7 subscales of the SIS and 1 with all secondary outcome measures. In addition, differences in changes scores between ITT and PP were calculated.
To investigate differences over time, linear mixed models (LMM) were estimated for every primary and secondary outcome. These models take into account the correlation structure present in the data due to repeated measures within each patient, while accommodating for missing observations. The primary and secondary outcomes were entered in the model as dependent continuous variables, time as continuous variable and age (continuous) and type of rehabilitation (inpatient/outpatient/both) as control variables. Due to skewed distributions, power (squared) transformations were performed with EQ5D subscales (without VAS score) and logarithmic (log natural) transformations were performed with IPAQ scores. A model with a random slope and with unstructured covariance structure was estimated. For the USER-P, a model with only a random intercept was used, since a random slope model did not converge. Since not all outcome variables were normally distributed, LMM with bootstrapping was performed to obtain more accurate confidence intervals and to check whether results regarding significance differences between groups and change over time could be confirmed.
Data were entered and stored using Microsoft Access 2016 and analyses were performed using SPSS 25.0. p < 0.05 was considered significant.
During the study period, a total of 568 people with stroke met the inclusion criteria, of whom 318 (55.9%) gave informed consent and returned the baseline questionnaire (Fig. 2); 153 people with stroke in the control period and 165 in the intervention period. Of the 306 people who completed the 3-months follow-up, 159 people were included in the intervention group and 147 in the control group (96.2% completion rate), and of the 281 people who completed the 6-months follow-up, 150 people were included in the intervention group and 131 in the control group (88.3% completion rate). Participation was similar in the CG and IG. Baseline characteristics of people with stroke who completed the study and those lost to follow-up did not differ significantly (results not shown).
Fig. 2. Patient flow chart. eR: eRehabilitation.
Apart from SDs with respect to age (mean CG 58.6 (SD12.4); IG 62.6 (SD 10.5) years, p = 0.020), no SDs were found in the baseline characteristics or length of stay between people with stroke in the CG and IG (Table I). Compared with the CG, people with stroke who used the intervention more often had a combination of inpatient and outpatient rehabilitation (Table I, CG n = 55, 35.9%; users n = 30, 55.6%).
Table I. Characteristics of 318 stroke patients admitted to a rehabilitation centre in a period where conventional rehabilitation was offered (control group) or eRehabilitation was offered in addition (intervention group)
Use of the intervention in the IG
In this pragmatic trial, healthcare professionals delivered the intervention to 82 participants in the IG (50.0%), of whom 54 (65.8%) used it. Of the 54 users, 36 used the physical exercise applications, 19 the cognitive exercise application, and 15 the activity tracker. The median number of cognitive exercises performed was 14 (IQR 2–37), the median number of physical exercises was 10 for both applications (IQR Telerehabilitation 4–23, IQR Physitrack 3–51). The median number of uploads of the data of the activity tracker was 4 times (IQR 1–15). Fig. 3 shows that most users (85.2%) stopped using the intervention before T3. More details about the amount of use of the applications in the intervention and the influence of several implementation activities on this use are published elsewhere.
Primary outcomes
Regarding the changes within groups, the largest improvements occurred between the start of rehabilitation and T3, both for the CG and IG (Table II). Between T0 and T3, significant improvements in the SIS subscales, except for Feelings & emotion, were seen within both groups. Between T3 and T6, significant improvements were seen only within the IG, SIS subscales Memory and Meaningful activities. All mean changes score between T0 and T3 for both the IG and CG were below the MCID.
Regarding group differences, no significant differences between the IG and CG were seen between T0 and T3. However, between T3 and T6, the improvements were significantly greater in the IG than the CG for the SIS subscales Communication and Physical strength. Taking into account all time-points, no significant differences were seen between CG and IG. All mean changes in scores between T3 and T6 for both the IG and CG were below the MCID.
Secondary outcomes
Within groups, between T0 and T3, the EQ5D total score improved and the USER-P deteriorated significantly and the FSS improved significantly in the IG only (Table II). All other secondary outcomes showed no significant within-group changes. Between T3 and T6 only the USER-P Restriction and Satisfaction scores improved significantly within both groups. None of the between-group differences reached significance between T0 and T3, or T3 and T6 or T0 and T6.
Fig. 3. Use of Fast@home over time. Number of non-users (blue) and users (red) of Fast@home over time with measurement moments at T0 (start of rehabilitation), T3 (3 months after admissions) and T6 (6 months after admission).
Table II. Intention-to-treat analysis, comparing the control group (n = 153) with the intervention group (n = 165). Baseline scores and change score in mean difference (SD) for T0–T3 and T3–T6 and linear mixed models (LMM) for the whole period (T0–T6).
Per-protocol analysis
The PP analysis overall yielded similar results to the ITT analysis (Table III). No group differences were found between T0 and T3. Between T3 and T6, significantly greater improvements on the SIS subscales Communication and Physical strength were seen in the IG compared with the CG. In addition, differences in the change in scores of the SIS subscales Memory and Meaningful activities reached significance. All mean changes in scores of the PP analyses, of both IG and CG and between T0 and T3 and T3 and T6, were below the MCID.
To compare the results of the ITT analyses with the PP analyses, differences in changes in scores between ITT and PP were calculated (Table SII). The magnitude of improvements over time was larger for the users group (PP) compared with the total IG (ITT), both between T0 and T3 (for 8 of the 12 outcome measures) as well as between T3 and T6 (for 13 of the 17 outcome measures).
Table III. Per-protocol analyses, comparing the control group (n = 153) with the users of eRehabilitation (n = 54). Baseline score and change score in mean difference (SD) for T0–T3 and T3–T6 and linear mixed models (LMM) for the whole period (T0–T6).
This quasi-experimental pragmatic clinical study found that, with a comprehensive eRehabilitation intervention combining multiple applications offered alongside conventional stroke rehabilitation, some improvements were better maintained on the longer term than with conventional rehabilitation alone. Whereas people with stroke in both the control and intervention groups improved significantly during the first 3 months after admission on various domains of health, no significant differences between the groups were seen. In the second 3-month period, however, although further improvements within the groups were small, significant differences in favour of the intervention group were found in some of the outcome measures. These differences were even more pronounced if only the people with stroke actually using the intervention were taken into account, suggesting that the longer term differences may be attributed to the intervention.
The absence of an effect of eRehabilitation in the first 3 months after stroke is in line with the results of previous studies (11,13), concluding that those who received eRehabilitation reported additional exercise practice, but this did not directly translate into significant difference in the primary outcomes. The lack of short-term effect is probably related to the intensity of conventional rehabilitation in the first phase after stroke, with limited opportunities for further optimization of care. Moreover, irrespective of the treatment offered, in people with stroke the largest improvements are seen during the first 3 months following stroke (3, 36). Thus, the added value of the intervention might be under the threshold for clinical significance in that period.
In contrast to other studies, the current study also collected data during a follow-up period until 6 months after stroke, when institutional rehabilitation was finished for most people with stroke. Although improvements between 3 and 6 months were smaller compared with the first 3 months in both groups, there appeared to be an overall benefit of the intervention. This is striking, given the disappointingly low rates of participants being offered and using the intervention. Yet, as the differences were greater when only participants actually using the intervention were taken into account, it is possible that the effect was related to the eRehabilitation intervention. Although most participants stopped with the use of the applications after discharge, they were probably more likely to continue doing exercises at home and thereby maintaining or slightly improving the functional gains of the first 3 months. Although, in the longer term, some statistically significant differences were seen between the intervention and control groups, their clinical relevance remains uncertain. Overall, the mean changes in scores were relatively small. For the Physical Strength subscale, the only subscale with significant between-group differences and of which an MCID is known, the observed statistically significant difference did not exceed the MCID.
The overall improvements in people with stroke over time and the observed differences between the control and intervention groups were mainly seen in the SIS. The SIS appears to be a valuable instrument, reflecting the heterogeneity of the consequences of stroke on the individual patient. Nevertheless, problems in people with stroke vary widely, and evaluating cognitive, physical and mental health in all of them independently of the presence of such problem, may dilute the differences between patient groups. Future research should therefore also include patient-specific outcome measures, such as the COPM (37). Moreover, since the consequences of a stroke are so heterogeneous, more detailed analyses to evaluate changes in relevant domains (e.g. cognitive, motor, aphasia) for a specific subgroup of people with stroke are recommended. Unfortunately, the different subgroups in the current study would be too small for such investigations.
The relatively low proportion of people with stroke who received the intervention suggests that, although the implementation activities were employed as intended, this may not have led to the change that was predicted. A process evaluation, investigating which components of the implementation strategy actually worked and why with the implementation of the eRehabilitation intervention is currently underway. In this, the current study found that healthcare professionals did not deliver the eRehabilitation intervention to all patients, most likely due to physical, mental or cognitive limitations of the patients hampering engagement. Moreover, not all patients who received the intervention proceeded with it. This could be explained by the fact that those patients did not see the added value of continuation of usage after rehabilitation was finished, because they had already sufficiently recovered. Although the relatively low use can be seen as an important drawback, the current study reflects the situation in usual care and, in that respect, the rates of people with stroke who were actively offered the intervention may not be considered that unfavourable.
Study limitations
Although this study suggests the potential of eRehabilitation offered alongside conventional rehabilitation, the results must be interpreted with care, as the study has several limitations. First, this study did not have a randomized, controlled design, and people with stroke and healthcare professionals were not blinded regarding as to whether they had access to the intervention. Therefore, it cannot be ruled out that their awareness influenced the results, or that other, unknown developments in the rehabilitation centre occurring over time had an impact on the findings. Secondly, as mentioned previously, the numbers of people with stroke who were offered and actually used eRehabilitation were relatively low. Although the total number of people with stroke included met the requirements of the sample size calculation, this was not true if, in the intervention group, only people with stroke actually using the intervention were considered. Future studies investigating the effect of the use of eRehabilitation should develop a clear decision algorithm emphasizing the clinical decisions whether to deliver the intervention to a patient. In addition, the reasons for (non-)use of the eRehabilitation by patients should be registered, as well as what is actually prescribed and performed (both the applications and exercises within an application), which is necessary to calculate adherence. Thirdly, due to errors in data collection, the current study could not use the SIS hand function data. However, this study was performed in the clinical setting, reflecting the situation in which eRehabilitation will be used most.
This study indicates that a comprehensive eRehabilitation intervention, combing multiple applications and offered alongside conventional stroke rehabilitation, is beneficial regarding the maintenance of some of the improvements obtained directly after stroke. Further research should investigate the effect of a comprehensive eRehabilitation intervention using a parallel group design, and better monitoring of the delivery and use of the intervention. It would also be of interest to study partial replacement of conventional stroke rehabilitation by eRehabilitation applications.
The authors would like to thank all the patients and healthcare professionals who participated in this study.
Funding. Stichting Innovatie Alliantie supported this project financially (grant 2014-046PRO).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize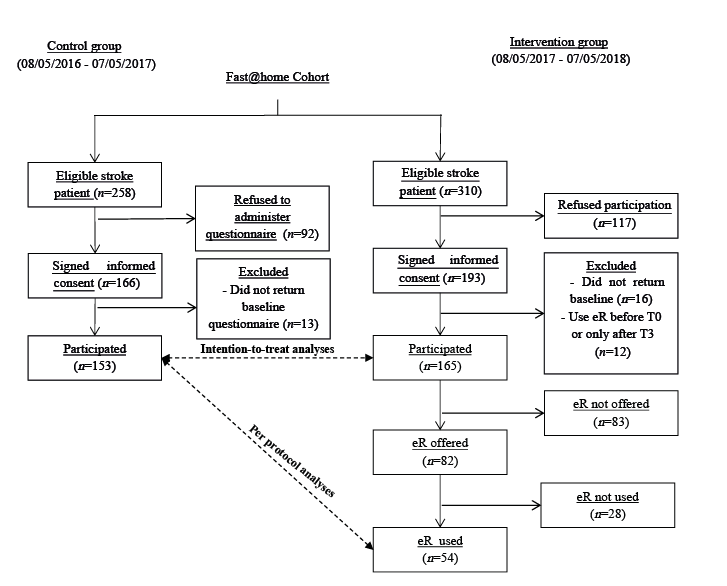 Click to show fullsize
Click to show fullsize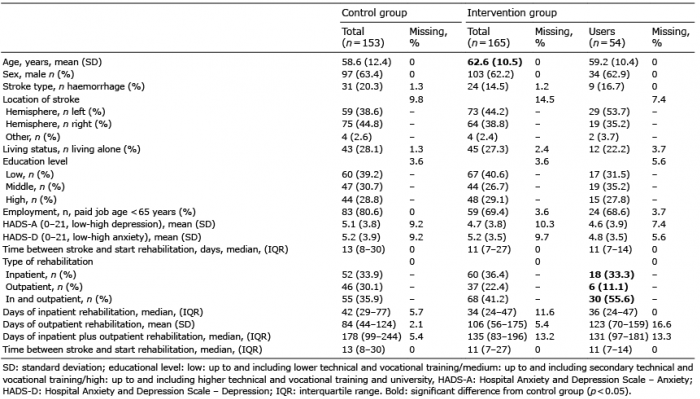 Click to show fullsize
Click to show fullsize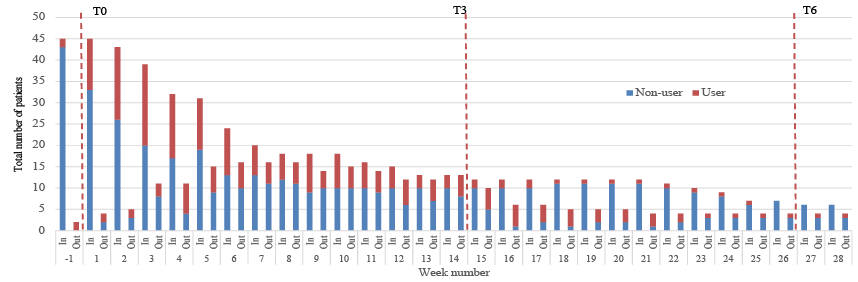 Click to show fullsize
Click to show fullsize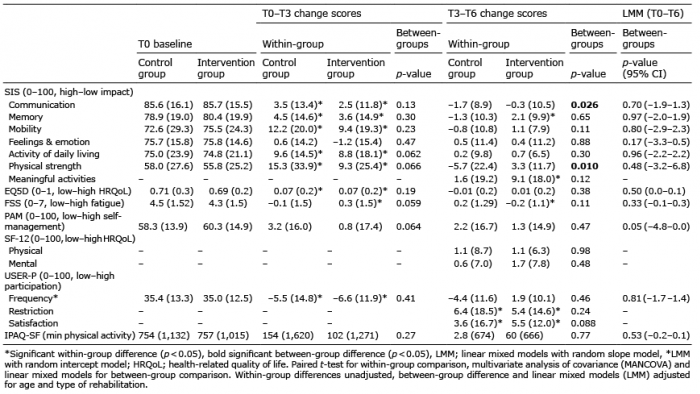 Click to show fullsize
Click to show fullsize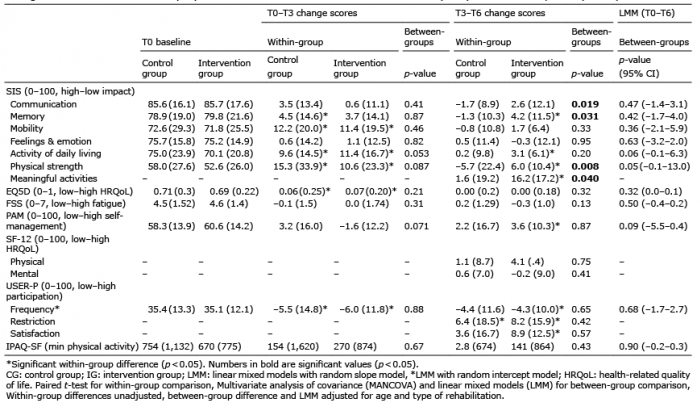 Click to show fullsize
Click to show fullsize