Yusuke Asano, Yoko Kano and Tetsuo Shiohara
Department of Dermatology, Kyorin University School of Medicine, 6-20-2 Shinkawa Mitaka, Tokyo, 181-8611, Japan. E-mail: yskasn@kyorin-u.ac.jp
Accepted August 27, 2007.



Yusuke Asano, Yoko Kano and Tetsuo Shiohara
Department of Dermatology, Kyorin University School of Medicine, 6-20-2 Shinkawa Mitaka, Tokyo, 181-8611, Japan. E-mail: yskasn@kyorin-u.ac.jp
Accepted August 27, 2007.
Sir,
Anti-tumour necrosis factor alpha (TNF-α) agents, such as infliximab, adalimumab and etanercept, are remarkably effective in the treatment of rheumatoid arthritis (RA), Crohn's disease and psoriasis vulgaris (1–4). Recent case reports have described the treatment of hidradenitis suppurativa (5) and acne conglobata (6) with infliximab. Regardless of the dramatic improvement in symptoms, it has been documented that various infections, such as tuberculosis, pneumocystis and aspergillosis, often develop among patients treated with these agents (7). We report here a patient with RA who developed atypical cutaneous tuberculosis following the administration of infliximab.
CASE REPORT
A 73-year-old woman presented with an erythematous induration on her left forearm. Because of RA, she had been treated with prednisolone (PSL) 10 mg daily and methotrexate (MTX) 6 mg weekly (three-divided-dose schedule over 24 h) for 5 years. Despite these therapies, her symptoms were not ameliorated. She was on no other medication and no past history of tuberculosis was noted. Subsequently, treatment with infliximab infusions was administered at baseline (week 0); weeks 2,6 and 14; and every 8 weeks thereafter in addition to PSL and MTX. Three months after the start of treatment with infliximab, she was febrile to over 38°C and developed an erythematous indurated lesion on her left forearm. Treatment with cefcapene pivoxil was initiated due to a strong suspicion of bacterial cellulitis; however, the lesion enlarged with redness and ulceration (Fig. 1). No lymphadenopathy was noted. Skin biopsy from the cutaneous lesion was performed. Histopathological findings showed epithelioid cell granulomas with prominent caseation necrosis and many Langhans’-type giant cells in the dermis (Fig. 2A). Numerous acid-fast bacilli were observed near the caseation necrosis in Ziehl-Neelsen staining of the specimen (Fig. 2B). Mycobacterium tuberculosis was detected by polymerase chain reaction (PCR) examination and confirmed by culture examination using the skin specimen. Despite no respiratory symptoms, chest X-ray and computed tomography demonstrated small nodules with bilateral infiltrates in the chest, compatible with pulmonary tuberculosis. M. tuberculosis was detected by PCR examination of the sputum. She was diagnosed as having both cutaneous and pulmonary tuberculosis. Infliximab was discontinued immediately; quadruple anti-tuberculosis therapy, comprising isoniazid, rifampicin, pyrazinamide and ethambutol, was started. After 5 months of anti-tuberculosis therapy, the cutaneous lesion gradually resolved and pulmonary lesions cleared.
Fig 1. Erythematous indurated lesion with ulcer on the left forearm.

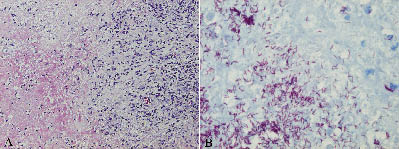
Fig 2. (A) Epithelioid cell granuloma with prominent caseation necrosis (H&E stain: ×40). (B) Numerous acid-fast bacilli in the dermis (Ziehl-Neelsen stain: ×100).
DISCUSSION
TNF-α is a pro-inflammatory cytokine that is involved in the immune protection against infection. It plays a central role in the immune response against M. tuberculosis. Indeed, TNF-α contributes to the formation of granulomas that isolate bacilli and prevent their dissemination (8). In addition, recent articles have demonstrated that anti-TNF-α agents have the potential to suppress pro-inflammatory cytokine production by the induction of regulatory T cells (9, 10). One of the anti-TNF-α agents, infliximab, is a chimeric monoclonal antibody with high binding affinity and specificity for TNF-α; it has the ability to cross-link TNF-α molecules for up to 2 months. Previous documents showed that infliximab is well known to increase the risk of the onset of tuberculosis.
Although the tuberculosis infection in this present case developed during concomitant immunosuppressive treatment, the temporal association between the onset of cutaneous lesion strongly suggests that the infection was induced by the introduction of infliximab. Indeed, the previous article by Keane et al. (7) demonstrated that the tuberculosis infections following administration of infliximab in patients with recalcitrant RA treated with PSL and MTX developed approximately 12 weeks after the initiation of infliximab, as in our case. Additionally, more than half of the patients had extrapulmonary manifestations of tuberculosis, including lymph node disease, peritoneal disease, pleural disease, and meningeal disease.
Tuberculosis infections associated with infliximab tend to reveal unusual clinical manifestations with acute onset. Lung tuberculosis shows atypical manifestations, such as high fever and strong respiratory symptoms mimicking bacterial pneumonia, and disseminated small nodules on X-ray and computed tomography (11). Our present case developed an atypical cutaneous manifestation of tuberculosis infection that resembles bacterial cellulitis. The cellulitis-like cutaneous tuberculosis has rarely been observed in previous reports. A similar cutaneous finding has been observed only in a diabetic patient treated with chronic systemic corticosteroids for arthralgia (12).
The mechanism by which an acute inflammatory cutaneous manifestation of tuberculosis emerged in our present case has not been elucidated. In view of the observation that similar atypical manifestations of tuberculosis infection occasionally developed in patients with acquired immune deficiency syndrome after starting highly active antiretroviral therapy (HAART), it is likely that the acute cellulitis-like inflammation might have resulted from recovery of immune responses against latent M. tuberculosis that were suppressed during anti-TNF-α treatment (13). Indeed, this patient developed cutaneous tuberculosis lesion 3 months after the start of treatment with infliximab. This is consistent with the time period required for restoration of the immune response.
Conflict of interest: None declared.
REFERENCES
1. Maini R, St Clair EW, Breedveld F, Furst D, Kalden J, Weisman M, et al. Infliximab (chimeric anti-tumor necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomized phase III trial. ATTRACT Study Group. Lancet 1999; 354: 1932–1939.
2. Reich K, Nestle FO, Papp K, Ortonne JP, Evans R, Guzzo C, et al. Infliximab induction and maintenance therapy for moderate-to-severe psoriasis: a phase III, multicentre, double-blind trial. Lancet 2005; 366: 1333–1335.
3. Poulalhon N, Begon E, Lebbe C, Liote F, Lahfa M, Bengoufa D, et al. A follow-up study in 28 patients treated with infliximab for severe recalcitrant psoriasis: evidence for efficacy and high incidence of biological autoimmunity. Br J Dermatol 2007; 156: 329–336.
4. Kalb RE, Gurske J. Infliximab for the treatment of psoriasis: clinical experience at the State University of New York at Buffalo. J Am Acad Dermatol 2005; 53: 616–622.
5. Lebwhol B, Sapadin AN. Infliximab for the treatment of hidradenitis suppurativa. J Am Acad Dermatol 2003; 49: 275–276.
6. Shirakawa M, Uramoto K, Harada FA. Treatment of acne conglobata with infliximab. J Am Acad Dermatol 2006; 55: 344–346.
7. Keane J, Gershon S, Wise RP, Mirabile-Levens E, Kasznica J, Schwieterman WD, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent. N Engl J Med 2001; 345: 1098–1104.
8. Gardam MA, Keystone EC, Menzies R, Manners S, Skamene E, Long R, et al. Anti-tumor necrosis factor agents and tuberculosis risk: mechanism of action and clinical management. Lancet Infect Dis 2003; 3: 148–155.
9. Nadkarni S, Mauri C, Ehrenstein MR. Anti-TNF-α therapy induces a distinct regulatory T cell population in patients with rheumatoid arthritis via TGF-β. J Exp Med 2007; 204: 33–39.
10. Chen X, Zhou B, Li M, Deng Q, Wu X, Le X, et al. CD4(+)CD25(+)FoxP3(+) regulatory T cells suppress Mycobacterium tuberculosis immunity in patients with active disease. Clin Immunol 2007; 123: 50–59.
11. Imaizumi K, Sugishita M, Usui M, Kawabe T, Hashimoto N, Hasegawa Y. Pulmonary infectious complications associated with anti-TNF α therapy (infliximab) for rheumatoid arthritis. Int Med 2006; 45: 685–688.
12. Lee NH, Choi EH, Lee WS, Ahn SK. Tuberculous cellulitis. Clin Exp Dermatol 2000; 25: 222–223.
13. Shelburne SA, Hamill RJ. The immune reconstitution inflammatory syndrome: AIDS Rev 2003; 5: 67–79.

